Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
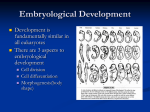
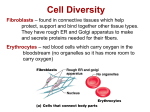
• • • • • scrotum = supportive structure for the testes consists of loose skin and superficial fascia that hangs from the root of the penis externally- single pouch separated at the midline by a raphe internally – divided by a scrotal septum into two sacs each containing 1 testis the septum = dartos muscle (smooth muscle) + superficial fascia – • • • dartos is also found in the subcutaneous portion of the scrotal skin each testis is associated with a cremaster muscle – skeletal muscle that is a continuation of the internal oblique exterior location of the testis ensures its internal temperature is at least 2 to 3C lower than the body core contraction of the muscles lifts the scrotal sac closer to the trunk of the body and warms it -testis: develop internally near the kidneys and descend through the inguinal canal during the latter half of the seventh month gestation -covered by several protection membranes 1. tunica vaginalis – serous membrane derived from the peritoneum, forms during the descent of the testes 2. tunica albuginea – internal to the TV -extends inward to divide the testes into lobules (200-300) -each lobule contains 1 to 3 coiled seminiferous tubules for sperm production - each seminiferous tubule is lined with epithelium that produce sperm - contained within that epithelium are germ cells for sperm production – known as spermatogenic cells or spermatogonia • embedded among the spermatogenic cells of the seminiferous tubules are large cells called Sertoli cells – sustenacular cells – surround the spermatogenic cells and the developing spermatocytes and spermatids – produces numerous chemicals involved in spermatogenesis – some of these chemicals result in a blood-testis barrier – this barrier prevents an immune response against the spermatogenic cells’ surface antigens which are recognized as they develop as being foreign – other chemicals - cytokines and growth factors that mediate spermatogenesis • anti-Müllerian hormone (AMH) - secreted during the early stages of fetal life • inhibin and activins - secreted after puberty, and work together to regulate FSH secretion • androgen binding protein - faciliate spermatogenesis and sperm maturation • between adjacent seminiferous tubules are the interstitial cells or Leydig cells – for the production of testosterone (androgen) – can be a site for the development of testicular cancer - along with Sertoli cells – androgen = hormone for the development of masculine characteristics Spermatogenesis • • • • • • sperm development – from sperm stem cells called spermatogonia the maturing sperm can be found toward the lumen of the seminiferous tubule, the spermatogonia in the most mature = sperm cells or spermatozoa 1. some spermatogonium break away from the basement membrane of the seminiferous tubule 2. each spermatogonium forms two primary spermatocytes (2n = 46) 3. primary spermatocyte starts meiosis I - the formation of secondary spermatocytes (n = 23) – • however despite having 23 chromosomes, these chromosomes are still comprise of two chromatids 4. completion of meiosis II and formation of 4 spermatids (n) – 23 chromosomes each made up of one chromatid Spermatogenesis • spermiogenesis – last stage of spermatogenesis • development of spermatids into a sperm cell – spherical spermatids transform into elongated sperm containing an acrosome and bearing a flagellum Mitosis Meiosis I Meiosis II Spermiogenesis interstitial cell Sperm • three functions – 1. reach the oocyte – 2. penetrate the oocyte – 3. donate its chromosomes to the oocyte • major parts – 1. head: contains the nucleus with 23 highly condensed chromosomes (one chromatid) – 2. acrosome: covers the anterior 2/3 of the head • specialized organelle • contains digestive enzymes to dissolve the protective barriers surrounding the oocyte – 3. midpiece • contains mitochondria arranged in a spiral • also contains a pair of centrioles for the production of the microtubules for the tail – 4. tail or flagellum • made up of microtubules • principal piece – longest portion of the tail • end piece – terminal portion of the tail • 300 million made each day • 60 um long -release of gonadotropic releasing hormone (GnRH) from the neurosecretory cells of the hypothalamus -GnRH travels to the anterior pituitary via the hypophyseal portal system -in response - the gonadotrophs of the anterior