Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
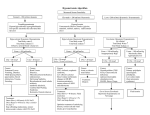
Article fluids & electrolytes Disorders of Water Metabolism in Children: Hyponatremia and Hypernatremia Michael L. Moritz, MD,* Juan Carlos Ayus, MD† Objectives After completing this article, readers should be able to: 1. Describe the clinical manifestations of hyponatremic encephalopathy. 2. Identify the risk factors for developing hyponatremic encephalopathy. 3. List the risk factors for developing cerebral demyelination following the correction of hyponatremia. 4. Characterize the clinical manifestations of hypernatremia. 5. Identify patients at greatest risk for developing hypernatremia. Introduction In conjunction with the tremendous medical advances of the past century, an increasing number of hospitalized patients are dependent on parenteral fluids. Caring for children who have complex medical conditions has resulted in new challenges for prescribing parenteral therapy to maintain sodium and water homeostasis; most electrolyte disturbances occur in the hospital. Although the kidneys play an important role in the development of disorders in water handling, most of the morbidity and mortality results from central nervous system dysfunction (Table 1). This review discusses common disorders of water metabolism, emphasizing the neurologic sequelae. Hyponatremia Hyponatremia is defined as a serum sodium level less than 135 mEq/L (135 mmol/L). It is one of the most common electrolyte disorders encountered in hospitals, occurring in approximately 3% of hospitalized children. The cause usually is identified easily, and the condition rarely is fatal, but sometimes the cause can be elusive and mortality can result from inappropriate therapy. Pathogenesis Under normal circumstances, the human body can maintain plasma sodium levels within the normal range (135 to 145 mEq/L [135 to 145 mmol/L]), despite wide fluctuations in fluid intake. The body’s primary defense against developing hyponatremia is the kidney’s ability to generate dilute urine and excrete free water. The primary reasons that children develop hyponatremia encompass underlying conditions that impair the kidney’s ability to excrete free water (Table 2). Hyponatremia usually occurs in the setting of excess water intake, with or without sodium losses, in the presence of impaired free water excretion. Only under the most extreme circumstances can excess water intake or sodium loss alone lead to hyponatremia in the absence of impaired free water excretion. It is important to realize that the serum sodium concentration does not reflect total body sodium content accurately. Rather, a decrease in serum sodium more closely reflects an increase in total body water, and an increase in serum sodium reflects a free water deficit. Diagnostic Approach Before embarking on an aggressive therapeutic regimen, it is vital to confirm that hyponatremia is associated with hypo-osmolality. Hyponatremia can be associated with either a normal or an elevated serum osmolality (Fig. 1). The most common causes are hyperglycemia, severe hyperproteinemia, or hyperlipidemia. Hyperglycemia results in *Assistant Professor of Pediatric Nephrology, Children’s Hospital of Pittsburgh, Pittsburgh, PA. † Professor of Medicine, University of Texas Health Science Center at San Antonio, San Antonio, TX. Pediatrics in Review Vol.23 No.11 November 2002 371 fluids & electrolytes hyponatremia & hypernatremia Abnormalities of Water Metabolism Leading to Brain Damage Table 1. Hyponatremia ● Syndrome of inappropriate secretion of antidiuretic hormone ● Postoperative ● Oral water intoxication ● Diuretics Hypernatremia ● ● ● ● Gastroenteritis Fluid restriction Diabetes insipidus Sodium excess hyperosmolality, with a translocation of fluid from the intracellular space to the extracellular space, resulting in a 1.6-mEq/L (1.6-mmol/L) decrease in levels of serum sodium for every 100 mg/dL (5.6 mmol/L) elevation in serum glucose concentration above normal. Severe hyperlipidemia and hyperproteinemia can cause a displacement of plasma water, which will result in a decreased sodium concentration (pseudohyponatremia) with a normal serum osmolality. Serum sodium levels