Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
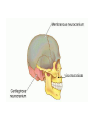
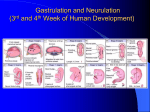
EMBRYOLOGY YR1 SLT EMILY BURTENSHAW Introduction to embryology: • Basic concepts and principles • Influences on the growth and development of the embryo • Critical period concept • The first 8 weeks: organogenesis • Development of the nervous system, skull, face, palate, pharynx and tongue • Prenatal development: 3 stages of unequal length. • Germinal stage: days 1 to 14 ie from conception to implantation • Embryonic stage: begins at implantation approximately 2 weeks after conception and continues through weeks 3 to 8 (the period oforganogenesis ) • The Foetal Stage: from 9th week to the birth (40 weeks from last period, or 38 weeks from fertilisation) • Organs grow and continue differentiation • Increase in weight Critical period: What can affect prenatal development? • • • • Chromosomal and genetic factors Teratogens: maternal disease, drugs Mutagens: radiation Other maternal influences on development: • Diet, age, chronic illness, environmental hazards and maternal emotions Chromosomal abnormalities • 23 pairs of chromosomes • Over 50 different chromosomal abnormalities • Too many chromosomes • Too few chromosomes • Vast majority of chromosomal abnormalities are lethal (spontaneous abortion) Genetic disorders • Through dominant or recessive genes • Eg Cystic fibrosis • Phenylketonuria (PKU) – Lack of enzyme to digest food containing amino acid phenylalanine (e.g.milk) – Phenylpyruvic acid accumulates in the body and attacks the developing nervous system – Hyperactivity; learning difficulties – Test routinely given at birth – Treatment: diet Pregnancy testing • Human chorionic gonadotrophin • Secreted by chorion of the placenta from day 8 post fertilisation – Detected by test kits 14 days after conception Foetal assessment: • Chorionic villus sampling (weeks 1012) • Amniocentesis (weeks 14-16 plus 4 weeks for results) • Ultrasound (16-20 weeks) Iterative processes in embryological development: • Cell division (proliferation) • Cell adhesion • Separation of cell sheets to form cavities • Cell migration • Cell differentiation • Cell induction Birth defects: • Cell proliferation : embryo/organ system vulnerable to genetic or environmental factors • Cell migration: cells move into position; can be affected by matrix through which they travel • Cell differentiation: cells assume their ultimate form or phenotype – less vulnerable to insult Carnegie stages Three sources of embryonic stem cells: Day 14: GASTRULATION: a process that lasts 2 weeks caudal DAY 15: 0.2mm Buccopharyngeal membrane LEFT RIGHT Primitive node Primitive streak rostral The fate of the 3 germ layers: • Ectoderm: CNS, PNS, epidermis, hair, nails, sensory epithelium (nose, ear, eye) • Mesoderm: part of skull, muscles, vertebrae, urogenital system, serous membranes, body wall, limbs • Endoderm: gut tube and its derivatives; glands, lungs, liver, gall bladder, pancreas Birth defects originating during gastrulation: • situs inversus • Teratoma (formed from epiblast cells – contain hair, skin, bone, liver etc cells) • Caudal dysgenesis Weeks 3 to 4 • Formation of the neural and gut tubes • Embryo transformed from a trilaminar disc into something more recognisable! Neurulation: • Formation of neural plate • Elevation and curling of lateral edges • ‘zippering’ and formation of the neural tube Formation of the notochord: Folding of the embryo: • Dorsal surface – formation of the neural tube – ‘zippering’ effect – cervical first, then caudally • Ventral surface – formation of gut tube and body cavities • Body stalk – eventual umbilical cord epic neurulation neurulation video Final destination neural crest cells: • • • • • • • • • • • • • Connective tissue and bones of the face and skull C cells of thyroid gland Septum of the heart Odontoblasts Dermis in the face and neck Dorsal root ganglia Sympathetic chain and pre-aortic ganglia Parasympathetic ganglia of the GI tract Adrenal medulla Schwann cells Glial cells Arachnoid and pia mater melanocytes Formation of the umbilical ring: • Proliferation and differentiation of mesoderm • Causes ventral folding along sides of embryonic axis; amnion surrounds embryo • Formation of gut tube • Brain grows • Head and tail folding • ‘purse strings’ effect • http://www.embryo.nl/anim%20craniocaud ale%20kromming.mv Ontogeny replicates phylogeny Neural crest cells… • • • • Leave cranial area BEFORE fold closure Leave the spinal area AFTER closure Start as ectoderm Change to loose connective tissue (called mesenchyme) • Migrate to destination • Differentiate into a wide variety of cell types In the head and neck region: • Form ganglia of the cranial nerves • Connective tissue and some of the bones of the skull and face • Dermis in the face and neck • Odontoblasts • Arachnoid and pia mater • Glial cells Fate of the mesoderm: • Paraxial mesoderm forms paired somites from occiput caudally along the length of the neural tube • In the head region, somitomeres form part of skull, muscles, vertebrae, and dermis of the skin. Development of the Skull: • Neurocranium (protective covering of the brain) derived from paraxial mesoderm – Membranous portion (flat bones) – Cartilagenous portion = Chondrocranium (base of the skull) • Viscerocranium (skeleton of the face – the ‘middle third’ - & including the mandible) derived entirely from neural crest cells viscerocranium Development of the brain vesicles: • • • • • Cranial end of neural tube expands Neural tube closure complete in week 4 Brain vesicles form the future brain Anterior vesicle: prosencephalon This subdivides: telencephalon (future cerebral hemispheres) and diencephalon (optic and thalamic tissues and other structures) Primary Brain Vesicles (rhombencephalon) Further development of the NS • The nervous system continues to develop and changes occur up until the early 20’s • The main changes include: • Myelination • Formation of synapses • Synaptic pruning • Apoptosis Synaptic pruning: • Role of microglia is to…..? • They also pluck off or ‘prune’ some of the synapses between neurons • In conjunction with apoptosis of neurons, ensures that only the mostused ie strongest connections, remain • Keeps the brain operating efficiently Implications for SLT: • Aberrant synaptic pruning may be at the root of MND, MS • AD – by the time it is identified, people have lost over HALF their synapses • Children with ASD have increased cerebral volume, ? ? have not undergone the same extent of synaptic pruning? Myelination: • Starts late in embryonic development and continues into adolescence/early adulthood • Forebrain the last part to complete myelination • Q What is the function of the myelin sheath? THE SPINAL CORD • Extends from the foramen magnum to the level of the second lumbar vertebra. • Shorter than the vertebral column because it does not grow as rapidly during embryonic development. • Because the spinal cord is shorter, spinal nerves do not always exit the vertebral column at the same level as their origin in the spinal cord. By the end of the 4th week: • Neural folds have closed • Head region distinguished by presence of 3 brain vesicles • Lens and otic placodes for eye and ear development; • Primitive oral cavity (stomatodeum) • 3 pairs of pharyngeal arches Formation of the pharyngeal arches: • Neural crest material grows from the rhombencephalic region (rhombomeres) • Migrates and forms 6 paired bands • These form the pharyngeal arches • Each is accompanied by its own artery, nerve and cartilage First arch deformities: • • • • Micrognathia Cleft palate (indirectly) Conductive hearing loss External ear malformations formation of the face formation of the palate detailed formation of the face