Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
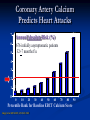
A Cardiologist’s Perspective On Preventing Heart Disease (and Strokes!) C. Michael Wright, MD FACC Medical Director The LifeScore Clinic Outline 1. 2. 3. 4. 5. 6. Cardiovascular Disease (CVD)-Scope of the Problem What is Atherosclerosis? Who is at Risk? How Do We Measure Risk? How Can You Prevent It? Random Cartoons to keep it light! Outline 1. 2. 3. 4. 5. 6. Cardiovascular Disease (CVD)-Scope of the Problem What is Atherosclerosis? Who is at Risk? How Do We Measure Risk? How Can You Prevent It? Random Cartoons to keep it light! 1. Scope of the Problem 102 million with cholesterol >200 50 million with systolic blood pressure >140, diastolic >90 47 million current smokers age 18+ 44 million obese (BMI ≥30) 10 million diabetics Annual direct and indirect cost of CVD - $329 billion in 2002 Strokes 500 000 Heart Attacks 650 000 Heart Failure 550 000 Types of CVD Cardiovascular DiseaseIt’s Big! Outline 1. 2. 3. 4. 5. 6. Cardiovascular Disease (CVD)-Scope of the Problem What is Atherosclerosis? Who is at Risk? How Do We Measure Risk? How Can You Prevent It? Random Cartoons to keep it light! 2. What Is Atherosclerosis? Tunica adventitia Tunica media Tunica intima Endothelium Subendothelial connective tissue Internal elastic membrane Smooth muscle cells Elastic/collagen fibers External elastic membrane Stages of Atherosclerosis Normal Plaque Development Fatty streak Lipid-rich plaque Foam cells Thrombus Lipid core Evolution of Plaque Coronary Wall Dynamics with Plaque Mural Plaque Vessel wall Vessel “lumen” Normal vessel No Narrowing Mild Plaque Mild Narrowing Moderate Plaque Time [years] Severe Narrowing Extensive Plaque Plaque Rupture Thrombus Fibrous Cap Lipid Core IVUS vs. Angiography Outline 1. 2. 3. 4. 5. 6. Cardiovascular Disease (CVD)-Scope of the Problem What is Atherosclerosis? Who is at Risk? How Do We Measure Risk? How Can You Prevent It? Random Cartoons to keep it light! 3. Who is at Risk? Lifestyle Determines Cardiovascular Health Inactivity Refined Carbohydrates Low intake Of Omega 3 High intake of sodium Low intake of Omega 9 Trans fatty acids Oxidative Stress Lipid abnormalities Insulin Resistance Sympathetic activation Inflammation RAS activation Low intake of antioxidants Low intake of Essential minerals Caloric Intake > Caloric expenditure Endothelial Dysfunction & Vascular Injury Atherosclerosis Begins in Childhood % with Coronary Fatty Streaks 100 80 60 40 20 0 2-15 yr olds 21-39 year olds The Bogalusa Heart Study % with Coronary Atheromas 80 70 60 50 40 30 20 10 0 2-15 yr olds 15-20 21-25 26-39 The At Risk Patient Physical Inactivity Risk Factors and Coronary Atherosclerosis in Young Adults The Bogalusa Heart Study Early High TC Levels Associated With Later CHD Events Results After 40 Years No. of CHD events* 40 35.2 35 30 25 17.5 20 11.5 15 10 6.9 5 0 118-172 *1017 men, average age 22 173-189 190-208 TC (mg/dL) Adapted from Klag MJ, et al. N Engl J Med. 1993;328:313-318. 209-315 Outline 1. 2. 3. 4. 5. 6. Cardiovascular Disease (CVD)-Scope of the Problem What is Atherosclerosis? Who is at Risk? How Do We Measure Risk? How Can You Prevent It? Random Cartoons to keep it light! 4. How Do We Measure Risk? EBT Score > 75th 15 hs-CRP + TC/HDL 5 hs-CRP 2.5 TC/HDL 2.35 t-PA Ag 2.15 Fibr 1.8 TC 1.6 Homocysteine 1.6 Lp(a) 1.25 0 Relative risk in men from the Physicians Health Study (highest quartile) 5 10 15 Effect of Risk Factors The Cholesterol Overlap Issue No CHD 35% of CHD occurs In people with TC <200 mg/dL 150 CHD 200 250 Total Cholesterol (mg/dL) 300 CME Monograph Based on an Expert Panel Discussion. Cardiovascular risk stratification using high-sensitivity Creactive protein (hs-CRP), a cardiovascular inflammatory risk marker. Certified Continuing Medical Education Series 2001; April 16, 2001; Castelli WP. Atherosclerosis 1996;S1-S9 Calcium in Plaque Cooper Clinic 6 Year F/U CVD Risk by Calcium Score 27.8 15 Adjusted Relative Risk * n=17,256; 461 events, 17 deaths 12 P < .01 9 7.1 6 3 2.2 2.4 1-15 16-95 1 0 0 