currently are measured by either direct- or indirect-reading ion- Disorders of Impaired Renal Water Excretion Table 2. Effective Circulating Volume Depletion ● ● ● Gastrointestinal losses: vomiting, diarrhea Skin losses: cystic fibrosis Renal losses: salt-wasting nephropathy, diuretics, cerebral salt wasting, hypoaldosteronism ● Edematous states: heart failure, cirrhosis, nephrosis, hypoalbuminemia Thiazide Diuretics Renal Failure ● ● Acute Chronic Nonhypovolemic States of Antidiuretic Hormone Excess ● Syndrome of inappropriate secretion of antidiuretic hormone ● Cortisol deficiency ● Hypothyroidism 372 Pediatrics in Review Vol.23 No.11 November 2002 selective electrode potentiometry. The direct method will not indicate pseudohyponatremia because it measures the activity of sodium in the aqueous phase of serum only. The indirect method may indicate pseudohyponatremia because the specimen is diluted with a reagent prior to measurement. The indirect method is performed in approximately 60% of chemistry laboratories in the United States; therefore, pseudohyponatremia remains an entity of which clinicians must be aware. If hyponatremia is associated with hypoosmolality (true hyponatremia), the next step is to measure the urinary osmolality to determine if there is an impaired ability to excrete free water (urineOsm ⬎100mOsm/kg). The most useful information for correctly diagnosing hyponatremia is a detailed history of fluid balance, weight changes, medications (especially diuretics), and underlying medical illnesses. Hyponatremia usually is a multifactorial disorder, and a detailed history can identify sources of salt and water losses, free water ingestion, and underlying illnesses that prompt a nonosmotic stimulus for vasopressin production. Assessment of the volume status on physical examination and the urinary electrolytes on laboratory evaluation can be extremely helpful, but both findings can be misleading. For patients in whom hyponatremia is due to salt losses, such as from diuretics, signs of volume depletion may be absent on physical examination because the volume deficit may be nearly corrected by oral intake of hypotonic fluids if the thirst mechanism is intact. In general, a urinary sodium concentration less than 25 mEq/L (25 mmol/L) is consistent with effective circulating volume depletion, and a concentration greater than 25 mEq/L (25 mmol/L) is consistent with renal tubular dysfunction, use of diuretics, or the syndrome of inappropriate antidiuretic hormone secretion (SIADH) (Fig. 1). Numerous factors can affect the urine sodium, making interpretation difficult. Therefore, the timing of the urinary measurements in relation to dosages of diuretics, intravenous fluid boluses, or fluid and sodium restriction is important. Clinical Manifestations A major consequence of hyponatremia is influx of water into the intracellular space, resulting in cellular swelling that can lead to cerebral edema and encephalopathy. The clinical manifestations of hyponatremia are primarily neurologic and related to cerebral edema caused by hypo-osmolality (Table 3). The symptoms of hyponatremic encephalopathy vary substantially among individuals; the only consistent symptoms are headache, nausea, fluids & electrolytes hyponatremia & hypernatremia Figure 1. Diagnostic approach to hyponatremia. vomiting, emesis, and weakness. As the cerebral edema worsens, patients develop behavioral changes and an impaired response to verbal and tactile stimuli. Advanced symptoms include signs of cerebral herniation, such as seizures, respiratory arrest, dilated pupils, and decorticate posturing. Not all patients have the usual progression in symptoms; advanced symptoms can develop suddenly. Children are at particularly high risk for developing symptomatic hyponatremia. They develop hyponatremic encephalopathy at higher serum sodium concentrations than do adults and have a poor prognosis if timely therapy is not initiated. This appears to be due to the higher brain-to-skull size ratio in children, which leaves less room for brain expansion (Fig. 2). Children’s brains reach adult dimensions by 6 years of age, but the full skull size is not reached until 16 years of age. Also, animal data suggest