pituitary gland produce and release the 2 gonadotropins 1. Follicle Stimulating Hormone - FSH 2. Leutenizing Hormone - LH 1. Follicle stimulating hormone – works with testosterone to stimulate spermatogenesis -synergistic action by FSH and testosterone on the Sertoli cells -FSH binds to the surface of the Sertoli cell -testosterone and its receptor is internalized by the Sertoli cell - together FSH + testosterone results in secretion of androgen-binding protein by Sertoli cells -ABP binds to testosterone and promotes better spermatogenesis -GnRH and FSH release are both inhibited by the release of inhibin (by the Sertoli cells) 2. Leutinizing hormone - stimulates male hormone production by the Leydig cells -testosterone synthesized from cholesterol in the testes -testosterone stimulates the final stages of spermatogenesis -suppresses GnRH and LH synthesis by negative feedback Testosterone • testosterone and DHT both bind to same receptors – • • receptors are found within the nuclei of the target cells targets – bone, muscle effects – 1. prenatal development • stimulates the male pattern of the reproductive system – gonads develop during the 5th week of gestation from two sets of ducts: 1) Wolffian ducts (males) and 2) Mullerian ducts (females) – therefore the embryo has the potential to develop into either sex – BUT “maleness” determined by a gene called SRY – sex determining region of the Y chromosome – SRY protein expression induces differentiation of Sertoli cells – Sertoli cells secrete anti-Mullerian Hormone– apoptosis within the Mullerian ducts which inhibits the development of female structures -in response to hCG – Leydig cells begin to synthesize testosterone -testosterone stimulates development of the epididymus, vas deferens, ejaculatory duct and seminal vesicle • DHT stimulates development of external genitalia – – – – development around the 8th week from the genital tubercle (both males and females) – comprised of a urethral groove and two labiosacral swellings elongation of part of the genital tubercle into the penis labiosacral swellings - scrotum • testosterone is converted in the brain to estrogens – development of certain brain regions in males – 2. development of male sexual characteristics – 3. development of sexual function • male sexual behavior • spermatogenesis • libido in both males and females – females – androgen release by the adrenal cortex – 4. stimulation of anabolism • stimulate protein synthesis Testosterone -pressure generated by the Sertoli cells pushes the sperm into a series of ducts within the testes that end up as the epididymis -within the epididymis is the ductus epididymis -also made up of a head, body and tail portion -site of sperm maturation – acquire mobility (14 days) -helps propel sperm into the: -vas (ductus) deferens: conducting tube from testis to urethra -connects to the tail of the epididymis -connects the testes to the urethra -made up of a pseudostratified columnar epithelium with a lamina propria connective tissue plus three layers of smooth muscle -contractions of these muscular layers propel the sperm Reproductive Ducts -spermatic cord supports the vas deferens + blood vessels (testicular artery and the pampiniform venous plexus), lymphatic vessels, the cremaster muscle and autonomic nerves -passes through the inguinal canal • ejaculatory duct – forms from the union of the seminal vesicle and the end of the vas deferens – pass through the prostate gland and terminate in the urethra • urethra: 3 sections: • A. prostatic - runs through the prostate • connects to ducts from the prostate and to the ejaculatory duct • B. membranous - between prostate and penis • -through the muscles of the perineum – urogenital diaphragm • C. spongy - through the erectile tissue of the penis Male reproductive glands • • • • • • • • • • -glands: seminal vesicles, prostate, bulbourethral glands -produce fluid that combine with sperm to make semen -semen: alkaline, activates sperm cells 1. prostate: surrounds the urethra -forms as an outgrowth of the urethra along with the bulbourethral glands -secretes a thin, milky fluid that enhances sperm motility and neutralizes vaginal fluid 2. seminal vesicles: connect to urethra via the ejaculatory ducts -secretes an alkaline fluid that contains sugars and prostaglandins (stimulates uterine contractions) 3. bulbourethral glands: 2 glands behind the prostate -secrete a fluid that lubricates the penis -conveys urine and semen -body is found externally -body is comprised of two tissue types of erectile tissue surrounded by connective tissue A. corpus cavernosum - large spaces B. corpus spongiosum - smaller spaces -surrounds the urethra -root of the penis is attached to the pelvis -corpus spongiosum enlargens at the tip - glans penis (sensory receptors) -glans penis covered with a loose fold of skin = prepuce -ovary: production of egg -surface is covered with a germinal epithelium (simple epithelium) – does NOT give rise to the ova! -next layer is = tunica albuginea – dense irregular connective tissue capsule -outer cortex- granular tissue due to the presence of tiny ovarian follicles - inner medulla - connective tissue with blood & lymphatic vessels and nerves Oogenesis and Follicular Development • • • begins before birth early fetal development – primordial germ cells from the yolk sac migrate into the developing ovaries differentiate to form oogonia (diploid stem cells) – • • undergo mitosis to produce millions of germ cells most of the germ cells degenerate by atresia a few develop further into primary oocytes – entered prophase I of meiosis – – – – – surrounded by a layer of follicular cells = primordial follicle continue to develop into primary follicles at birth – 200,000 to 2,000,000 follicles within the ovary at puberty 40,000 are still present 400 will develop further (rest undergo atresia) -release of FSH and LH each month causes the development of one primary oocyte into a secondary oocyte -development of a few primordial follicles into primary follicles (only one will continue until ovulation) -primary follicle – primary oocyte surrounded by several layers of epithelial cells called granulosa cells -develops a clear glycoprotein layer between the oocyte and the granulosa cells – zona pellucida -the outermost granulosa cells contact a basement membrane which begins to develop into two layers (theca layers) -now known as the secondary follicle -secondary follicle begins to accumulate fluid in the center of the follicle (antrum) -innermost granulosa cells firmly attaches to the zona pellucida = corona radiata -becomes larger and turns into the tertiary or mature Graafian follicle -completes meiosis I – two haploid cells -these haploid cells are uneven in size but each have 23 chromosomes (two chromatids each - 46) -smaller cell – first polar body (discarded nuclear material) -larger cell – secondary oocyte -receives most of the cytoplasm and has 23 chromosomes -stops at metaphase II -ovulated Oogenesis and Follicular Development • ovulation – expulsion of the secondary oocyte into the pelvic cavity with the first polar body and corona radiata • fertilization – union of egg and sperm – penetration of the sperm into the secondary oocyte results in the resumption of meiosis II – the secondary oocyte splits again into two cells of unequal size (n) – larger one is called the ovum and the smaller one is the second polar body – combination of the ovum and the sperm results in the formation of the zygote – the first polar body splits also into two haploid cells – therefore meiosis of the primary oocyte produces one haploid ovum and three haploid polar bodies that degenerate • uterus: receives and nourishes the embryo • -comprised of a body, a curved portion (fundus) and the cervix • • • -uterine wall outer perimetrium, muscular myometrium and inner endometrium -endometrium: mucosal layer covered with epithelium -rich blood supply, sloughed off during menstruation • uterine tubes (Fallopian tubes): conduction of egg from ovary to uterus • -expands at end near the ovary = infundibulum with fimbrae (fingers) for the • “catching” of the released egg -lined with a mucosal layer and columnar epithelium with cilia -are also cells with microvilli rather than cilia – produce a nutritive fluid for the egg • cervix: projects into the vaginal canal Female Reproductive Cycle • two cycles – 1. ovarian: during and after the maturation of the oocyte – 2. uterine: concurrent series of changes in the endometrium of the uterus to prepare it for embryo implantation -3 major types of estrogens: 1. beta-estradiol 2. estrone 3. estriol 4. other smaller quantities -follicular estrogens: a. promote the development of the female reproductive structures, secondary sex characteristics and the mammary glands b. increase protein anabolism, including bone synthesis c. lower blood cholesterol d. inhibit the release of GnRH, FSH and LH -GnRH causes release of FSH and LH from anterior pituitary -FSH