Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
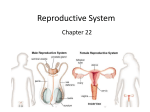
Physiology and Health: Chapter 8-10 Summary The testes of the human male produce sperm from germline cells in seminiferous tubules and make testosterone in interstitial cells. The mobility and viability of sperm are maintained by fluids secreted by the prostate gland and seminal vesicles. The ovaries of the human female contain germline cells that produce ova (eggs) each surrounded by a protective follicle. Hormones made by the ovary are oestrogen and progesterone. The pituitary gland releases follicle stimulating hormone (FSH) and interstitial-cellstimulating hormone (ICSH)/luteinsing hormone (LH). In men, FSH stimulates sperm production and ICSH promotes testosterone production. The concentration of testosterone is maintained at a steady level by negative feedback control. In women, FSH stimulates the development of a follicle containing an ovum (egg) and the secretion of oestrogen. LH triggers ovulation and brings about the development of the corpus luteum which secretes progesterone. Oestrogen stimulates the proliferation of the endometrium and progesterone promotes its further development and vascularisation. The menstrual cycle lasts for about 28 days and involves a follicular phase and a luteal phase. Fertility in men is continuous; fertility in women is cyclical, being restricted to the 1-2 days following ovulation in each monthly cycle. Infertility may be caused by failure to ovulate, blockage of oviducts or failure of implantation in women, and low sperm count in men. Methods of treatment of infertility include the use of drugs that stimulates ovulation, artificial insemination, in--vitro fertilisation (IVF) and intracytoplasmic sperm injection (ICSI). Pre-implantation genetic diagnosis may be used during IVF to check an embryo for chromosomal defects before implantation. Some methods of contraception are based on biological knowledge of the menstrual cycle and the avoidance of fertile periods. Other physical methods depend on barriers, intrauterine devices or sterilisation. Some chemical methods prevent follicles from being stimulated and eggs from being released. Others cause thickening of cervical mucus. During antenatal care, a dating scan is made by ultrasound imaging to determine the stage the pregnancy has reached. An anomaly scan is used to detect physical problems with the fetus. Signs of medical conditions suffered by pregnant women can be detected using screening tests for marker chemicals. These allow risk of genetic disorders in the fetus to be assessed and may be followed up by diagnostic tests. A karyotype is a display of a compliment of chromosomes arranged in pairs to show their form, size and number. During amniocentisis, a sample of amniotic fluid is taken to obtain cells for karyotyping to check for chromosomal abnormalities. During chorionic villus sampling, cells for the same purpose are obtained from the placenta. This procedure carries a higher risk of miscarraige than amniocentesis. A Rhesus-negative mother is given anti-rhesus antibodies after birth of a Rhesus-positive baby to destroy and Rhesus antigens before her immune system has time to respond to them. Postnatal screening is carried out on newborn babies to check for metabolic disorders such as PKU. Information about particular characteristics can be collected from the members of a family and be used to construct a pedigree chart. Single gene disorders show different patterns of inheritance, such as autosomal recessive.