that prepubertal children have an impaired ability to regulate brain cell volume due to diminished cellular sodium extrusion related to lower testosterone levels. Hypoxemia is another major risk factor for developing hyponatremic encephalopathy. The occurrence of a hypoxic event, such as respiratory insufficiency, is a major factor militating against survival without permanent brain damage in patients who have hyponatremia. The combination of systemic hypoxemia and hyponatremia is more deleterious than is either factor alone because hypoxemia impairs the ability of the brain to adapt to hyponatremia, leading to a vicious cycle of worsening hyponatremic encephalopathy (Fig. 3). Hyponatremia leads to decreased cerebral blood flow and arterial oxygen content. Patients who have symptomatic hyponatremia can develop hypoxemia by at least two different mechanisms: noncardiogenic pulmonary edema or hypercapnic respiratory failure. Respiratory failure can occur suddenly in patients who have symptomatic hyponatremia. Most of the neurologic morbidity reported for children who have hyponatremia has occurred in patients who have had a respiratory arrest as a feature of hyponatremic encephalopathy. Of the many conditions that have been associated with hyponatremia, only a few are likely to lead to symptomatic hyponatremia. SIADH SIADH is one of the most common causes of hyponatremia in the hospital and frequently leads to severe hyponatremia (plasma sodium, ⬍120 mEq/L [120 mmol/ L]). It is caused by elevated ADH secretion in the absence of an osmotic or hypovolemic stimulus. SIADH Pediatrics in Review Vol.23 No.11 November 2002 373 fluids & electrolytes hyponatremia & hypernatremia Anatomic Changes and Clinical Symptoms of Hyponatremic Encephalopathy Table 3. Anatomic Changes Brain swelling Pressure on rigid skull Tentorial herniation Clinical Symptoms Headache Nausea Vomiting Seizures Respiratory arrest loop diuretics. Vasopressin 2 receptor antagonists are a promising therapy that are under investigation but are not approved for clinical use. Postoperative Hyponatremia Deaths due to hyponatremic encephalopathy have been reported in healthy children following routine surgical procedures. Patients develop hyponatremia postoperatively due to a combination of nonosmotic stimuli for ADH release, such as subclinical volume depletion, pain, nausea, stress, edema-forming conditions, and administration of hypotonic fluids. The postoperative nonosmotic stimuli for ADH release usually resolve by the third postoperative day, but they can persist until the fifth postoperative day. The most important factors leading to postoperative hyponatremia are failure to recognize the compromised ability of the patient to maintain water balance and the administration of hypotonic fluids. All postoperative patients should be considered at risk for developing hyponatremia, and prophylactic measures should include avoidance of hypotonic fluids and administration of normal saline unless a free water deficit is present. Serum electrolytes should be monitored postoperatively in patients receiving intravenous fluids, and physicians should be alert to signs of symptomatic hyponatremia. can be associated with a variety of illnesses, but most often it is due to central nervous system disorders, pulmonary disorders, and medications (Table 4). Among the latter, the chemotherapeutic drugs vincristine and cyclophosphamide and the antiepileptic drug carbamazepine are especially common. SIADH is essentially a diagnosis of exclusion. Before it can be diagnosed, diseases causing decreased effective circulating volume, renal impairment, adrenal insufficiency, and hypothyroidism must be excluded. The hallmarks of SIADH are: mild volume expansion with low-to-normal plasma concentrations of creatinine, urea, uric acid, and potassium; impaired free water excretion with normal sodium excretion that reflects sodium intake; and hyponatremia that is relatively unresponsive to sodium administration in the absence of fluid restriction. SIADH usually is of short duration and resolves with treatment of the underlying disorder and discontinuation of the offending medication. Fluid restriction is the cornerstone of therapy, but