96-407 >407 (Abstract # P3) Final Program & Abstracts: AHA - 42nd Annual Conference on Cardiovascular Disease Epidemiology and Prevention. April 23-26, 2002, Honolulu, HA CVD Events By CAC Quartile 25 Calcium Score Percentile 21.5 20 19 No. Events Odds Ratio 15 10 6.2 6 5 1 1 1 1 0 1st 2nd 3rd 4th Quartile Raggi P, Callister TQ, Cooikl B , He Z-X, Lippolis NJ, Russo DJ, Zelinger A, Mahmarian JJ. Identification of patients at increased risk of first unheralded acute myocardial infarction by electron-beam computed tomography. Circulation 2000;101:850-55 MI or SCD with Very High CAC Annual event rate 30 25% 25 17% 20 Cancer Database 12.3% Circ 1998;97:535-43 15 7.1% JACC 2001;37:1551-7 10 5 0 EBT Score >1,000 * Wayhs JACC 2002;39:225-30 Severe SPECT Abn. MWMA Stress Echo Lung Cancer Mortality Outline 1. 2. 3. 4. 5. 6. Cardiovascular Disease (CVD)-Scope of the Problem What is Atherosclerosis? Who is at Risk? How Do We Measure Risk? How Can You Prevent It? Random Cartoons to keep it light! 5. How Can You Prevent It? Discover, Design, Do = 3D Health Discover your risk! If high, then aggressive risk factor management If Moderate, then moderate risk factor management If low, then just try to follow a reasonably healthy lifestyle! Design your goals Do your program to achieve your goals Two Books To Read 10 Key Dietary Guidelines 1. 2. 3. Eat omega-3 Rich Foods - Fatty Fish (salmon, trout, tuna, herring, mackerel); walnuts, canola oil, flaxseeds, green leafy vegetables Eat mono-unsaturated fats - Olive oil (extra virgin), canola oil Get 7 or more servings of vegetables and fruits per day Dietary Guidelines Continued 4. 5. 6. Balance animal protein with vegetable protein- legumes (especially soybeans), nuts Avoid saturated fat by choosing lean meat over fatty meat, low fat over full fat in dairy products Avoid oils high in omega-6 fatty acids (corn, safflower, sunflower, soybean and cottonseed oils) Dietary Guidelines Continued 7. Reduce intake of trans-fatty acids: 1. 2. 3. 4. 5. 8. Most margarines Vegetable shortening Commercial pastries Deep fat fried foods Most prepared snacks, mixes and convenience foods Eat unrefined cereals and grains Dietary Guidelines Continued 9. Drink plenty of water every day 10. Be aware of the sodium content of foods and consume less than 2 grams/day Country Diet Comparisons INTERNATIONAL COMPARISONS reveal that total fat intake is a poor indicator of heart disease risk. What is important is the type of fat consumed. In regions where saturated fats traditionally made up much of the diet (for example, eastern Finland), rates of heart disease were much higher than in areas where monounsaturated fats were prevalent (such as the Greek island of Crete). Crete's Mediterranean diet, based on olive oil, was even better for the heart than the low-fat traditional diet of Japan. January ’03 Scientific American Walter C. Willett and Meir J. Stampfer, professors of epidemiology and nutrition at the Harvard School of Public Health Different Food Pyramids Key Supplements-Omega-3 Fatty Acids Fish oil for DHA and EPA Flaxseed or borage oil for Alpha-linolenic acid DHA eggs Decreased inflammation Decreased arrhythmias Decreased clotting tendencies 1-4 grams a day Key Supplements- Vitamins C and E Reduced risk of neurodegenerative diseases Reduced risk of cataracts E- Inhibits oxidation of LDL cholesterol Prevent progression of atherosclerosis is carotid arteries Doses: Vitamin E- 400-800 IU; Vitamin C500-2,000mg per day Key Supplements- Alpha Lipoic Acid Fat and water-soluble antioxidant Regenerates vitamins C and E Binds toxic metals Improves insulin sensitivity Helps the body use glucose for energy Dose- 100-300 mg/day Key Supplements- Co-enzyme Q10 Fat-soluble antioxidant Involved in energy production in mitochondria Regenerates Vitamins C,E and A Inhibits oxidation of LDL cholesterol, cell membranes, and DNA Improves insulin sensitivity Lowers blood pressure Depleted by statin drugs Dose- 30-90 mg/day (gel) Key Supplements- Folic Acid, Vitamins B6 & B12 Lower homocysteine levels Homocysteine can raise risk for