Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
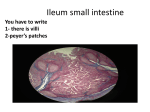
DIGESTIVE SYSTEM FUNCTION?? MAKE FOOD SMALL ENOUGH TO BE ABSORBED MONOMERS DIGESTIVE SYSTEM kidshealth.org DIGESTIVE SYSTEM www.nlm.nih.gov DIGESTIVE SYSTEM arbl.cvmbs.colostate.edu MICROANATOMY OF THE DIGESTIVE TUBE arbl.cvmbs.colostate.edu MUCOSA SURFACE EPITHELIUM; CONNECTIVE TISSUE; SMOOTH MUSCLE; SOME HAVE FOLDINGS TO ?; TUBULAR GLANDS: – MUCUS; DIGESTIVE ENZYMES LUMEN PROTECTS LAYERS & BODY; SECRETION AND ABSORPTION SUBMUCOSA LOOSE CONNECTIVE TISSUE; GLANDS; BLOOD VESSELS; LYMPH VESSELS; NERVES; TO NOURISH AND TRANSPORT MATERIAL AWAY MUSCULAR LAYER INNER COAT: CIRCULAR SMOOTH MUSCLE FIBERS: DIAMETER DECREASES OUTER COAT: LONGITUDINAL FIBERS: TUBE SHORTENS FOR MOVEMENTS SEROSA/SEROUS LAYER OUTER COVERING: VISCERAL PERITONEUM; CONNECTIVE TISSUE WITH EPITHELIUM ON TOP (OUTSIDE); PROTECT TISSUES BELOW; SECRETE SEROUS FLUID: MOISTENS AND LUBRICATES SO ORGANS SLIDE FREELY MUCOSAL EPITHELIUM arbl.cvmbs.colostate.edu MOVEMENTS MIXING: – MOVEMENT OF STOMACH, OR SEGMENTS (SEGMENTATION); MIXES FOOD AND DIGESTIVE ENZYMES PROPELLING: – PERISTALSIS: RING OF CONTRACTION & CAUSES RECEPTIVE RELAXATION SEGMENTATION arbl.cvmbs.colostate.edu PERISTALSIS arbl.cvmbs.colostate.edu PERISTALSIS www.nlm.nih.gov INNERVATION USUALLY WHICH ONE ? PARASYMPATHETIC – BY PLEXUSES ? – INCREASE ACTIVITY; VAGUS NERVE & SACRAL POTION OF S.C. SYMPATHETIC – DECREASE – FIGHT OR FLIGHT MOUTH CHEEK & LIPS: SKELETAL MUSCLES TONGUE: – LINGUAL FRENULUM: TO FLOOR – PAPILLAE FRICTION, TASTE BUDS – HYOID BONE – LINGUAL TONSILS: OF ? PALATE – ANTERIOR: HARD – POSTERIOR: SOFT – UVULA SWALLOWING: CLOSE NASAL PASSAGES – PALATINE TONSILS – PHARYNGEAL TONSILS: ADENOIDS TEETH HARDEST STRUCTURES OF BODY NOT BONE ? PRIMARY: 10; 6 Mo TO 4y SECONDARY: 32; 6 y TO 22y FUNCTION: ? WHY? – INCISORS: BITE – CANINES: GRAB AND TEAR – PREMOLARS, MOLARS: GRINDING TEETH en.wikipedia.org CROWN – ENAMEL: CALCIUM; HARDEST SUBSTANCE; NOT REPLACED, WEARS DOWN ROOT DENTIN: HARDER THAN BONE CENTRAL CAVITY: PULP – BLOOD VESSELS, NERVES, CONNECTIVE TISSUE ROOT CANALS: CEMENTUM AROUND ROOT PERIDONTAL LIGAMENT: COLLAGEN; CEMENTUM TO JAW SALIVARY GLANDS PRODUCE ? FOR? – MOISTENS, BINDS, STARTS CHEMICAL DIGESTINO OF FOOD; SOLVENT: DISSOLVES