it represents a slow method of correction and frequently is impractical in infants who receive most of their nutrition in liquid form. All intravenous fluids should be of a tonicity of at least normal saline; if this does not correct the plasma sodium, 3% sodium chloride may be administered as needed. If more rapid correction of hyponatremia is needed, the addition of a loop diuretic in combination with hypertonic fluids is useful. Agents that produce diabetes insipidus, such as demeclocycline, can be used if SIADH persists for more than 1 month and is unresponsive to fluid restriction, increased sodium intake, and Figure 2. Effects of physical factors on hyponatremic encephalopathy. 374 Pediatrics in Review Vol.23 No.11 November 2002 fluids & electrolytes hyponatremia & hypernatremia Table 4. Causes of SIADH Central Nervous System Disorders ● ● ● ● ● ● Infection: meningitis, encephalitis Neoplasms Vascular abnormalities Psychosis Hydrocephalus Postpituitary surgery Pulmonary Disorders ● ● ● ● ● Pneumonia Tuberculosis Asthma Positive pressure ventilation Pneumothorax Carcinomas ● ● ● ● ● Bronchogenic carcinomas Oat cell of the lung Duodenal Pancreatic Neuroblastoma Medications ● ● ● ● 3. Effects encephalopathy. Figure of hypoxemia on Vincristine Intravenous cyclophosphamide Carbamazepine Serotonin reuptake inhibitors hyponatremic Oral Water Intoxication in Infants Water intoxication is one of the most common causes of symptomatic hyponatremia in healthy infants; 70% of infants younger than 6 months of age who develop seizures that have no apparent cause are found to have hyponatremia due to water intoxication. Most of these infants are living in poverty and develop water intoxication when caregivers either dilute formula inappropriately or supplement feedings with water. Because an infant’s caloric intake depends almost entirely on a liquid diet, hunger will drive the infant to accept a low-solute formula to the point of water intoxication. Infants typically present with generalized tonic-clonic seizures, respiratory insufficiency, and hypothermia. Affected infants may be managed with rapid and partial correction of hyponatremia via administration of hypertonic or normal saline. The hyponatremia corrects rapidly due to a free water diuresis, and it corrects spontaneously in many infants after they resume normal feeding. With appropriate treatment, the prognosis generally is good without long-term neurologic sequelae. Diuretics Diuretics are a relatively common cause of hyponatremia in children, with severe and symptomatic hyponatremia occurring primarily in patients receiving thiazide diuretics. Thiazide diuretics can cause both acute and chronic hyponatremia, but typically hyponatremia develops in the first few weeks following the initiation of therapy. Thiazide diuretics frequently are employed to manage edema-forming states, and the effects of the diuretic are synergistic with other underlying disorders that cause hyponatremia. Excess water intake also is a major contributing factor to the development of hyponatremia among those receiving diuretics. Treatment In general, if there are no neurologic manifestations of hyponatremia, correction with hypertonic saline is unnecessary and potentially harmful. Symptomatic hyponatremia, on the other hand, is a medical emergency. Once signs of encephalopathy are identified, prompt treatment is required in a monitored setting before imaging studies are performed. Fluid restriction alone has no place in the treatment of symptomatic hyponatremia. Affected paPediatrics in Review Vol.23 No.11 November 2002 375 fluids & electrolytes hyponatremia & hypernatremia tients should be treated with hypertonic saline (3%) at a dose of 514 mEq/L administered by an infusion pump. The rate of infusion should raise the plasma sodium concentration by about 1 mEq/L (1 mmol/L) per hour until either the patient becomes alert and seizure-free, the plasma sodium level increases by 20 to 25 mEq/L (20 to 25 mmol/L), or a serum sodium concentration of approximately 125 to 130 mEq/L (125 to 130 mmol/L) is achieved, whichever occurs first. If the patient is seizing or showing other signs of increased intracranial pressure, the infusion rate should