Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
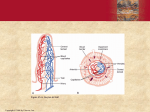
Chapter 30 Medical Nutrition Therapy for Lower Gastrointestinal Tract Disorders Common Intestinal Symptoms Intestinal gas and flatulence Constipation Diarrhea Steatorrhea Gastrointestinal strictures and obstruction © 2004, 2002 Elsevier Inc. All rights reserved. Diarrhea Need to solidify stools Pectin (apples, bananas) is helpful World Health Organization provides guidance on fluid and electrolyte replacements—set formula works best Gatorade also useful © 2004, 2002 Elsevier Inc. All rights reserved. Steatorrhea Dietary Modification Increase kcal to meet needs, especially protein and carbohydrate Control fat level Give only level tolerated Use MCT oil to meet kcal needs with caution Vitamin and mineral supplements Use fat-soluble vitamins; add extra Ca, Mg, Zn, Fe © 2004, 2002 Elsevier Inc. All rights reserved. Steatorrhea MCT Oil 8 to 10 carbons long Bile not needed for absorption Delivered to liver via blood 8.3 kcal/g 1 T = 116 kcal Expensive Increases osmolality of tube feedings © 2004, 2002 Elsevier Inc. All rights reserved. Celiac Disease Gluten-Sensitive Enteropathy Adverse reaction to gluten—gliadin fraction Intestinal mucosa damaged —Malabsorption of nutrients —Iron deficiency —Osteomalacia —Growth failure —Projectile vomiting © 2004, 2002 Elsevier Inc. All rights reserved. Normal Human Duodenal Mucosa (A) and Peroral Small Bowel Biopsy Specimen (B) from a Patient with Gluten Enteropathy (From Floch MH. Nutrition and Diet Therapy in Gastrointestinal Disease. New York: Menum Medical Book Co., 1981.) © 2004, 2002 Elsevier Inc. All rights reserved. Celiac Disease−Cause Algorithm content developed by John Anderson, PhD, and Sanford C. Garner, PhD, 2000. Updated by Peter L. Beyer, 2002. © 2004, 2002 Elsevier Inc. All rights reserved. Celiac Disease−Pathophysiology (Adapted from Bray GA. Gray DS, Obesity, part 1: Pathogenisis. West J Med 149:429, 1988; and Lew EA, Garfinkle L; Variations in mortality by weight among 750,000 men and women. J Clin Epidemiol 32:563, 1979.) Algorithm content developed by John Anderson, PhD, and Sanford C. Garner, PhD, 2000. Updated by Peter L. Beyer, 2002. © 2004, 2002 Elsevier Inc. All rights reserved. Celiac Disease−Medical and Nutritional Management Algorithm content developed by John Anderson, PhD, and Sanford C. Garner, PhD, 2000. Updated by Peter L. Beyer, 2002. © 2004, 2002 Elsevier Inc. All rights reserved. Celiac Disease Gluten-Sensitive Enteropathy Treatment Remove gluten from the diet: —Wheat —Rye —Buckwheat —Barley © 2004, 2002 Elsevier Inc. All rights reserved. Celiac Disease Gluten-Sensitive Enteropathy—cont’d Gluten/gliadin-containing foods Used to thicken many processed foods See Tables 30-3 and 30-4 © 2004, 2002 Elsevier Inc. All rights reserved. Tropical Sprue Cause unknown; imitates celiac disease Results in atrophy and inflammation of villi Sx: diarrhea, anorexia, abdominal distention Rx: tetracycline, folate 5 mg/d, B12 IM © 2004, 2002 Elsevier Inc. All rights reserved. Intestinal Brush Border Enzyme Deficiencies Lactose intolerance Causes: genetic or secondary deficiency of milk sugar enzyme, lactase —Blacks, Asians, Native Americans —Aging: damage to GI tract Dx: lactose tolerance test or breath hydrogen test Rx: avoid large amounts of lactose (milk protein allergy requires milk-free diet); take lactase enzyme; processed dairy sometimes OK © 2004, 2002 Elsevier Inc. All rights reserved. Inflammatory Bowel Disease Crohn’s disease or ulcerative colitis Both involve damage to the intestine Crohn’s: may damage either small or large intestine Disease progression varies Ulcerative colitis: begins at rectum and progresses up the large intestine © 2004, 2002 Elsevier Inc. All rights reserved. Inflammatory Bowel Disease−Cause Algorithm content developed by John Anderson, PhD, and Sanford C. Garner, PhD, 2000. Updated by Peter L. Beyer, 2002. © 2004, 2002 Elsevier Inc. All rights reserved. Inflammatory Bowel Disease− Pathophysiology Algorithm content developed by John Anderson, PhD, and Sanford C. Garner, PhD, 2000. Updated by Peter L. Beyer, 2002. © 2004, 2002 Elsevier Inc. All rights reserved. Inflammatory Bowel Disease−Medical and Nutritional Management Algorithm content developed by John Anderson, PhD, and Sanford C. Garner, PhD, 2000. Updated by Peter L. Beyer, 2002. © 2004, 2002 Elsevier Inc. All rights reserved. Inflammatory Bowel Diseases Rx: Diet depends on patient’s status Nutrition assessment Select route of feeding Fiber is beneficial except during flareups. © 2004, 2002 Elsevier Inc. All rights reserved. Disorders of the Large Intestine 1. Irritable bowel syndrome —Common syndrome involving altered intestinal motility, increased