FOOD = TASTE; BICARBONATE IONS: BUFFER: BALANCE pH FOR ENZYME ACTION; 3 PAIR AND MANY MINOR GLANDS 3 PAIR AND MANY MINOR GLANDS – SEROUS GLANDS SALIVARY AMYLASE – STARCH AND GLYCOGEN – MUCOUS GLANDS BINDS; LUBRICATES SALIVARY CONTROL PARASYMPATHETIC – LARGE AMOUNT OT WATERY SALIVA – REFLEX: PAVLOV’S DOGS SYMPATHETIC – SMALL AMOUNT OF VISCOUS SALIVA – UNPLEASANT LOOK, TASTE, SMELL – LESS SALIVA= HARD TO SWALLOW SALIVARY GLANDS www.entassociates.com MAJOR SALIVARY GLANDS PAROTID – LARGEST; CLEAR WATERY; LOTS OF AMYLASE SUBMANDIBULAR – EQUALLY SEROUS AND MUCOUS SUBLINGUAL – SMALLEST OF 3 – MOSTLY MUCOUS PHARYNX CONNECT NASAL AND ORAL CAVITY TO LARYNX AND ESOPHAGUS NASOPHARYNX – BEHIND SOFT PALATE – AIR PASSAGEWAY – EUSTACHIAN CANAL OPENING OROPHARYNX – END OF OUTH TO EPIGLOTTIS LARYNGOPHARYNX – EPIGLOTTIS TO LARYNX PHARYNX 1) Nasopharynx 2) Nasal Septum 3) Hard Palate 4) Tongue 5) Oropharynx 6) Laryngopharynx anatomy.med.umich.edu CIRCULAR MUSCLES= CONSTRICTOR MUSCLES – SUPERIOR; MIDDLE; INFERIOR SOME OF INFERIOR CONSTRICTOR MUSCLES ARE USUALLY CONTRACTED TO KEEP AIR OUT OF ESOPHAGUS SKELETAL MUSCLES BUT MOSTLY A REFLEX SWALLOWING STEPS 1: VOLUNTARY; CHEWING AND TURNING FOOD INTO BOLUS; TONGUE FORCES TO PHARYNX 2: SWALLOWING REFLEX STIMULATED – SOFT PALATE RAISES ? – EPIGLOTTIS BLOCKS TRACHEA ? – TONGUE PRESSES ON SOFT PALATE ? – LONGITUDINAL MUSCLES CONTSTRICT ? – INFERIOR CONSTRICTOR MUSCLE RELAXES ? – SUPERIOR CONSTRICTOR MUSCLE CONTRACTS 3: PERISTALSIS: FOOD THROUGH ESOPHAGUS TO STOMACH EPIGLOTTIS – http://www.youtube.com/watch?v=aPMw7acr Vro&feature=player_detailpage SWALLOWING: http://www.youtube.com/watch?v=wqMCzuIiPa M ESOPHAGUS 25 CM; COLLAPSIBLE ?; HOW DOES FOOD GET TO ABDOMEN ? – HIATUS – MUCOUS GLANDS ? – LOWER ESOPHAGEAL SPHINCTER ? – USUALLY CLOSED ? – PERISTALSIS OPENS SPHINCTER ? STOMACH 25-30 CM; CAVITY ~ 1L; RUGAE ? JUST BELOW DIAPHRAGM TYPE OF DIGESTION ? – BOTH; MIXES FOOD WITH GASTRIC JUICE; STARTS PROTEIN DIGESTION; SOME ABSORPTION; FOOD TO INTESTINES REGULAR 2 SMOOTH MUSCLE LAYERS: PLUS OBLIQUE MUSCLES (ESPECIALLY FUNDUS AND BODY); – STRONGER; MORE MIXING http://gerd.emedtv.com/gerd-video/whathappens-when-you-have-gerd-video.html PARTS CARDIA: NEAR ESOPHAGEAL OPENING FUNDUS: BALLOON AREA AT START: STORAGE BODY: DILATED AREA; MIDDLE; PYLORIC