be increased to raise the serum sodium level by 4 to 8 mEq/L (4 to 8 mmol/L) during the first hour or until the seizure activity ceases. Assuming that total body water comprises 50% of total body weight, 1 mL/kg of 3% sodium chloride in water will raise the plasma sodium by about 1 mEq/L (1 mmol/L). Cerebral Demyelination Brain damage and cerebral demyelination can develop if there is an excessive change in serum sodium levels. Cerebral demyelinating lesions are a rare but recognized complication of therapy for hyponatremic encephalopathy. They typically occur several days following the correction of hyponatremia and can present with confusion, quadriplegia, pseudobulbar palsy, and a pseudocoma with a “locked in” stare. In many cases, they are asymptomatic. The lesions are diagnosed best on magnetic resonance imaging performed at least 2 weeks following the correction of hyponatremia. The incidence of cerebral demyelination is unclear because most reported cases failed to document the demyelination. Recent data demonstrated that the rate of correction has little or no relationship to the development of demyelinating lesions; rather, the absolute magnitude of correction and the underlying illnesses are the major contributing factors. Hyponatremic patients who develop demyelinating lesions have either: a) been made hypernatremic inadvertently, b) had their plasma sodium levels corrected by greater than 25 mmol/L in 24 to 48 hours, c) suffered a hypoxic event, or d) had severe liver disease. Because the risk of death and permanent neurologic damage in untreated hyponatremia far exceeds the theoretical possibility of demyelinating lesions following correction, clinicians should not hesitate to use hypertonic saline in symptomatic patients. Hypernatremia Hypernatremia is defined as a serum sodium concentration greater than 145 mEq/L (145 mmol/L). In both children and adults, hypernatremia is seen primarily in hospitals and occurs in individuals who have restricted access to water for a variety of reasons. Typically, affected patients are either debilitated by an acute or chronic illness, have neurologic impairment, or are at the extremes of age. Infants, especially those born preterm, are at particularly high risk for the development of hypernatremia because of their relatively small mass-to-surface area ratio and their dependency on a caretaker to administer fluids. Gastroenteritis remains an important cause of hypernatremia in children, but it is much less common than previously reported. Ineffective breastfeeding is a rare cause of hypernatremia, but the incidence appears to be increasing. It primarily occurs in primiparous welleducated mothers, who fail to recognize progressive malnutrition and dehydration. Significant vascular complications have been reported in these infants. Unlike mild chronic hyponatremia, which may be physiologic in certain Excess water intake is a major contributing factor to the development of hyponatremia among those receiving diuretics. 376 Pediatrics in Review Vol.23 No.11 November 2002 edematous diseases, a serum sodium concentration greater than 145 mEq/L (145 mmol/L) always should be considered abnormal and evaluated thoroughly. Pathogenesis The body has two defenses to protect against developing hypernatremia: the ability to produce a concentrated urine and a powerful thirst mechanism. ADH release occurs when the plasma osmolality exceeds 275 to 280 mOsm/kg (275 to 280 mmol/kg) and results in a maximally concentrated urine when the plasma osmolality exceeds 290 to 295 mOsm/kg (290 to 295 mmol/ kg). Thirst is the body’s second line of defense, but it provides the ultimate protection against hypernatremia. If the thirst mechanism is intact and access to free water is unrestricted, it is rare for a person to develop sustained hypernatremia from either excess sodium ingestion or a renal concentrating defect. fluids & electrolytes hyponatremia & hypernatremia Figure 4. Diagnostic approach to hypernatremia. Diagnosis Hypernatremia is usually multifactorial, and a systematic approach is required to determine the contributing factors (Fig. 4). Serum sodium, glucose, and osmolality levels must be measured. An elevated serum sodium concentration