Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
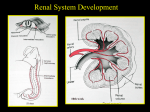
Chapter 5. Anatomy and Embryology 부산백병원 산부인과 R3 강영미 Pelvic Viscera Embryonic development Female urinary and genital tract Closely related, anatomically and embryologically Embryologic urinary system ; important inductive influence on developing genital system Anomalies in one system are often mirrored by anomalies in another system Embryonic development Urinary system, internal reproductive organs and external genitalia Develop synchronously at an early embryologic age(table 5.6) Urinary system Kidney, Renal collecting system, Ureters Kidney, renal collecting system and ureters from longitudinal mass of mesoderm(nephrogenic cord) Mesonephric(Wolffian) duct Singular importance for the following reasons Grows caudally in developing embryo to open an excretory channel into the primitive cloaca and outside world Serves as starting point for development of the metanephros which becomes definitive kidney Differentiates into the sexual duct system in male Although regressing in female fetuses, inductive role in development of the paramesonephric or mullerian duct Metanephros Development of metanephros 그림 13-8 Bladder and Urethra Cloaca Genital system development Genital system In embryologic stage, early genital system Indistinguishable between two sexes Known as “ indifferent stage” of genital development Mesodermal epithelium, mesenchyme and primordial germ cell Internal reproductive organs Primordial germ cells 1. Mullerian duct Paramesonephric or mullerian ducts Form lateral to mesonephric ducts Grow caudally and then medially to fuse in midline Contact urogenital sinus in region of the post. urethra at slight thickening known as sinusal tubercle Male fetus TDF Results in degeneration of gonadal cortex and differentiation of the medullary region of the gonad into Sertoli cells Sertoli cells Secrete glycoprotein known as anti-mullerian hormone(AMH) Cause regression of paramesonephric duct system in male embryo Signal for differentiation of Leydig cells from the surrounding mesenchyme Male fetus Leydig cells Produce testosterone,dihydrotestosterone with 5areductase Testosterone Responsible for evolution of mesonephric duct system into vas deferens, epididymis, ejaculatory ducts and seminal vesicle At puberty, leads to spermatogenesis and changes in primary and secondary sex characteristics DHT Results in development of the male external genitalia and prostate and bulbourethral glands Female fetus In the absence of TDF, medulla regresses and cortical sex cords break up into isolated cell clusters(primordial follicles) in the absence of AMH & testosterone, Mesonephric duct system degenerates Then, paramesonephric duct system develops Inf. fused portion Uterovaginal canal -> uterus and upper vagina Cranial unfused portions Open into celomic cavity(future peritoneal cavity) Fallopian tubes 3. Accessory genital glands Female accessory genital glands Develop as outgrowths from urethra(paraurethral or Skene) and definitive urogenital sinus(greater vestibular or Bartholin) Ovaries first develop in the thoracic region, but arrive in pelvis by complicated process of descent This descent by differential growth ; under the control of a ligamentous cord called the gubernaculum Genital system ; 3. Accessory genital glands Gubernaculum External genitalia Genital system abnormalities Congenital defects in sexual development, usually arising from a variety of chromosomal abnormalities, tend to present clinically with ambiguous external genitalia Known as intersex conditions or hermaphroditism Classified according to the histologic appearance of the gonads (1) True hermaphroditism Individuals with true hermaphroditism Have both ovarian and testicular tissue Most commonly as composite ovotestes Occasionally with an ovary on one side and a testis on the other In the latter case, a fallopian tube and single uterine horn may develop on the side with the ovary ∵ absence of local AMH Extremely rare condition (2) Pseudohermaphroditism In individuals with pseudohermaphroditism, Genetic sex indicates one gender External genitalia has characteristics of the other gender Caused either by abnormal levels of sex hormones or abnormalities in the sex hormone receptors (2) Pseudohermaphroditism Males with pseudohermaphroditism Genetic males with feminized external genitalia Hypospadias(urethral opening on the ventral surface of the penis) Incomplete fusion of the urogenital or labioscrotal folds ; m/c manifesting sx. Females with pseudohermaphroditism Genetic females with virilized external genitalia Clitoral hypertrophy Some degree of fusion of the urogenital or labioscrotal folds Genital Structures Vagina Hollow fibromuscular tube extending from the vulvar vestibule to the uterus In dorsal lithotomy, directed posteriorly toward the sacrum In upright position, almost horizontal Spaces between the cervix and vagina ; ant, post, and lateral vaginal fornices Post. vaginal wall ; about 3 cm longer than the ant. wall ∵ vagina