Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
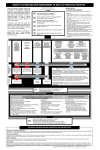
Extravasation of Intravenous Non-Chemotherapeutic Agents Lisa Sheehan, RN, BSN UPMC Shadyside What is Extravasation? Extravasation happens when a vesicant medication escapes into the surrounding tissue by: Cannula puncturing the Fluid leaking from vein at wall of the vein insertion site Signs / Symptoms: pain, redness, burning, pallor, no blood return, edema, decreased IV flow or flush Who is at an increased risk for extravasation? • Patients with chronic conditions causing arterial insufficiency • Patients with compromised venous or lymph drainage • Patients on meds that can cause the skin and veins to become more fragile: corticosteroids, anticoagulants, chemotherapy • Elderly, children, and sedated patients Prevention, Prevention, Prevention… Early detection and prompt action are required to prevent tissue necrosis and functional loss in this medical emergency First step after extravasation is noticed or suspected… STOP THE INFUSION STOP Calcium Chloride extravasation that resulted in hand amputation Post-Extravasation Steps… • Leave catheter in place without any pressure to the site and explain procedure to patient • Estimate amount of medication that entered surrounding tissue • Perform hand hygiene • Aspirate medication with 3ml syringe directly attached to the colored hub and withdraw catheter while aspirating Post-Extravasation Steps… • Clean area with alcohol and let dry • Trace leading edge of extravasated area and / or photograph to monitor improvement or worsening of area (This step is often missed) • Elevate extremity above level of heart for 48 hours to help reduce edema • DO NOT use this site, sites distal to, or entire extremity if possible for IV access until resolved • Re-establish IV access Consider MD consultation • Severe extravasation symptoms exist • • • • Severe pain Skin discolored around area Inflammation larger than a quarter Drugs used include amiodarone, epinephrine, norepinephrine, phenylephrine, dopamine, ephedrine, vasopressin, calcium chloride, or vancomycin When to Consult Plastic Surgery • Extravasation involves calcium chloride • Surrounding tissues are discolored, tense, blistering • Patient reports severe pain • Decreased peripheral pulse or slow cap refill • Greater than 25ml medication escaped into tissue Compresses Warm Compress • Promote vasodilation • Increased drug absorption • Decreased local drug concentration • Can cause maceration and necrosis if MOIST HEAT used Cold Compress • Promote vasoconstriction • Localizes the extravasation • Allows vasculature and lymph system to drain the medication from the area Procedure: Apply compress for 5 minutes then check site. If red, macerated, blistering, or patient feels pain with compress remove compress!! Apply for 15-20 minutes at least 4 times / day for 24 hours or until discomfort resolved. Antidotes • All antidotes must be ordered by MD or advanced practice provider • MD must assess patient prior to giving antidote • Use for severe extravasations where patients are showing severe symptoms or severe pain • Time is of the essence to be effective! Phentolamine • Primarily used for Pressor extravasation • Should be used within 12 hours of incident • May use more than one dose if needed to encircle affected area • Max dose 50 mg During drug shortages nitroglycerin topical ointment or transdermal patch may be used if patient is stable with SBP > 90. Hyaluronidase • Primarily for non-pressor extravasations • Most effective if used within 60 minutes of incident, but can be beneficial up to 12 hours after the incident. Antidote Administration • Multiple subcutaneous injections are given using a 25g or 26g needle in a pin-cushion fashion along the periphery of the affected site. • Change the needle with each new injection Assessment To be performed and charted each shift or patient handoff until any symptoms are resolved or patient is discharged Affected Area Affected Extremity • Redness / necrosis • Edema • Drainage • Pain, burning, itching • Changes in temperature of area • Sensation of fingertips / toes • Movement • Pulses Documentation • Complete an incident report • Document severity according to Infiltration Rating Scale • Include: • • • • • • • • Measurements, location, catheter size Subjective description Estimated fluid volume of medication MD notification Management of extravasation provided Photograph if taken Patient education and follow-up instructions Consults if needed INS Infiltration and Extravasation Scale Case Study #1 • Radiology called IV Team for restart of an IV but the patient was in transit. IV Team advised them to have floor call when patient settled. • 30 minutes later, floor RN calls with infiltrate of Potassium and possibly Zosyn into a swollen hand / wrist area • IV RN arrives within 15 minutes to find IV removed and patient reporting, “This is the worst pain I have ever felt in my life.” • IV Team suggested antidote Hyaluronidase was needed, so call MD. • IV Team notes swelling approximately to mid forearm, cool to touch and leaking from IV site and advises plastic surgery consult if antidote does not relieve pain. All pulses WNL Case Study #1 cont’d… • MD arrives and unsure of what to order or how to treat. • IV RN suggests antidote and hands hospital policy to RN for MD reference. IV RN had to leave unit for urgent blood restart. • IV Team arrives back to unit to find antidote was never given and the plastic surgeon was angry at being told he needed to be there within 60 minutes to address this situation. • Patient arm was elevated with cool compress. • Plastics did see patient and advised current treatment and that antidote no longer needed by the time he arrived (2-3 hours after call) and no risk for necrosis was evident. Case Study #1 Questions • What could have been done better? • What was done well? • How could it have been prevented? Case Study #2 • IV Team called to ICU for extravasation of epinephrine from a chest port. IV Team arrived within 10 minutes. • Advised immediate MD consult to order antidote. • MD arrived within 10 minutes and ordered antidote. ICU RN administered antidote with IV Team as a resource. • Plastics consulted with treatments advised for tissue sloughing, but no surgical intervention needed. Case Study #2 Questions • What could have been done better? • What was done well? • How could it have been prevented?