always is associated with hyperosmolality and should be considered abnormal. In cases of significant hyperglycemia, the serum sodium concentration will be depressed due to the associated translocation of fluids from the intracellular to extracellular space. Once hypernatremia has been diagnosed, a detailed history should be taken and fluid intake reviewed to determine if the patient has an intact thirst mechanism, has restricted access to fluids, or is not being provided adequate free water in intravenous fluids. Urine volume should be measured and compared with fluid intake, and the urine osmolality and electrolyte levels should be determined to assess if the renal concentrating ability is appropriate and to quantify the urinary free water losses. A less than maximally concentrated urine (⬍800 mOsm/kg [800 mmol/L]) in the face of hypernatremia is a sign of a renal concentrating defect because hypernatremia is a maximal stimulus for ADH release. For patients who have hypernatremia, the following should be evaluated: gastrointestinal losses, dermal losses from fever or burns, diet history (including enteral feedings), medication history (including diuretics), and sources of exogenous sodium. Clinical Manifestations and Mortality Hypernatremia results in an efflux of fluid from the intracellular space to the extracellular space to maintain osmotic equilibrium. This leads to transient cerebral dehydration and cell shrinkage. Brain cell volume can decrease by as much as 10% to 15% acutely, but it adapts quickly. Within 1 hour, the brain significantly increases its intracellular content of sodium and potassium, amino acids, and unmeasured organic substances (idiogenic osmoles). Within 1 week, the brain regains approximately 98% of its water content. If severe hypernatremia develops acutely, the brain may not be able to increase its intracellular solute sufficiently to preserve its volume, and the resulting cellular shrinkage can cause structural changes. Cerebral dehydration from hypernatremia can result in a physical separation of the brain from the meninges, leading to rupture of the delicate bridging veins and intracranial or intracerebral hemorrhages. Venous sinus thrombosis progressing to infarction also can develop. Acute hypernatremia also has been shown to cause cerebral demyelinating lesions in both animals and humans. Patients who have hepatic encephalopathy are at the highest risk for developing such lesions. Children who have hypernatremia usually appear agitated and irritable, but these symptoms can progress to lethargy, listlessness, and coma. Neurologic examination frequently reveals increased tone, nuchal rigidity, and brisk reflexes. Myoclonus, asterixis, and chorea can be present; tonic-clonic and absence seizures have been described. Hyperglycemia is a particularly common consequence of hypernatremia in children. Severe hypernatremia also can result in rhabdomyolysis. Although earlier reports showed that hypocalcemia was associated with hypernatremia, this has not been found in more recent literature. Hypernatremia is associated with a mortality rate of 15% in children, which is estimated to be 15 times higher than the age-matched mortality in hospitalized children who do not have hypernatremia. The high mortality rate Pediatrics in Review Vol.23 No.11 November 2002 377 fluids & electrolytes hyponatremia & hypernatremia Management of Hypernatremia circulatory collapse, fluid resuscitation with normal saline or colloid should be instituted before correctCause Treatment* ing the free water deficit. The type A. Sodium and water loss 0.45% Sodium chloride in 5% dextrose of therapy depends largely on the ● Gastroenteritis in water cause of the hypernatremia and B. Primary water loss 0.2% Sodium chloride in 5% dextrose in ● Ineffective breastfeeding water should be tailored to the pathoC. Nephrogenic diabetes insipidus 0.1% Sodium chloride in 2.5% dextrose physiologic events involved in each in water (acute management) patient (Table 5). Oral hydration D. Central diabetes insipidus Desmopressin acetate should be instituted as soon as it E. Sodium overload 5% dextrose in water can be tolerated safely. Plasma elecDiuretics or dialysis may be needed trolytes should be measured every *Avoid 5% dextrose in water if hyperglycemia is present. 