stroke, heart attacks and alzheimer’s disease B6 lowers blood pressure DosesFolic acid 400-800mcg/day B6 100-200mg/day B12 1-2mg/day Key Supplements- L-Carnitine Helps convert fatty acids to energy Transports fatty acids into mitochondria 98% of carnitine in the body is in the heart and muscle cells Slows age-dependent decline in mitochondrial function Slows neuro-degeneration and loss of cognitive function Improves insulin sensitivity Improves thyroid function Key Supplements- L-Carnitine Heart Increases heart’s energy production Reduces heart rate during exercise Reduces size of heart attacks Reduces chest pain (angina) Muscle Increases power and endurance Reduces fatigue Helps maintain and increase muscle mass Speeds recovery time after exercise Key Supplements- Carnosine Two amino acids linked together Blocks glycation (sugar bonding to proteins) Glycated proteins cause stiffness and thickening of artery wall and heart muscle Slows aging in animal models May be useful in treatment of cataracts How much? 1 to 2 grams per day Effects of 10% Weight Loss Exercise! Dr. Ken Cooper, of the Cooper Institute of Aerobic Research, found that exercise was associated with a 40 % reduction in heart attacks in females and a 60 % reduction in heart attacks in males. In another study, he found that people who were in the lower 20 % of cardiovascular fitness had a death rate that was three times higher than the most fit group. The study also showed that men taking up exercise, even after the age of 60, will increase their life expectancy. Exercise capacity and mortality among men referred for exercise testing. Myers J, Prakash M, Froelicher V, Do D, Partington S, Atwood JE. Division of Cardiovascular Medicine, Stanford University Medical Center After adjustment for age, the peak exercise capacity measured in metabolic equivalents (MET) was the strongest predictor of the risk of death among both normal subjects and those with cardiovascular disease. Each 1-MET increase in exercise capacity conferred a 12 percent improvement in survival. CONCLUSIONS: Exercise capacity is a more powerful predictor of mortality among men than other established risk factors for cardiovascular disease. Other Beneficial Effects of Exercise •The risk of developing colon cancer is decreased by half in people who exercise regularly. •Estrogen-dependent cancers (breast, ovarian and endometrial cancers) and prostate cancer are decreased with regular exercise. •The risk of dying from cancer declines sharply as exercise increases. •Regular weight-bearing exercise can reduce the incidence of osteoporosis, a reduction of bone strength (and susceptibility to fractures) responsible for thousands of deaths yearly in the U.S. Diet & Lifestyle-Longitudinal Study Nurses’ Health Study- 84,129 women aged 34-59 During 14 yrs, 1129 cases of CHD (1.3%) Low risk group- non-smokers, BMI <25, ½ drink or more/day, ½ or more/day of moderate or vigorous physical activity, upper 40% for 6 dietary variables (cereal fiber, omega 3 fatty acids, folate, high polyunsat/sat fat ratio, low intake of trans fat, low glycemic load This group had a relative risk of 0.17 compared to women in other groups. Coronary Artery Calcium Predicts Heart Attacks 7 Annual Absolute Risk (%) 6 676 initially asymptomatic patients 32+7 months f/u 5 6.54 4.9 3.62 4 2.64 3 1.92 1.38 2 1 0.36 0.51 0.71 0.99 0 0 10 20 30 40 50 60 70 80 Percentile Rank for Baseline EBCT Calcium Score Raggi et al AHJ 2001;141:193-199 90 LDL Goals LDL-C Lowering With Statins: Reduced CHD Events Secondary Prevention 4S-PL Primary Prevention 25 LIPID-PL 20 4S-Rx 15 CARE-PL CARE-Rx 10 LIPID-Rx 5 WOSCOPS-Rx WOSCOPS-PL AFCAPS-Rx AFCAPS-PL 0 50 70 90 110 130 150 LDL Cholesterol (mg/dL) Adapted from Illingworth DR. Med Clin North Am. 2000;84:23-42. 170 190 210 Heart Protection Study- Vascular Events by LDL Plaque Regression Related to LDL-Lowering % change in lesion volume vs. final LDL achieved +120% 0 – 80% 60 120 200 LDL (mg/dL) Treated Untreated Callister TQ. N Engl J Med 1998;339:1972-78 Suboptimal Therapy (LDL >120 mg/dl) THE END!