Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
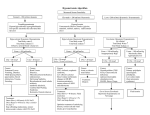
Syndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH) Pathophysiology Abnormal production & secretion of antidiuretic hormone (ADH) vasopressin Vasopressin normally released from posterior pituitary → acts on collecting ducts → causes kidneys to reabsorb water Water retention results in hyponatremia & water intoxication Incidence & At Risk Populations Occurs in 3-5% of adults with cancer Causes: Ectopic tumor secretion of ADH or ADH-like substances Small cell lung cancer (accounts for 80% SIADH in cancer) Head & neck cancer Pancreatic, prostate, duodenal, or colon carcinoma Hodgkin’s & nonHodgkin’s lymphoma Thymoma Primary brain tumors Chemotherapy Cisplatin Cyclophosphamide Ifosphamide Melphalan (high dose) Vinca alkaloids Other Medications Narcotics Tranquilizers Barbiturates General anesthetics Non-Malignant Causes CNS Disorders Pulmonary Disorders Signs & Symptoms Severity of symptoms depends on how quickly the syndrome develops and the degree of hyponatremia Mild hyponatremia: Sodium 125 – 134 mEq/L May be asymptomatic May present with thirst, anorexia, nausea, fatigue, weakness, muscle cramps, headache Moderate hyponatremia: Sodium 115 – 124 mEq/L Weight gain, oliguria, progressive neurologic symptoms Severe hyponatremia: Sodium < 115 mEq/L Signs/symptoms related to cerebral edema Papilledema, delirium, hypoactive reflexes, ataxia, gait disturbances, seizures, coma, death Other common symptoms: Weight gain without edema Thirst ↓ Urine Output Medical Management Treat underlying cause Fluid restriction Mild hyponatremia: 800-1,000 ml/day Moderate to severe hyponatremia: 500 ml/day IV fluid administration Mild to moderate hyponatremia: isotonic (0.9%) saline Severe hyponatremia: hypertonic (3%) saline may be infused at rate of 1-2 mEq/L per hour Discontinue when serum sodium level >120 mEq/L Avoid rapid correction of hyponatremia → too rapid correction may lead to demyelination of nerve tissue 20 rapid loss of brain electrolytes & organic osmolytes Pharmacologic interventions: Administer medications that block the action of ADH in the collecting tubules Demeclocycline: 600 – 1200 mg po daily Urea 30-60 mg po daily Lithium carbonate Nursing Management Assess hydration status Skin turgor Mucus membranes Intake & output Daily weights Assess neurologic status Changes in LOC Headache Lethargy Irritability Disorientation, mental confusion Seizures Maintain safety needs Seizure precautions for serum sodium < 125 mEg/L Keep area free of clutter Patient & Family Education Report signs & symptoms of hyponatremia including thirst, weight gain without edema, ↓ urine output, nausea, anorexia, weakness, headache, confusion, irritability Rationale for fluid restrictions & plan for fluid intake Comfort measures to ↓ dry mouth (oral care, sugarless candy) From: Clancey, J.K. (2006). “Syndrome of Inappropriate Antidiuretic Hormone Secretion”, in Understanding and Managing Oncologic Emergencies: A Resource for Nurses, Kaplan, M. (Ed.). Pittsburgh: Oncology Nursing Society, pp. 197-216.