2 hours until the patient is neurologically stable. The rate of correction of hyperis unexplained. Most of the deaths are not related directly natremia depends largely on the severity of hypernatreto central nervous system pathology and appear to be mia and its cause. Due to the relative inability of the brain independent of the severity of hypernatremia. Recent to extrude idiogenic osmoles, rapid correction of hyperstudies have noted that patients who develop hypernatrenatremia can lead to cerebral edema. Although no definmia following hospitalization and patients in whom itive studies document the optimal rate of correction that treatment is delayed have the highest mortality. Approxcan be undertaken without developing cerebral edema, imately 40% of the deaths in children occurred while empiric data have shown that unless symptoms of hyperpatients were still hypernatremic. natremic encephalopathy are present, a rate of correction not exceeding 1 mEq/h or 15 mEq/24 h is reasonable. Treatment In severe hypernatremia (sodium, ⬎170 mEq/L The goal of therapy for hypernatremia is to correct both [170 mmol/L]), serum sodium should not be corrected the serum sodium level and the circulatory volume. The to below 150 mEq/L (150 mmol/L) in the first 48 to cornerstone is provision of adequate free water to correct 72 hours. It is not uncommon for seizures to occur the serum sodium level. The free water deficit cannot be during the correction of hypernatremia; they may be a assessed easily by physical examination in children who sign of cerebral edema. They usually can be managed by have hypernatremic dehydration because most of the slowing the rate of correction or by administering hyperwater losses are intracellular. Accordingly, the signs of tonic saline to increase the serum sodium concentration volume depletion are less pronounced due to better slightly. The seizures are usually self-limited and not a preservation of the extracellular volume. A simple sign of long-term neurologic sequelae. Patients who have method of estimating the minimum amount of fluid acute hypernatremia that is corrected by the oral route necessary to correct the serum sodium is by the following can tolerate a more rapid rate of correction with a much equation: lower incidence of seizures. Table 5. Free water deficit (mL) ⫽ 4 mL ⫻ lean body weight (kg) ⫻ [desired change in serum sodium mEq/L (mmol/L)] Larger amounts of fluid will be required, depending on the fluid composition. To correct a 3-L free water deficit, approximately 4 L of 0.2% sodium chloride in water or 6 L of 0.45% sodium chloride in water would be required because they contain approximately 75% and 50% free water, respectively. The calculated deficit does not account for insensible losses or ongoing urinary or gastrointestinal losses. Maintenance fluids, which include replacement of urine volume with hypotonic fluids, are given in addition to the deficit. If there are signs of 378 Pediatrics in Review Vol.23 No.11 November 2002 Suggested Reading Arieff AI. Central nervous system manifestations of disordered sodium metabolism. Clin Endocrinol Metab. 1984;13:269 –293 Arieff AI, Ayus JC, Fraser CL. Hyponatraemia and death or permanent brain damage in healthy children. BMJ. 1992;304:1218–1222 Ayus JC, Arieff AI. Chronic hyponatremic encephalopathy in postmenapausal women: association of therapies with morbidity and mortality. JAMA. 1999;281:2299 –2304 Ayus JC, Arieff AI. Pathogenesis and prevention of hyponatremic encephalopathy. Endocrinol Metab Clin North Am. 1993;22: 425– 446 Ayus JC, Arieff AI. Pathogenesis and treatment of hypoosmolar and hyperosmolar states. In: Suki WN, Massry SG, eds. Suki and fluids & electrolytes hyponatremia & hypernatremia Massry: Therapy of Renal Diseases and Related Disorders. 3rd ed. Boston, Mass: Kluwer Academic Publishers; 1997:1–19 Ayus JC, Arieff AI. Pulmonary complications of hyponatremic encephalopathy: noncardiogenic pulmonary edema and hypercapnic respiratory failure. Chest. 