ANTRUM: FUNNEL SHAPED; AT END TO ? PYLORIC CANAL: BEFORE SMALL INTESTINE PYLORIC SPHNCTER: THICK CIRCULAR MUSCLE; VALVE: CONTROLS EMPTYING GASTRIC SECRETIONS GASTRIC PITS: GASTRIC GLANDS: TUBULAR: OR 3 SECTRETORY CELL TYPES – MUCOUS: NEAR OPEININGS OF PITS; – CHIEF CELLS: DEEPER; DIGESTIVE ENZYMES – PARIETAL CELLS: DEEPER; HCl – ALL= GASTRIC JUICE CHIEF CELLS RELEASE PEPSINOGEN: INACTIVE FORM OF PEPSIN WHY INACTIVE? – PEPSINOGEN AND HCl= PEPSIN GASTRIC LIPASE: MOSTLY ON BUTTERFAT BECAUSE OF LOW pH MUCUS PROTECTS FROM PEPSIN PARIETAL CELLS ALSO SECRETE INTRINSIC FACTOR: HELPS ABSORB VITAMIN B12 CONTROL OF GASTRIC SECRETIONS PRODUCED CONTIUOUSLY BUT IN VARYING AMOUNTS CELLS OF GASTRIC GLANDS SECRETE SOMATOSTATIN: INHIBITS ACID SECRETION PARASYMPATHETIC: ACh SUPRESSES SOMATOSTATIN AND MORE GASTRIC JUICE PRODUCED GASTRIN ALSO INCREASES SECRETION CAUSE HISTAMINE TO BE RELEASED= INCREASES GASTRIC SECRETION http://highered.mcgrawhill.com/olcweb/cgi/pluginpop.cgi?it=swf:: 535::535::/sites/dl/free/0072437316/1201 05/anim0037.swf::Three%20Phases%20of %20Gastric%20Secretion http://highered.mcgrawhill.com/olcweb/cgi/pluginpop.cgi?it=swf:: 535::535::/sites/dl/free/0072437316/1201 05/anim0037.swf::Three%20Phases%20of %20Gastric%20Secretion THREE STAGES CEPHALIC PHASE: – BEFORE FOOD ENTERS STOMACH: SMALL, TASTE, LOOK, THOUGHT OF FOOD BY PARASYMPATHETIC STIMULATION – GREATER HUNGER = GREATER SECRETION – 30-50% OF SECRETION GASTRIC PHASE: – 40-50%; WHEN FOOD ENTERS STOMACH – DISTENSION OF STOMACH = RELEASE OF GASTRIN = PRODUCTION OF MORE GASTRIC SECRETION – pH AT 3.0 = GASTRIN INHIBITED; 1.5 = GASTRIC SECRETION STOPS – H FOR HCl COMES FROM BLOOD REPLACED BY BICARBONATE ION INTESTINAL PHASE: – 5%; WHEN FOOD ENTERS SMALL INTESTINES RELEASES INTESTINAL GASTRIN FROM INTESTINES – MORE FOOD ENTERS SMALL INTESTINES AND SYMPATHETIC IMPULSES = INHIBITS SECRETION – PROTEIN AND FAT RELEASES CHOLECYSTOKININ WHICH SLOWS MIXING OF STOMACH – FATS CAUSE RELEASE OF INTESTINAL SOMATOSTATIN WHICH DECREASES GASTRIC SECRETION GASTRIC ABSORPTION A LITTLE BIT – WATER, SOME SALTS, SOME LIPID-SOLUBLE DRUGS, ALCOHOL MIXING/EMPTYING STOMACHACHE FROM TOO MUCH FOOD MIXING: BOLUSCHYME PERISTALSIS SLOWLY MOVES CHYME INTO SMALL INTESTINES PASSING THROUGH DEPENDS ON TYPE OF FOOD: FATS UP TO 6 HOURS