Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
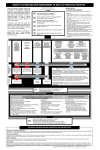
Case Report Extravasation Injury of the Upper Limb by Intravenous Clindamycin Dahal P,* Shrestha JM** *Consultant surgeon, Associate Proffesor, TUTH ABSTRACT Intravenous drug administration is a common practice in all hospitals. It can cause minor complications like thrombophlebitis to severe complications like local skin necrosis, and severe soft tissue necrosis. It can also cause severe disability. Attention and caution is necessary in the intravenous administration of irritant drugs. INTRODUCTION I ntravenous fluids and drugs administration is a routine procedure for nurses. Extravasation or infiltration occurs when fluids or medications administered by the intravenous route penetrates the perivascular or subcutaneous space. All intravenous fluids can cause tissue injury following extravasation. However, certain substances such as cytotoxic or vasoactive drugs and hyperosmolar agents are associated with a greater risk of tissue injury. The complications may range from minor (ecchymosis, hematoma and phlebitis) to severe form (extravasation causing tissue necrosis). The reported incidence of complications of extravasation is very difficult to obtain in the literatures. Some studies have reported the extravasation of vesicant chemotherapy in children by 11% and in adults by 22%.1But there are different case reports on extravasation of different cytotoxic agents in the literatures but no literature was found about the tissue injury due to extravasation of intravenous clindamycin. Extravasation induces prolonged hospital stay of patient, unnecessary diagnostic procedures, treatment, disability and stress in the life of the patients andto their relatives. The economic loss and medico legal complications areanother important Correspondence : Dr Peeyush Dahal Burn& Plastic Surgery Unit National Academy of Medical Sciences Bir Hospital, Kathmandu Email: [email protected] factor.In this article, a patient with extravasation of intravenous Clindamycin is described with literature review. CASE REPORT A 14 years boy was admitted to the hospital for the treatment of empyema thoracic with sepsis. He had the history of seizure disorders in the past and he was regularly taking phenytoin orally. At the time of hospital admission peripheral intravenous line was open and intravenous Clindamycin(Dalacin) and Amikacin was administered. He developed painful swelling in the right forearm immediately after administration of drug. When the swelling and pain increased this intravenous line was removed. Central venous pressure line was placed, thoracotomy was done but the swelling of forearm increased gradually and extended up to the lower part of arm. The skin became black(Figure: 1) on the seventh day.Then hewas referred to plastic surgery unit with wrist drop on the 15th day after thoracotomy. Figure 1. The wound was debrided immediately. Common extensor muscles were necrosed at their proximal part and were necrosed partially at the distal part. Upper Volume 11│Number 2│Jul-Dec 2011 51 PMJN Postgraduate Medical Journal of NAMS Extravasation Injury of the Upper Limb by Intravenous Clindamycin part of theradius was exposed and the elbow joint space was opened (figure: 2). Figure 2. The raw area was covered with thick split thickness skin graft and the bone was covered with fasciocutaneous abdominal flap(Figure 3&4). Figure 3. Figure 4. Flap was detached after four weeks (Figure 5) and he was discharged by planning for tendontransfer to correct the wrist drop. Figure 5. 52 PMJN Postgraduate Medical Journal of NAMS Volume 11│Number 2│Jul-Dec 2011 DISCUSSION Extravasation is defined either as the escape of a chemotherapeutic agent from a vessel into the surrounding tissues by leakage or as an involuntary injection of a drug into the tissues2. The chemotherapeutic agents may be vesicants or the irritants and extreme ph causes decrease vein tolerance and rupture leading to extravasation. Author could not find a single literature regarding extravasation of intravenous clindamycin. Irritants are drugs that can cause an inflammatory reaction, aching, swelling, pain or phlebitis at the injection site or along the vein. Generally symptoms are self-limiting and usually there are no long-term sequelae. But Symptoms may arise immediately orseveral days or weeks after extravasation of vesicant drugs. The severity of tissue injury is dependent on the type, concentration and quantities of the injected chemotherapeutic agent. It may cause severe and lasting tissue injury and necrosis and sometimes leading