1995;107:517–521 Ayus JC, Krothapalli RK, Arieff AI. Treatment of symptomatic hyponatremia and its relation to brain damage. A prospective study. N Engl J Med. 1987;317:1190 –1195 Ayus JC, Wheeler JM, Arieff AI. Postoperative hyponatremic encephalopathy in menstruant women. Ann Intern Med. 1992; 117:891– 897 Bartter FC, Schwartz WB. The syndrome of inappropriate secretion of antidiuretic hormone. Am J Med. 1967;42:790 – 806 Fraser CL, Arieff AI. Epidemiology, pathophysiology, and management of hyponatremic encephalopathy. Am J Med. 1997;102: 67–77 Cooper WO, Atherton HD, Kahana M, et al. Increased incidence of severe breastfeeding malnutrition and hypernatremia in a metropolitan area. Pediatrics. 1995;96:957–960 Keating JP, Schears GJ, Dodge PR. Oral water intoxication in infants: an American epidemic. Am J Dis Child. 1997;145: 985–990 Moritz ML, Ayus JC. The changing pattern of hypernatremia in hospitalized children. Pediatrics. 1999;104:435– 439 Morris-Jones PH, Houston IB. Prognosis of the neurological complication of acute hypernatremia. Lancet. 1967;2:1385– 1389 Rose DR. Hyperosmolal states– hypernatremia. In: Clinical Physiology of Acid-Base and Electrolyte Disorders. 4th ed. New York, NY: McGraw-Hill, Inc; 1994:695–736 Rose DR. Hypoosmolal states– hyponatremia. In: Clinical Physiology of Acid-Base and Electrolyte Disorders. 4th ed. New York, NY: McGraw-Hill, Inc; 1994:651– 694 Sarnaik AP, Meert K, Hackbarth R, Fleischmann L. Management of hyponatremic seizures in children with hypertonic saline: a safe and effective strategy. Crit Care Med. 1994;19:758 –762 Weisberg LS. Pseudohyponatremia: a reappraisal. Am J Med. 1989; 86:315–318 Please note that the deadline for submission of your answer sheets for the quizzes in the issues of 2002 has been extended to January 31, 2003. Pediatrics in Review Vol.23 No.11 November 2002 379 fluids & electrolytes hyponatremia & hypernatremia PIR Quiz Quiz also available online at www.pedsinreview.org. 1. A 9-month-old girl presents with a 5-day history of severe, watery diarrhea. She is irritable and appears clinically dehydrated, although less than would be expected from her history. Her mental status deteriorates, and she appears comatose. Her serum sodium level is 184 mEq/L (184 mmol/L). The most likely mechanism for this acute change is: A. B. C. D. E. Brainstem herniation. Cerebral edema. Cerebral hypoxia. Demyelination. Intracranial hemorrhage. 2. A 5-year-old boy in the intensive care unit experiences seizures 2 days following cardiac surgery. His serum sodium concentration is 117 mEq/L (117 mmol/L). Other expected laboratory values would include: A. Decreased plasma osmolality (<280 mOsm/kg H2O [280 mmol/kg H2O]); decreased urine osmolality (<100 mOsm/kg H2O [100 mmol/kg H2O]). B. Decreased plasma osmolality (<280 mOsm/kg H2O [280 mmol/kg H2O]); increased urine osmolality (>100 mOsm/kg H2O [100 mmol/kg H2O]). C. Increased plasma osmolality (>280 mOsm/kg H2O [280 mmol/kg H2O]); decreased urine osmolality (<100 mOsm/kg H2O [100 mmol/kg H2O]). D. Increased plasma osmolality (>280 mOsm/kg H2O [280 mmol/kg H2O]); increased urine osmolality (>100 mOsm/kg H2O [100 mmol/kg H2O]). E. Normal plasma osmolality; normal urine osmolality. 3. The mother of a 3-month-old boy is concerned that “he is too weak and won’t gain weight!” He was born at 25 weeks’ gestation and had chronic lung disease that was treated with diuretics. Laboratory studies demonstrate that he is hyponatremic. The best laboratory study to assess the contributing effect of the diuretics further is: A. B. C. D. E. Plasma osmolality. Serum blood urea nitrogen. Serum creatinine. Urine osmolality. Urine sodium. 4. A 9-year-old boy who has cerebral palsy is admitted to the hospital following 4 days of diarrhea. His initial serum sodium level is 174 mEq/L (174 mmol/L). Once circulatory volume is restored, the primary focus of the fluid management must be to provide appropriate amounts of: A. B. C. D. E. Chloride. Free water. Glucose. Phosphate. Potassium. 5. Children who have hypernatremic dehydration often appear minimally dehydrated on clinical examination. This feature is due to maintenance of: A. B. C. D. E. Extracellular fluid volume. Intracellular fluid volume. Total body glucose. Total body sodium concentration. Total body water balance. 380 Pediatrics in Review Vol.23 No.11 November 2002