Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Calorie restriction wikipedia , lookup
Human nutrition wikipedia , lookup
Adipose tissue wikipedia , lookup
Low-carbohydrate diet wikipedia , lookup
Epidemiology of metabolic syndrome wikipedia , lookup
Saturated fat and cardiovascular disease wikipedia , lookup
Body fat percentage wikipedia , lookup
Fat acceptance movement wikipedia , lookup
Waist–hip ratio wikipedia , lookup
Overeaters Anonymous wikipedia , lookup
Food choice wikipedia , lookup
Gastric bypass surgery wikipedia , lookup
Obesity and the environment wikipedia , lookup
Diet-induced obesity model wikipedia , lookup
Abdominal obesity wikipedia , lookup
Childhood obesity wikipedia , lookup
Body mass index wikipedia , lookup
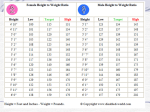
Obesity, Overweight and Weight Control Healthy Weight Network Prevalence of Overweight Among Children & Adolescents 6-19 Years Age 1963-65 (Years) 1966-70 197174 197680 198894 19992002 6-11 4% 4% 7% 11% 16% 12-19 5% 6% 5% 11% 16% Source: National Center for Health Statistics Overweight and Obesity Definitions Height/Weight Tables Metropolitan Life Insurance, revised 1983 Based on weight-height mortality study Weights are ages 25 to 59 based on lowest mortality Height and Weight Chart - height weight chart, weight height chart Overweight and Obesity Definitions BMI = weight (kg) height squared (m²) Significantly correlated with total body fat content Classification of Overweight and Obesity by BMI Obesity Class BMI kg/m2 Underweight <18.5 Normal 18.5–24.9 Overweight 25–29.9 Obesity Extreme Obesity I 30.0–34.9 II 35.0–39.9 III 40.0 Overweight and Obesity - Definitions Waist Circumference Presence of excess fat in abdomen out of proportion to total body fat is a independent predictor of risk and mortality. Waist circumference is positively correlated with abdominal fat content. High Risk: Men >102 cm (>40 in.); Women > 88 cm (>35 in.) Waist-to-Hip Ratio Waist-to-hip ration measures waist at its narrowest point and hip at widest point. Women with 35” waist and 46”hip = 35/46 = 0.76 Risk: Women with waist-to-hip ratio >0.8 Men with waist-to-hip ratio > 1.0 Assessment of Obesity Anthropometrics Medical Psychological Nutritional Weight Control Advantages of Weight Loss: Blood Pressure Serum/Plasma Lipids Reductions in serum triglycerides and increases in HDL Reductions in total cholesterol and LDL Blood Glucose NHANES III Age-Adjusted Prevalence of Hypertension* According to BMI BMI <25 BMI 25-26 BMI 27-29 BMI >30 50 38.4 Percent 40 32.2 30 20 22.5 25.2 18.2 21.9 24.0 16.5 10 0 Men Women *Defined as mean systolic blood pressure 140 mm Hg, as mean diastolic 90 mm Hg, or currently taking antihypertensive medication . Brown C et al. Body Mass Index and the prevalence of Risk Factors for Cardiovascular Disease (in preparation). NHANES III Age-Adjusted Prevalence of High Blood Cholesterol* According to BMI BMI <25 BMI 25-26 BMI 27-29 BMI >30 Percent 50 40 27.9 30 20 14.7 17.5 20.4 28.2 20.2 15.7 10 0 Men *Defined as > 240 mg/dL. Brown C et al. Body Mass Index and the Prevalence of Risk Factors for Cardiovascular Disease (in preparation). Women 24.7 NHANES III Age-Adjusted Prevalence of Low HDL-Cholesterol* According to BMI BMI <25 BMI 25-26 BMI 27-29 BMI >30 Percent 60 50 41.5 40 31.4 30 23.1 17.2 20 10 27.0 27.2 16.5 9.1 0 Men *Defined as <35 mg/dL in men and <45 mg/dL in women. Brown C et al. Body Mass Index and the Prevalence of Risk Factors for Cardiovascular Disease (in preparation). Women Nutritional Assessment Weight History Age of onset Highest/lowest adult weights Patterns of weight gain and loss Environmental triggers Current eating patterns Nutritional Intake Nutritional Assessment Environmental Factors Exercise history Motivation and readiness to change Treatment for Obesity BMI 25-26.9 27-29.9 Diet, Physical Activity & Behavior Therapy With comorbiditie s With comorbiditie s Pharmcotherapy Surgery 30-34.9 If not lost 1#/week after 6 mo. With comorbiditie s 3539. 