Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
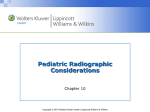
Medication Administration and Intravenous Therapy Copyright © 2008 Wolters Kluwer Health | Lippincott Williams & Wilkins The Six “Rights” of Medication Administration • The right medication • The right patient • The right dose • The right route • The right time • The right documentation Copyright © 2008 Wolters Kluwer Health | Lippincott Williams & Wilkins Role of the Nurse in Medication Administration • Understanding the factors that influence or alter how the child absorbs, metabolizes, and excretes the medication • Being aware of any allergies the child may have • Administering the medications properly • Teaching the patient and the family caregivers about the effects and possible side effects of medications given Copyright © 2008 Wolters Kluwer Health | Lippincott Williams & Wilkins Copyright © 2008 Wolters Kluwer Health | Lippincott Williams & Wilkins Guidelines for Medication Administration in Children • Do not give the child a choice in whether or not to take the medicine • Do give choices that allow the child some control • Do not tell the child that the injection will not hurt • Give simple and brief explanations • Assure child that it is okay to be afraid and/or to cry • Do not talk in front of the child as if he or she were not there • Be positive in approaching the child Copyright © 2008 Wolters Kluwer Health | Lippincott Williams & Wilkins Guidelines for Medication Administration in Children (cont.) • Keep time between explanation and administration brief • Prepare for medication administration out of sight of the child • Obtain cooperation from family caregivers Copyright © 2008 Wolters Kluwer Health | Lippincott Williams & Wilkins Methods of Computing Child Dosages for Medication • Body weight method – The child’s weight in kilograms is used to calculate a safe dose range for that child • Body surface area (BSA) method – The West nomogram • A graph with several scales arranged • When two values are known, the third can be plotted by drawing a line with a straight edge Copyright © 2008 Wolters Kluwer Health | Lippincott Williams & Wilkins Using a Nomogram Used to estimate the body surface area (BSA) of a child height is on the left, weight is on the right The BSA is the area where a ruled line intersects on the middle column Used to calculate child’s dose from an adult dosage of medication (average adult BSA = 1.7 m2). (example 12 kg/58 in.=.66 m2) Copyright © 2008 Wolters Kluwer Health | Lippincott Williams & Wilkins Routes of Medication Administration • Oral • Intramuscular • Eye, ear, and nose drops • Rectal medications • Intravenous therapy Copyright © 2008 Wolters Kluwer Health | Lippincott Williams & Wilkins Oral Medications • Sit infant on your lap using the “hugging” method (infant’s legs between your knees and one arm tucked behind your back) • Mix suspensions well • If using syringe, place to the side and back of mouth • Give slowly via cup or syringe, allowing time for swallowing, do not put in baby’s bottle • Older child may be able to do themselves • May offer juice or water after administration Copyright © 2008 Wolters Kluwer Health | Lippincott Williams & Wilkins Copyright © 2008 Wolters Kluwer Health | Lippincott Williams & Wilkins Copyright © 2008 Wolters Kluwer Health | Lippincott Williams & Wilkins Ear Drops • To straighten ear canal: • Children under the age of 3, pull pinna of ear down and back • Children older than 3, pull pinna up and back • Gently massage area in front of ear to facilitate entry of drops • Keep supine for a few minutes to facilitate fluid absorption • Allow to warm prior to installation Copyright © 2008 Wolters Kluwer Health | Lippincott Williams & Wilkins Suppository/Enema • Guideline for enema administration: • infant - 120 to 240 mL, insert 1 inch • 2 to 4 years - 240 to 360 mL, insert 2 inches • 4 to 10 years - 360 to 480 mL, insert 3 inches • 11 years - 480 to 720 mL, insert 4 inches • After rectal administration, hold the buttocks together firmly to relieve pressure on anal sphincter (5-10 min.) Copyright © 2008 Wolters Kluwer Health | Lippincott Williams & Wilkins IM Injections • Preferred sites: • vastus lateralis/rectus femoris - thigh muscles, site free of major nerves and blood vessels, preferred site for infants • ventrogluteal - only use after walking for 1 year • dorsogluteal - high risk (sciatic nerve and major blood vessel), poorly developed in infants - DO NOT USE • deltiod - upper arm, site for rapid absorption, Copyright © 2008 Wolters Kluwer Health | Lippincott Williams & Wilkins Injections • Subcutaneous: 3/4-5/8 inch, 23-26 gauge, upper arm or abdomen • IM: 5/8-1 inch, 20-25 gauge, vastus lateralis, deltoid • IM maximum amounts: 0.5 mL for infants, 1 mL for toddlers, in school-age/adolescent deltoid 1 mL, vastus lateralis 2 mL • EMLA cream (topical anesthetic) can be used if time allows (60 min. to 2 1/2 hours) • Pediatric doses are calculated to the nearest hundreth and usually measure in a TB syringe Copyright © 2008 Wolters Kluwer Health | Lippincott Williams & Wilkins Copyright © 2008 Wolters Kluwer Health | Lippincott Williams & Wilkins Reasons for Administering IV Therapy to a Pediatric Patient • To maintain fluid and electrolyte balance • To administer antibiotic therapy • To provide nutritional support • To administer chemotherapy or anticancer drugs • To administer pain medication • To administer blood products Copyright © 2008 Wolters Kluwer Health | Lippincott Williams & Wilkins Candidates for IV Therapy • Children who have poor gastrointestinal absorption caused by diarrhea, vomiting, and dehydration • Children who need a high serum concentration of a drug • Children who have resistant infections that require IV medications • Children with emergency problems • Children who need continuous pain relief Copyright © 2008 Wolters Kluwer Health | Lippincott Williams & Wilkins Fundamental Concepts of Fluid Balance • Water – Intracellular fluid – Extracellular fluid • Electrolytes – Maintain acid–base balance • Acid–base balance – Acidosis – Alkalosis Copyright © 2008 Wolters Kluwer Health | Lippincott Williams & Wilkins Copyright © 2008 Wolters Kluwer Health | Lippincott Williams & Wilkins Complications Associated With the Use of Central Venous Lines • Contamination • Thrombosis • Dislodgement of the catheter • Extravasation (fluid escaping into surrounding tissue) Copyright © 2008 Wolters Kluwer Health | Lippincott Williams & Wilkins Selection of IV Sites • Varies with the child’s age • The best choice is the one that least restricts the child’s movements • Sites used include the hand, the wrist, the forearm, the foot, and the ankle • The antecubital fossa, which restricts movement, is sometimes used, only if other sites are not available • The scalp vein may be used if no other site can be accessed Copyright © 2008 Wolters Kluwer Health | Lippincott Williams & Wilkins Equipment Collected in Preparation for Starting an IV Line • IV tubing • Any necessary extension tubing • The container of solution • The equipment to stabilize the site • A tourniquet • Cleansing supplies used by the institution Copyright © 2008 Wolters Kluwer Health | Lippincott Williams & Wilkins Equipment Collected in Preparation for Starting an IV Line (cont.) • Sterile gauze, adhesive tape, cling roll gauze • An IV pole • An infusion pump or controller • A plastic cannula or winged small-vein needle, usually between 21-gauge and 25-gauge (depending on the child’s size) Copyright © 2008 Wolters Kluwer Health | Lippincott Williams & Wilkins Observations of the IV Site • Redness • Pain • Induration (hardness) • Flow rate • Moisture at the site • Swelling Copyright © 2008 Wolters Kluwer Health | Lippincott Williams & Wilkins