initiates follicular growth -LH stimulates the maturation of follicles -both LH and FSH stimulate the secretion of estrogens from the follicle -LH stimulates the theca layers of the follicle to make androgens -FSH stimulates the uptake of these androgens and converts them to estrogens -LH triggers ovulation and results in development of corpus luteum -corpus luteum produces and releases progesterone and some estrogen plus relaxin and inhibin -estrogen and progesterone regulate pregnancy, menstruation, secondary sex char’s & development of sex organs at puberty -relaxin – relaxes the uterus by inhibiting contractions of the myometrium -important to the implantation of the embryo – produced by the placenta during pregnancy -also increases the flexibility of the pubic symphysis -inhibin - inhibits secretion of FSH and LH 1. Menstrual Phase A. Ovarian events – FSH increase causes development of primary follicles and primary oocytes B. Uterine events – 50-150 mL of blood, tissue fluid, mucus and epithelial cells -shed from the stratum functionalis -occurs because of declining levels of E and P – loss of stratum functionalis - leaving the stratum basalis intact 2. Preovulatory Phase – most variable in length A. Ovarian events – secretion of E and inhibin from the secondary follicles -one secondary follicle outgrows the rest to become the dominant follicle -the dominant follicle secretes E and I which causes an inhibition of FSH and a decrease in the stimulation of other follicles -the dominant follicle develops into the Graafian follicle -forms a blister-like bulge due to an increase in fluid within the antrum of the follicle -the GF continues to increase its estrogen production B. Uterine events – E stimulates the repair of the SF – growth from the stratum basalis -increase in arteriole size and blood supply • 3. Ovulation • A. Ovarian events – rupture of the GF usually around day 14 • ovulated secondary follicle remains surrounded by its corona radiata and its zone pellucida • triggered by a positive feedback system – high levels of E at the end of the preovulatory phase increases the secretion of GnRH, which then increases the release of LH • increased LH induces rupture of the GF about 9 hours after the LH peak • basis for the at-home ovulatory tests – detect rises in LH • B. Uterine events - none • signs of ovulation – – – – Increase in basal body temperature Changes in cervical mucus Cervix softens Mittelschmerz---pain • 4. Postovulatory Phase – most consistent part of the cycle (14 days) – A. Ovarian events – the mature graafian follicle collapses and bleeds - the development of a blood clot results as the follicle induces bleeding – follicle is now called the corpus hemorrhagicum • granulosa and thecal cells come into direct contact – follicle is transformed into corpus luteum cells under the influence of LH • luteal cells produce hormones - progesterone, estrogen, relaxin and inhibin – Progesterone and estrogen are now –ve feedback signals for inhibition of GnRH – together with inhibin • if the ovum is NOT fertilized, the CL degenerates into the corpus albicans – 2 weeks • Resulting decrease in P, E and Inhibin results in the release of GnRH, FSH and LH (loss of negative feedback) - new follicular growth begins • if fertilized – the CL persists beyond 2 weeks by the secretion of human chorionic gonadotropin (hCG) hormone produced by the developing chorion that surrounds the embryo (8 days post-fertilization) GnRH release Stratum functionalis B. Uterine events – P and E produced by the corpus luteum promotes the growth and vascularization of the endometrium and its thickening to about 12-18 mm -endometrial glands within the endometrium begin to secrete glycogen – energy for the fertilized egg Summary Birth Control Methods • • • • • Surgical Hormonal Mechanical barriers Periodic abstinence Coitus interruptus Reproductive disorders • Males – – – – • Females – – – – – – • testicular cancer prostate concer erectile dysfunction (ED) benign prostatic hyperplasia PMS PMDD Endometriosis Ovarian, uterine cysts Ovarian, uterine, cervical cancer vulvovaginal candidiasis Both – UTI – STDs – gonorrhea, syphillis, chlamydia, genital herpes, genital warts Pregnancy -fertilization in the upper third of the oviduct/fallopian tube -fertilization = union of egg and sperm -plasma membrane of the egg is surrounded by an extracellular matrix = zona pellucida and a ring of follicular cells = corona radiata (nourishment in the follicle) -after