Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
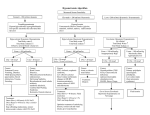
Diagnosis and Treatment of Hyponatremia Acute: Symptomatic Chronic: Asymptomatic Thomas DuBose,M.D. Professor and Chair, Internal Medicine Wake Forest University School of Medicine Hyponatremia: ICU Pseudohyponatremia • Hyperglycemia, Hyperlipidemia Post-operative Hyponatremia SIADH Cerebral Salt Wasting Mechanical Ventilation Cirrhosis Congestive Heart Failure SIRS/MODS Loop diuretics with hypotonic fluid replacement Certain drug intoxications Agents that enhance ADH release or action Major Causes of Hyponatremia EIVF Depletion SIADH Hormone mediated Adrenal Insufficiency Hypothyroidism Pregnancy Disorders in which ADH levels may be appropriately suppressed True Volume Depletion CHF or Cirrhosis Advanced renal failure Primary polydipsia Beer drinker’s potomania Pseudohyponatremia High plasma osmolality: hyperglycemia, mannitol, urea Normal plasma osmolality: hyperlipidemia, hyperproteinemia, glycine infusion. Steps in the Evaluation of Hyponatremia Calculate plasma osmolality Measure plasma osmolality • • Evaluate volume status of patient • • • When low; defines true hypo-osmolal state or clinical hyponatremia Consider plasma glucose, protein and lipids Volume depletion Volume expansion Euvolemia Measure urine sodium Estimating the Serum Osmolality BUN GLUCOSE 2[Na ]p 2.8 18 In Spurious Hyponatremia: Calculated OSMp < Determined OSMp Spurious Hyponatremia (hyperlipemia, hyperproteinemia) is not a hypoosmolar state. Causes of Hypoosmolality Volume Depletion • • • • • Volume Expansion • GI, lung or skin losses Third space sequestration Adrenal insufficiency Renal salt wasting Cerebral salt wasting CHF, cirrhosis with ascites, nephrotic syndrome Euvolemic • SIADH, water intoxication, reset osmostat, drugs Antidiuretic Drugs Antidiuretic hormones: Vasopression Oxytocin Diuretics: Thiazides Furosemide Ethacrynic acid CNS-active drugs: Vincristine Carbamazepine Psychotropic drugs Inhibitors of prostaglandin synthesis: Chlorpropamide Salicylates Acetaminophen Nonsteroidal anti-inflammatory agents COX 2 inhibitors Others: Clofibrate Cyclophosphamide Somatostatin Ecstasy Syndrome of Inappropriate ADH Release (Bartter’s Criteria) Hyponatremia and true hypoosmolality by definition Euvolemia clinical Urine less than maximally dilute (urinary osmolality usually > 200 mOsm/kg of H2O) Normal renal, cardiac, hepatic, adrenal, pituitary, and thyroid function No history of antidiuretic drugs No emotional or physical stress Urinary sodium > 20 mEq/litera a Urinary sodium may be <20 mEq/liter if the patient is volume deleted or on low sodium intake. Disorders Associated With SIADH Carcinomas Pulmonary disorders Central nervous system disorders Most Common Causes of SIADH in Elderly (CDP and NHR)* Medications Idiopathic form Malignancies *Aging Clin Exp Res 2003, 15:6-11. Disorders Associated With SIADH: Carcinomas Small cell carcinoma of the lung Carcinoma of the duodenum Carcinoma of the pancreas Thymoma Lymphoma Ewing’s sarcoma Mesothelioma Carcinoma of the bladder Prostatic carcinoma Olfactory neuroblastoma Disorders Associated With SIADH: Pulmonary Disorders Viral pneumonia Bacterial pneumonia Pulmonary abscess Tuberculosis Aspergillosis Positive-pressure breathing Asthma Pneumothorax Cystic fibrosis Lung cancers Disorders Associated With SIADH: Central Nervous Disorders Encephalitis (viral or bacterial Meningitis (viral, bacterial, tuberculosis, fungal) Head trauma Brain abscess Brain tumors Guillain-Barré syndrome Acute intermittent porphyria Subarachnoid hemorrhage or subdural hematoma Cerebellar and cerebral atrophy Cavernous sinus thrombosis Neonatal hypoxia Hydrocephalus Shy-Drager syndrome Rocky Mountain spotted fever Delirium tremens Cerebrovascular accident (cerebral thrombosis or hemorrhage) Acute psychosis Peripheral neuropathy Multiple sclerosis Guiding Principles in the Treatment of Hyponatremia 1. Neurologic disease can follow both the failure to promptly treat as well as injudiciously rapid treatment of hyponatremia. 2. Presence or absence of significant neurologic signs and symptoms must guide treatment. 3. Acuity or chronicity of the electrolyte disturbance impacts the rate at which the correction should be undertaken. A Prudent Approach to the Treatment of Hyponatremia - 1 Acute Symptomatic Hyponatremia (duration < 48 hours) 1. 2. 3. 4. 