AS FOOD ENTERS SMALL INTESTINES THE PRESSURE BUILDS UP AND ENTEROGASTRIC REFLEX INHIBITS STOMACH PERISTALSIS AND SLOWS INTESTINAL FILLING CHOLECYSTOKININ RELEASED TO DECREASE PERISTALSIS Peristalsis http://www.nature.com/gimo/contents/pt 1/fig_tab/gimo13_V1.html http://www.youtube.com/watch?v=Ln09qi hUi3g&feature=player_embedded http://emedicine.medscape.com/article/19 48973-overview VOMITTING: REVERSE PERISTALSIS BY VOMITTING CENTER OF MEDULLA CONTRACTS ON STOMACH TO EXPELL STOMACH PANCREAS DUCT TO DUODENUM CELLS: – PANCREATIC ACINAR CELLS PANCREATIC JUICE PANCREATIC ACINAR CELLS: – PANCREATIC AMYLASE: ? – PANCREATIC LIPASE: ? – TRYPSIN, CHYMOTRYPSIN, CARBOXYPEPTIDASE: SPECIFIC PEPTIDE BONDS STORED AND RELEASED IN INACTIVE FORMS ? TRYPSINOGEN ACTIVATED BY ENTEROKINASE THEN TRYPSIN ACTIVATES THE OTHER 2 NUCLEASES: ? BICARBONATE: ALKALINE; NEUTRALIZES HCl CONTROL OF SECRETION NERVOUS AND ENDOCRINE SYSTEMS DURING CEPHALIC AND GASTRIC PHASES PARASYMPATHETIC STIMULATES PANCREAS SECRETIN STIMULATES RELEASE WHEN CHYME ENTERS DUODENUM: MOST;LY BICARBONATE IONS PROTEIN & FAT STIMULATES RELEASE OF CHOLECYSTOKININ STIMULATES SECRETION LIVER FIBROUS CAPSULE; TWO MAJOR LOBES; TWO MINOR LOBES HEPATIC LOBULES: FUNCTIONAL UNIT – HEPATIC CELLS; HEPATIC SINUSOIDS; – KUPFFER CELLS: REMOVE BACTERIA – COMMON HEPATIC DUCT CARBOHYDRATE METABOLISM, GLYCOGEN; GLUCONEOGENESIS; OXIDIZING FATTY ACIDS; SYNTHESIS OF MOLECULES; DEAMINATION OF AMINO ACIDS, FORMATION OF UREA AND OTHER AMINO ACIDS; STORAGE: GLYCOGEN, IRON, VITAMINS A, D, B12; DESTROY DAMAGED RBCs; REMOVES TOXIC MATERIAL; PHAGOCYTIZE PATHOGENS; BLOOD RESERVOIR; SECRETES BILE BILE WATER, BILE SALTS, BILE PIGMENTS, CHOLESTEROL, ELECTROLYTES GALL BLADDER DEPRESSION IN LIVER STORES, CONCENTRATES AND RELEASES BILE RELEASED WHEN STIMULATED BY CHOLECYSTOKININ RELEASED THROUGH BILE DUCT TO HEPATOPANCREATIC SPHINCTER CHOLESTEROL COULD FORM GALL STONES BILE SALT FUNCTION EMULSIFICATION – AIDS LIPASE AIDS ABSORBTION – FATTY ACIDS, GLYCEROL, & FAT SOLUBLE VITAMINS: A, D, E, K MOST OF BILE SALTS ARE REABSORBED IN SMALL INTESTINES SMALL INTESTINE 9-10 FT LONG RECEIVES DIGESTIVE ENZYMES FROM LIVER AND PANCREAS; FINISHES CHEMICAL DIGESTION; ABSORBTION; MOVES MATERIAL TO LARGE INTESTINES PARTS DUODENUM: – SHORTEST (25cm); MOST FIXED; JEJUNUM: – PROXIMAL 2/5THS; MOBILE ILEUM: – REST; MOBILE; USUALLY NO DISTINCT BREAK BUT JEJUNUM HAS LARGER DIAMETER; THICKER WALL, MORE ACTIVE, MORE VASCULAR, MORE LYMPH MATERIAL HELD BY MESENTERY STRUCTURE INTESTINAL VILLI ? – ESPECIALLY DUODENUM AND PROXIMAL JEJUNUM – SIMPLE COLUMNAR EPITHELIUM; LACTEAL; MICROVILLI ? – INTESTINAL GLANDS/CRYPTS OF LIEBERKUHN – PLICAE CIRCULARES ? SECRETIONS GOBLET CELL: ? BRUNNER’S GLANDS – SUBMUCOSA OF PROXIMAL DUODENUM – THICK, ALKALINE MUCUS INTESTINAL GLANDS – BASE OF VILLIE – A LOT OF WATERY FLUID; NO ENZYMES ? – ENZYMES IN MEMBRANE OF MICROVILLI CELLS PEPTIDASES SUCRASE, MALTASE, LACTASE INTESTINAL LIPASE REGULATION OF SECRETION MUCUS SECRETION INCREASES IN RESPONSE TO MECHANICAL STIMULUS AND IRRITANTS (GASTRIC JUICE) CHYME STIMULATES GOBLET AND INTESTINAL CELLS TO SECRETE DISTENSION: PARASYMPATHETIC STIMULATION TO INCREASE SECRETION ABSORPTION MOST ABSORBABLE MATERIAL IS ABSORBED MONOSACCHARIDES – FACILLITATED DIFFUSION PROTEINS – ACTIVE TRANSPORT LIPIDS – FATTY ACIDS: DIFFUSE RESYNTHESIZED BY ER CLUSTERS ENCASED IN PROTEIN: CHYLOMICRONS TO LACTEALS CONTRACTIONS MOVE CHYLOMICRONS THROUGH LYMPH TO BLOOD TO MUSCLE AND ADIPOSE TISSUE VLDL: VERY-LOW-DENSITYLIPOPROTEINS CARRY TRIGLYCERIDES TO ADIPOSE TISSUE VLDL LDL (LOW-DENSITYLIPOPROTEINS) HIGH CHOLESTEROL REMOVED BY CELLS HDL (HIGH-DENSITY-LIPOPROTEINS) REMOVE CHOLESTEROL FROM CELLS TO LIVER ENTER BY RECEPTORMEDIATED ENDOCYTOSIS CHOLESTEROL BECOMES BILE OR BILE SALTS MOST IS REABSORBED ALSO REABSORBS – WATER – ELECTROLYTES PROTEINS arbl.cvmbs.colostate.edu LIFE SPAN CHANGES OVERALL: SLOW, LITTLE TOOTH CARE VITAL – LOSS OF ENAMEL; WEAR; CEMENTUM AND DENTUM THICKEN, PULP LESSENS; NEURON LOSS; GUMS RECEDE; LOOSE TEETH; XEROSTOMIA: DRY MOUTH – MOST OFTEN DUE TO MEDICATIONS PERISTALSIS SLOWS= HEARTBURN; STOMACH LINING THINS; GASTRIC SECRETIONS DIMININSH = TAKES LONGER FOR DIGESTION SMALL INTESTINE ABSORBS LESS: A,D,K, AND ZINC – A: SKIN AND VISION PROBLEMS – D: WEAK BONES – K: LESS CLOTTING – ZINC: LOWERED HEALING AND IMMUNITY, ALTERED TASTE LACTOSE INTOLERANCE LESS INTRINSIC FACTOR: ANEMIA LOSS OF MUSCLE AND ELASTICITY: LESS PERISTALSIS OF LARGE INTESTINE: CONSTIPATION PANCREAS AND LIVER DON’T CHANGE MUCH LIVER MAY NOT DETOXIFY AS WELL GALLBLADDER LESS SENSITIVE BUT COMPENSATES