fertilization = zygote 1. sperm penetrates corona radiata 2. several sperm enter zona pellucida -one of the glycoproteins within the ZP (ZP3) acts as a receptor for the sperm -binding causes dissolution of the acrosome and release of digestive enzymes 3. ONE sperm penetrates the plasma membrane of the egg 4. immediate change in the oocyte cell membrane (depolarizes) -also binding results in release of intracellular calcium which stimulates exocytosis of secretory vesicles whose contents inactivate ZP3 and harden the zona pellucida - impervious to more sperm 5. oocyte releases the zona pellucida away from the egg surface 6. fusion of the sperm with nucleus of the egg -before fusion the secondary oocyte must complete meiosis II and form the ovum embryonic stage: week 2 to week 8 -after sperm penetration and ovum development the nuclei of the egg and sperm undergo changes to become pronuclei -union of sperm and egg pronuclei nuclei forms the zygote -first cell division = embryo -first division takes place 24 hours post-fertilization – takes 6 hours to complete -each succeeding division takes less time -72 hr stage = 16 cells -96 hr stage = morula (embryo is the size of the original ovum, filled with cells (blastomeres) Implantation • attaches after about 6 days • usually in the fundus or the body of the uterus • orients its inner cell mass toward the uterus • 7 day – the endometrium becomes more vascularized • 9 days – completely embedded • following implantation, the endometrium is called the decidua – several layers with defined functions -day 4 – formation of morula and passage into the uterine cavity -endometrial glands release a glycogen-rich fluid = uterine milk -enters the morula through the zona pellucida and provides nourishment -day 5 -the fluid begins to collect in the morula and reorganizes them around a fluid-filled cavity = blastocoel -embryo is now called a blastula or blastocyst (50-150 cells) -outer layer = trophoblast - forms extraembryonic tissues (e.g. placenta, yolk sac) -inner cell mass at one end - totipotent embryonic stem cells -by the end of day 5, the blastocyst digests a hole in the ZP and squeezes through it to undergo implantation -second week of development - the inner cell mass flattens = embryonic disk (hypoblast and epiblast) -hypoblast = primitive endoderm -epiblast = primitive ectoderm -amniotic cavity forms between the inner cell mass and the trophoblast -surrounded by an amniotic membrane – develops from the epiblast -fills with amniotic fluid – filtrate from maternal blood at initial stages -formation of the yolk sac (from the hypoblast) -forms blood cells, gives rise to sex cells and the stem cells of the immune system -also forms part of the embryonic digestive tube -portion will also become part of the umbilical cord -the outer trophoblast cells develops into two layers within the region where the blastocyst and the endometrium make contact – become part of the chorion -these trophoblast cells will secrete digestive enzymes that allow the embryo to burrow into the decidua -also secrete hCG – rescues the corpus luteum from degeneration • day 15: embryonic disk undergoes gastrulation to form the gastrula embryonic stage – formation of the three embryonic germ layers by differentiation of the ES cells within the embryonic disc • epiblast form a specialized region = primitive streak – – – – – clearly establishes a head and tail orientation head end the streak enlargens to form the primitive node cells from the epiblast move inward through the primitive streak some cells displace the hypoblast and form the endoderm other cells are retained in the area and form the mesoderm • mesoderma forms a loose connective tissue = mesenchyme – cells remaining in the epiblast form the ectoderm -portions of the mesoderm that do not form the notochord segment into sections called somites -> specific body regions and structures -in front of the primitive streak forms the primitive node – head and associated structures -mesodermal cells from the primitive node form a hollow tube near the future head of the embryo - become the notochord (day 22-24) (progenitor to the vertebral column) -four weeks of development - embryo forms a tubular structure -embryo begins to form definitive structures: -neural folds of ectoderm -> nervous system (brain and spinal cord) ** neurulation occurs by induction (one tissue influences the development of another) -e.g. nervous system requires the mesodermal cells of the notochord