5. Risk for complication of cerebral edema greater than risk of treatment of complication. Treat with hypertonic NaCl: 3% NaCl @ 12 mL/kg/hr or 2 mEq/L/hr. until convulsions subside. Usually means increasing [Na+] by 10%. Alternative: furosemide and hypertonic NaCl Full correction is dangerous. Correct by 10% or to 120-122 mEq/L slowly. Then initiate water restriction. A Prudent Approach to the Treatment of Hyponatremia - 2 Symptomatic Hyponatremia (Chronic or Unknown Duration) 1. Increase serum sodium by 10%, that is, approximately 10 mEq/L and then water restrict. Usually 1 -2 mL/kg/hr of hypertonic saline. 2. Do not exceed a correction rate of 1.5 mEq/L/hr at any given time. 3. Do not increase serum sodium by more than 15 mEq/day. 4. Long-term • H2O restriction • Demeclocycline 300 - 600 mg bid • V2 receptor antagonist? Aquaretics Therapeutic Strategy Based On Volume Status of Patient Presence of Absence of Symptoms Duration of Hypoosmolality Presence of absence of risk factors for development of neurological complication Osmotic demyelination is rare in patients with initial Na+ > 120mEq/L A Prudent Approach to the Treatment of Hyponatremia - 3 Asymptomatic Hyponatremia 1. Almost always chronic. 2. Treat with water restriction regardless of how low the serum sodium. Calculating Sodium Requirement in Hyponatremia In correcting hyponatremia the approximate expansion of total body water must be determined first by calculating the volume of water which was required to dilute the serum sodium concentration to its observed value. For example, in a 70 kg patient with a serum Na+ concentration of 120 mEq/L rather than 140 mEq/L, this calculation is made as follows: Body water in normal state = (70 kg) (0.60) = 42 L Body water in abnormal state = (x) (120) = (42)(140) = 49L Excess body water = 7 L The amount of Na+ in milliequivalents required for correction can then be calculated; again it is necessary to assume Na+ is distributed throughout the total body water. (140-patient’s - Na+) (calculated total body water) = total Na+ requirement. How to predict the effect of therapy on the patient’s serum sodium [Na ] Pa tien t [Na ] Bot [Na ] Patient TBW 1 The Bottle: 0.9% = 154 mEq/L Ringer’s = 130 mEq/L 0.45% = 77 mEq/L 3% = 513 mEq/L Diagnosis and Treatment of Hypernatremia Steps in Evaluation of Hypernatremia Establish history of water intake, and integrity of thirst mechanism Severe hypernatremia is unusual unless thirst mechanism is defective or water is not available to the patient. Determine patient’s volume status Measure urine sodium concentration Causes of Hypernatremia Volume Depletion Volume Expansion Urine Na+ < 20: sweating, diarrhea, burns Urine Na+ > 20: Renal losses: Hyperglycemia, mannitol, urea (osmotic diuresis), or intrinsic renal disease Urine Na+ > 20: Salt loading, Cushing’s syndrome, NaHCO3, hypertonic dialysis Eulovemic Urine Na+ < 20: Fever, heat exhaustion, hypermetabolic state Urine Na+ variable or > 20: Central DI, Nephrogenic DI Diuretic Drugs Alcohol Diphenylhydantoin Lithium Demeclocycline Acetohexamde Tolazamide Glyburide Propoxyphene Amphotericin Methoxyflurane Norepinephrine Patient Groups at Increased Risk for Hypernatremia Post craniotomy (sellar tumors) Elderly, nursing home residents Hypertonic infusions Tube feedings Osmotic diuretics Lactulose Mechanical ventilation Diabetes mellitus with poor glycemic control Polyuric disorders Diabetes Insipidus Central DI Failure to synthesize or secrete ADH Unable to concentrate urine with water deprivation (caution !) – 3% decrease in BW or increase in Posm to 295 normally results in increase in Uosm > 700 – Submaximal response: give ADH Central DI Uosm will increase by 100% or more Therapeutic Regimens for the Treatment of Diabetes Insipidus Drug Complete central dDAVP diabetes insipidus Partial central Vasopressin diabetes insipidus tannate Aqueous vasopressin Chlorpropamide Clofibrate Carbamazepine Nephrogenic Thiazide diabetes insipidus diuretics (NDI) NSAIDS Dose 10-20 mg intranasally q 12-24 hr 2-5 U IM q 24-48 hr 5-10 U SQ q 4-6 hr 250-500 mg/day 500 mg tid-qid 400-600 mg/day Conventional doses Conventional doses Amiloride (for 5 mg qd lithium-related NDI) Nephrogenic Diabetes Insipidus Does not respond to AVP Causes: Congenital NDI - AVPR2 or AQP2 mutation Hypokalemia Hypercalcemia Drugs: Lithium, demeclocycline, glyburide, colchicine, amphotericin B Treatment: Thiazides Reduce solute intake (low Na+ diet) NSAIDS Treatment of Symptomatic Hypernatremia 1. Drop Na+S by 2 mEq/L/hr. 2. Replace 50% of water deficit over 12-24 hrs. 3. Replace rest over next 24 hrs. 4. Perform serial neurological exams. 5. Decrease rate of correction when patient improved. 6. Measure Na+ in serum and urine q 12 hrs.