to disability. Review of the literature has revealed case reports of devastating tissue injuries(skin with or without muscle necrosis following cysplatin3, Mitomycin4 phenytoin5 extravasation. It is also found that the antibiotic, diuretics, dextrose extravasation has induced severe tissue injuries requiring reconstructive surgery.6 There different modalities of the treatment of the acute stage of this complication which include general measures like elevation of the involved extremity and application of coldcompresses to minimize the inflammatory reactions7, 8. The use hyaluronidase, phentolamineinjections and glyceryl trinitrate patches topromote drug absorption are also found9, 10, 11, 12. Saline flush-outhas been used to dilute the drug. Some authorsadvocate specific antidotes as the mainstay of treatment8.Early surgical debridement and skin grafting have also beenrecommended13. The systemic approach with some guide lines help for prompt and effective management. For this purpose Millam’s Classification (Table no.1)6 would be useful. Millam proposed conservative treatment for Stages I and II, and intervention for Stages III and IV. Stages III and IV infiltrates require prompt and aggressive intervention. Some exit stab incisions under local or general anesthesiaare made around the periphery Extravasation Injury of the Upper Limb by Intravenous Clindamycin of the area of extravasation and saline isinjected for flushing.Hyaluronidase, glyceryltrinitrate are other agents to reduce the ongoing tissue injury. There are specific antidotes for specific agents like anthracyclines, mitomycin C and mustine14. Table 1. Staging of intravenous (IV) infiltrates Stage Features I Painful IV site No erythema No swelling II Painful IV site Slight swelling (0%–20%) No blanching Good pulse below infiltration site Brisk capillary refill below infiltration site III Painful IV site Marked swelling (30%-50%) Blanching Skin cool to touch Good pulse below infiltration site Brisk capillary refill below infiltration site IV Painful IV site Very marked swelling (75%) Blanching Skin cool to touch Decreased or absent pulse* Capillary refill > four seconds* Skin breakdown or necrosis * The presence of any one of these characteristics constitutes a Stage IV infiltrate. CONCLUSION Intravenous extravasations of clindamycin may cause devastating complication as other chemotherapeutic agents. Safe Medication practices, precaution, awareness and intravenous drug administration guideline should be established to minimize extravasations. Prompt recognition and intervention also reduce the incidence of tissue necrosis leading to disability. REFERENCES 1. L. Hadaway, Infiltration and extravasation, preventing a complication of IV catheterization. AJN, 2007, 107 (8): 64-72, 2. D. L.Schrijvers Extravasation: a dreaded complication of chemotherapy. Annals of Oncology 14 (Supplement 3): 26–30, 2003. 3. O. Bairey, M. Shakali, J. Bashara. Severe tissue necrosis after Cysplatin Extravavasation at Low Concerntration: possible “Immediate Recall Phenomenon”.J Natl Cancer Inst 1997, 89 (16): 1233-1234. 4. E. U. Avdal, N. Aydinoğlu. Extravasations of Vesicant / Non- Vesicant Drugs andEvidence – Based Management: Int J Caring Sciences 2012, 5(2): 192-202. 5. J. J. Edwards, V Bosek. Extravasation Injury of the Upper Extremity by intravenous phenytoinAnesthAnalg 2002, 94; 672-3. 6. REC Rose, R Felix, A Crawford-Sykes, R Venugopal, G Wharfe, G Arscott; Extravasation Injuries; West Indian Med J 2008; 57 (1): 40-47 7. DLLarson. What is the appropriate management of tissue extravasationby antitumor agents? Plast Reconstr Surg 1985; 75: 397–405. 8. D. Casanova, J Bardot, GMagalon. Emergency treatment of accidentalinfusion leakage in the newborn: report of 14 cases. Br J Plast Surg2001; 54: 396–9 9. DCasanova, J Bardot, G Magalon. Emergency treatment of accidentalinfusion leakage in the newborn: report of 14 cases. Br J Plast Surg2001; 54: 396–9. 10.R.G. Dufresne. Skin necrosis from intravenously infused materials.Cutis 1987; 39: 197–8 11.L. Flemmer, JSL Chan. A pediatric protocol for management of extravasation injuries. Pediatr Nrusing 1993; 19: 355–8, 424. 12. 24. O’Reilly C, McKay FMA, Duffy P, Lloyd DJ. Glyceryl trinitrate in skinnecrosis caused by extravasation of parenteral nutrition. Lancet 1988;2: 565–6. 13. Linder RM, Upton J, Osteen R. Management of extensive doxorubicinhydrochloride extravasation injuries. J Hand Surg 1983; 8: 32–8. 14.Bertelli G. Prevention, management of extravasation of cytotoxicdrugs. Drug Saf 1995; 12: 245–55. Volume 11│Number 2│Jul-Dec 2011 53 PMJN Postgraduate Medical Journal of NAMS