sensitivity of the GI tract, and increased awareness and responsiveness of the viscera to internal and external stimuli —Alternating constipation and diarrhea, abdominal pain, and bloating © 2004, 2002 Elsevier Inc. All rights reserved. Disorders of the Large Intestine — cont’d 2. Diverticular disease —Herniations of the colon, chronic diverticulosis, acute diverticulitis —Diverticulosis High-fiber diet: fruits, vegetables, whole grains (2 tsp bran daily) —Diverticulitis Low-residue or elemental diet Possibly low-fat diet © 2004, 2002 Elsevier Inc. All rights reserved. Disorders of the Large Intestine — cont’d 3. Colon cancer and polyps —Colon cancer is the second most common cancer among US adults —Polyps are considered precursors of colon cancer. © 2004, 2002 Elsevier Inc. All rights reserved. Short Bowel Syndrome Follows removal of more than two thirds of small intestine Causes weight loss; diarrhea; decreased transit time; malabsorption; dehydration; loss of electrolytes; hypokalemia © 2004, 2002 Elsevier Inc. All rights reserved. Short Bowel Syndrome —cont’d Removal of ileocecal valve causes more complications. Fat malabsorption frequent Steatorrhea Saponify calcium, zinc, and magnesium Remove ileum and lose B12 and bile salt absorption © 2004, 2002 Elsevier Inc. All rights reserved. Short Bowel Syndrome —cont’d Factors Affecting Severity of Malabsorption, Number of Complications, and Dependence on Parenteral Nutrition Length of remaining small intestine Loss of ileum, especially distal one third Loss of ileocecal valve Loss of colon Disease in remaining segments(s) of gastrointestinal tract Radiation enteritis Coexisting malnutrition Older age surgery © 2004, 2002 Elsevier Inc. All rights reserved. Short Bowel Syndrome Nutritional Care Step 1 Parenteral only for most patients Step 2 Gradually introduce enteral nutrition. Glutamine is an important nutrient for the gut. Narcotic drugs for pain cause GI problems and should be evaluated. © 2004, 2002 Elsevier Inc. All rights reserved. Short Bowel Syndrome Eventually the remaining bowel increases absorptive surface, and problems decrease. Nutrition support is designed to meet each patient’s needs. © 2004, 2002 Elsevier Inc. All rights reserved. Other Bowel Diseases Irritable bowel syndrome Alternating diarrhea and constipation Rx: High-fiber diet: be careful with wheat bran Elimination of stimulants Evaluate for food allergies or intolerances © 2004, 2002 Elsevier Inc. All rights reserved. Blind Loop Syndrome Bacterial overgrowth from stasis in intestine, obstruction, radiation enteritis, fistula, or surgical repair Treatment (Rx): Appropriate meds for malabsorption Antibiotics for bacterial overgrowth © 2004, 2002 Elsevier Inc. All rights reserved. Diet Modification of Fiber in Diets Restricted-fiber diet 5 to 10 g/day High-fiber diet 25 to 35 g/day Minimal-residue diet or elemental formulas © 2004, 2002 Elsevier Inc. All rights reserved. Causes of Constipation— Gastrointestinal Diseases of the upper gastrointestinal tract —Celiac disease —Gastric cancer —Duodenal ulcer —Cystic fibrosis Diseases of the large bowel resulting in: —Failure of propulsion along the colon (colonic inertia) —Failure of passage though anorectal structures (outlet obstruction) Irritable bowel syndrome Anal fissures or hemorrhoids Laxative abuse © 2004, 2002 Elsevier Inc. All rights reserved. Causes of Constipation—Systemic Side effect of medication Metabolic endocrine abnormalities, such as hypothyroidism, uremia, and hypercalcemia Lack of exercise Ignoring the urge to defecate Vascular disease of the large bowel Systemic neuromuscular disease leading to deficiency of voluntary muscles Poor diet, low in fiber Pregnancy © 2004, 2002 Elsevier Inc. All rights reserved. Fistula Abnormal Opening Between Organs Causes: birth defects; trauma; inflammatory disease; malignant disease Rx: For fluid loss For electrolyte loss Aggressive nutritional support © 2004, 2002 Elsevier Inc. All rights reserved. Ileostomy or Colostomy Surgical Opening of Intestine to Outside Causes: ulcerative colitis; Crohn’s disease; colon cancer; trauma Rx: Nutrition needs vary with location and individual Avoid gas- or odor-forming foods Fluid and electrolyte needs © 2004, 2002 Elsevier Inc. All rights reserved. Hemorrhoidectomy Delay stool formation until healing can take place Rx: Minimal-residue diet or elemental diet After recovery High-fiber diet to prevent © 2004, 2002 Elsevier Inc. All rights reserved. Summary Lower GI conditions—important for nutritional consequences Important to note where obstruction or surgery has taken place to determine impact on specific nutrients Most dramatic: short bowel syndrome, which may require long-term TPN © 2004, 2002 Elsevier Inc. All rights reserved.