9 >40 Position of ADA Successful weight management requires a livelong commitment to healthful lifestyle behaviors emphasizing sustainable and enjoyable eating practices and daily physical activity Position Paper Goals for Weight Loss Prevent weight gain or stop weight gain Improvement in physical and emotional health Small maintainable weight losses or more extensive weight loss through sensible eating and exercise patterns Improvement in eating, exercise and other behaviors apart from any weight loss Goals for Weight Loss Initial goal to reduce body weight by approximately 10% from baseline. 1-2#/week for period of 6 months 1# body fat = 3500 calories 3500/7days = - 500 calories/day Need to assess individual’s motivation and readiness to enter weight loss therapy. How To Achieve Weight Loss 1,000 – 1,200 kcal/day for women and 1,200 – 1,600 kcal/day for men Reducing dietary fat along with carbohydrates can facilitate calorie reduction. Reducing dietary fat alone without reducing calories is not sufficient for weight loss. How To Achieve Weight Loss Physical activity is recommended as part of a comprehensive weight loss program because: contributes to weight loss may decrease abdominal fat increase cardio-respiratory fitness may help with maintenance of weight loss How To Achieve Weight Loss Behavior Therapy Pharmacotherapy - weight loss drugs Weight loss drugs may be used in combination with a comprehensive weight loss program, for patients with BMI>=30 with no risk factors & BMI >=27 with risk factors. Weight loss drugs should never be used without concomitant lifestyle changes. How To Achieve Weight Loss Better weight loss results are achieved with diet therapy when the duration of the intervention is at least 6 months. Long term weight loss is enhanced by a program of dietary therapy, physical therapy and behavioral therapy continued indefinitely. “Habit is habit and not to be flung out of the window by any man, but coaxed downstairs a step at a time.” –Mark Twain How To Achieve Weight Loss Outcome data on behavior therapy, Very Low Calorie Diets (VLCD) and Pharmacotherapy show weight regain in 3-5 years Frequent contacts between professional counselors and patients promote weight loss and weight maintenance Chicago Tribune | Biggest 'Lost' mystery: Why is Hurley still fat? Tips for Weight Loss Eat a variety of foods from the Food Guide Pyramid, including favorite foods Increase intake of high-water/high-fiber foods Vegetables and fruits Whole grains and legumes Soups Decrease consumption of energy dense foods High fat foods Foods with low moisture content Mayo Clinic Food Guide How to Calculate Energy Density Energy Density = Calories/Grams E.G. 150 Calories/100 grams = 1.5 Kcal/g Energy density of 1 – Eat any quantity Limit foods with energy density >2 Tips for Weight Loss Limit consumption of beverages containing alcohol and sugars Control Portion Sizes Plan meals and snacks ahead Establish regular eating habits Shop on a full stomach Shopping Tips Use a shopping list Read labels serving size and servings per container Tips for Weight Loss Eat from plates, not food packages Portion foods before bringing them to the table Eat slowly Sit down to eat Stop eating when you leave the table Watch for food ‘triggers’ Tips for Weight Loss Use of Meal Replacements? Fad Diets Americans spend >30 billion in the weight loss industry Single food diets - grapefruit, rice etc. High-protein, high fat diets VLCD Fasting High fiber, low-calorie diets Weight Loss Surgery