is attached at a higher point posteriorly than anteriorly Vagina Post. vaginal wall ; separated from post. cul-de-sac and peritoneal cavity by the vaginal wall and peritoneum This proximity ; clinically useful Culdocentesis Intraperitoneal hemorrhage, pus, other intraabdominal fluid Posterior colpotomy As an adjunct to laparoscopic excision of adnexal masses Cervix Endocervical canal About 2-3cm in length, opens proximally into the endometrial cavity at the internal os In early childhood, during pregnancy, or with oral contraceptive use, Columnar epithelium may extend from the endocervical canal onto the exocervix -> eversion or ectopy Cervical mucus production Under hormonal influence Around the time of ovulation - profuse, clear, thin In the postovulatory phase of the cycle ; scant and thick mucus Corpus At birth, cervix and corpus are about equal in size In adult women, corpus has grown to 2-3 times the size of the cervix Position ; flexion and version Flexion - angle between the long axis of the uterine corpus and cervix Version - angel of the junction of the uterus with the upper vagina Corpus Divided into several different regions ; Isthmus or lower uterine segment The area where the endocervical canal opens into the endometrial cavity Uterine cornu On each side of the upper uterine body, funnel-shaped area receives the insertion of the fallopian tubes Fundus Uterus above this area(cornu) Fallopian tubes Fallopian tubes and ovaries ; referred to as the adnexa Vary in length from 7 to 12 cm Function Ovum pickup Provision of physical environment for conception Transport and nourishment of the fertilized ovum Fallopian tubes Divided into several regions ; Interstitial Narrowest portion of the tube, lies within the uterine wall and forms the tubal ostia at the endometrial cavity Isthmus Narrow segment closest to the uterine wall Ampulla Larger diameter segment lateral to the isthmus Fimbria(infundibulum) Funnel-shaped abdominal ostia of the tubes Ovaries Paired gonadal structures that lie suspended between the plevic wall and the uterus by the infundibulopelvic ligament laterally and uteroovarian ligament medially Varies in size with measurements up to 5*3*3cm Consists of a cortex and medulla Cortex - specialized stroma and follicles Medulla - primarily of fibromuscular tissue and blood vessels Urinary tract Ureters 25cm in length Totally retroperitoneal in location Pathway of lower half of each ureter Traverses the pelvis after crossing the common iliac vessels at their bifurcation, just medial to the ovarian vessels Descends into the pelvis adherent to the peritoneum of the lateral pelvic wall and the medial leaf of the broad ligament Enter the bladder base anterior to the upper vagina, traveling obliquely through the bladder wall P. 772 Bladder divided into two areas ; Base of the bladder Consists of the urinary trigone posteriorly and a thickened area of detrusor anteriorly Trigone - two ureteral orifices and opening of the urethra into the bladder Receives a-adrenergic sympathetic innervation Is the area responsible for maintaining continence Dome of the bladder Parasympathetic innervation Is responsible for micturition Urethra Female urethra ; about 3 to 4 cm in length Extends from the bladder to the vestibule, traveling just anterior to the vagina Lined by nonkeratinized squamous epithelium that is responsive to estrogen stimulation Contains as inner longitudinal layer and outer circular layer Abdominal Wall Abdominal wall 1. Skin 2. Muscles Five muscles and their aponeuroses(fig 5.16) 3. Fascia ; (1) Superficial fascia Consists of two layers Camper fascia Most superficial layer, which contains a variable amount of fat Scarpa fascia Deeper membranous layer continuous in the perineum with colles fascia(superficial perineal fascia) and with deep fascia of the thigh(fascia lata) 3. Fascia ; (2) Rectus sheath Aponeuroses of the external and internal oblique and the transversus abdominis ; Combine to form a sheath for the rectus abdominis and pyramidalis, fusing medially in the midline at the linea alba and laterally at the semilunar line(fig 5.16) 3. Fascia ; (3) Transversalis fascia and endopelvic fascia Firm membranous sheet on the internal surface of the transversus abdominis muscle Like peritoneum, divided into a parietal and a visceral component Transversalis fascia Continues along blood vessels and other structures leaving and entering the abdominopelvic cavity Contributes to the formation of the visceral (endopelvic) pelvic fascia Pelvic fascia Invests the pelvic organs and attaches them to the pelvic side walls, thereby playing a critical role in pelvic support Perineum Situated at the lower end of the trunk between the buttocks Its bony boundaries Lower margin of the pubic symphysis anteriorly Tip of the coccyx posteriorly Ischial tuberosities laterally Diamond shape of the perineum Divided by imaginary line joining the ischial tuberosities immediately in front of the anus, at the level of the perineal body, into an ant. urogenital and a post. anal triangle(fig 5.18)