Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
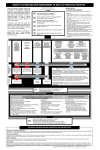
WOMEN AND NEWBORN HEALTH SERVICE King Edward Memorial Hospital CLINICAL GUIDELINES OBSTETRICS & GYNAECOLOGY PARENTERAL THERAPY IRON THERAPY MANAGEMENT OF INFILTRATION / EXTRAVASATION OF INTRAVENOUS IRON THERAPY Keywords: Iron infusion, extravasation, infiltration, iron therapy, ward 4 infusion unit AIM To describe the appropriate management of a woman who has sustained infiltration / extravasation of intravenous (IV) iron therapy. PROCEDURE BACKGROUND Paravenous leakage of all forms of IV iron therapy results in permanent skin pigmentation and may cause skin irritation thus it is imperative that the infusion is stopped immediately if infiltration/extravasation is suspected. Volumetric pumps will initially continue to flow until fluid accumulates in the subcutaneous tissues, thus careful observation and monitoring of the cannula insertion site is imperative. Recognition of infiltration/extravasation Table 1: Signs and symptoms of infiltration and extravasation Infiltration Tenderness/discomfort at insertion site Extravasation As infiltration in addition: Swelling above or below insertion site Burning stinging pain Taut skin above or below insertion site Redness may occur followed by blistering, tissue necrosis and ulceration Fluid leak at insertion site Coolness/blanching around insertion site Numbness or tingling above or below insertion site MANAGEMENT OF THE INFILTRATION 1. Remove the cannula immediately and abandon the infusion. 2. Do not attempt to resite the infusion. 3. Reassure and provide a full explanation to the patient. 4. Assess and document the volume of infiltration by recording the volume of the infused fluid. 5. Inform the patients RMO so an assessment can be made of sensory deficit which could indicate nerve damage or compartment syndrome. 6. Further advice may be required from other specialities including Dermatology (skin staining), Plastic Surgery (sensory deficit) or Haematology (anaemia management) as per individual patient symptoms. 7. Apply a cold pack to the infiltrated site and elevate the affected limb. 8. If iron staining is immediately visible, measure the site and arrange for hospital photographs to be taken. This will aid ongoing monitoring of the patient 9. Clearly document the management in the patient’s medical records. 10. Complete a clinical incident form. 11. The patient will be followed up as an out-patient where long term management will be discussed. 12. Laser therapy has been successful in reducing the skin staining long term. 2014 All guidelines should be read in conjunction with the Disclaimer at the beginning of this section Page 1 of 2 MANAGEMENT OF EXTRAVASATION If redness or blistering is apparent, then tissue necrosis can occur and management is aimed at limiting further tissue damage. 1. Remove the cannula immediately and abandon the infusion. 2. Do not attempt to resite the infusion. 3. Reassure and provide a full explanation to the patient. 4. Assess and document the volume of infiltration by recording the volume of the infused fluid. 5. Inform the patients RMO so an assessment can be made of sensory deficit which could indicate nerve damage or compartment syndrome. 6. Hydrocortisone cream may relive the irritation. 7. Further advice may be required from other specialities including Dermatology (skin staining), Plastic Surgery (ulceration or sensory deficit) or Haematology (anaemia management) as per individual patient symptoms. 8. Apply a cold pack to the infiltrated site and elevate the affected limb. 9. If redness, blistering or iron staining is immediately visible, measure the site and arrange for hospital photographs to be taken. This will aid ongoing monitoring of the patient 10. Clearly document the management in the patient’s medical records. 11. Complete a clinical incident form. 12. The patient will be followed up as an out-patient where long term management will be discussed. 13. Laser therapy has been successful in reducing the skin staining long term. REFERENCES / STANDARDS Doellman D, Hadaway L, Bowe-Geddes LA et.al. (2009) Infiltration and extravasation. Update on prevention and management. Journal Infusion Nursing 32;4. 203 – 211. Dougherty L (2008) IV therapy: recognising the differences between infiltration and extravasation British Journal of Nursing 17;14. 896 – 901. Erner RA, Meganlathery SB and Styler M (2004) Extravasation of systematic hemato-oncological therapies. Annals of Oncology 15 (6) 858 – 862 Raulin C, Werner S and Greve B. (2001) Circumscripted pigmentations after iron injections- treatment with Q switched laser systems. Lasers in Surgery and Medicine 28. 456 – 460. National Standards – 1- Care Provided by the Clinical Workforce is Guided by Current Best Practice 1- Incident Management and Reporting 9- Recognising and Responding to Clinical Deterioration 7- Blood and Blood products treatment options Legislation - Nil Related Policies – KEMH Clinical Guidelines: O&G: Parenteral Therapy: Iron Therapy Other related documents – Nil RESPONSIBILITY Policy Sponsor Initial Endorsement Last Reviewed Last Amended Review date Nursing & Midwifery Director OGCCU August 2014 August 2017 Do not keep printed versions of guidelines as currency of information cannot be guaranteed. Access the current version from the WNHS website. Management of Infiltration / Extravasation of Intravenous Iron Therapy Clinical Guidelines: Obstetrics & Gynaecology 2014 King Edward Memorial Hospital for Women Perth, Western Australia All guidelines should be read in conjunction with the Disclaimer at the beginning of this section Page 2 of 2