Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
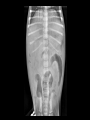
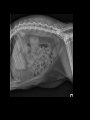
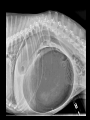
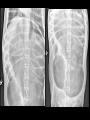
Emergency Radiographs Emergency Radiographs Immediate action needs to be taken If the condition is life threatening, treatment should be immediately started based on clinical signs/physical examination without waiting for radiographic confirmation Tension pneumothorax Radiographs can be stressful to already compromised patients Congestive heart failure Case 1 • 9 month old MN Jack Russell Terrier • Vomiting and gagging Esophageal Foreign Body Esophageal Foreign Body • Most common locations Caudal esophagus Thoracic inlet Heart base Esophageal Foreign Body Radiographic Signs • Visualization of a FB in the region of the esophagus • Deviation of the hilus or trachea Esophageal Foreign Body Radiographic signs – If complete obstruction, may see dilation of the esophagus cranial to the FB. – Aspiration pneumonia!!! – +/- pneumomediastinum Esophageal Foreign Body Positive Contrast • Only if the foreign body is not definitively identified – Filling defect Esophageal Foreign Body Positive Contrast • Barium sulfate – Avoid with esophageal foreign bodies • Pyogranulomatous reaction within the mediastinum if esophageal tear • Can make endoscopy difficult Esophageal Foreign Body Positive Contrast • Barium sulfate – Aspiration can cause pneumonitis and granulomas of interstitial tissues and lymph nodes • Likely volume dependent • Small amount of aspiration likely negligible Esophageal Foreign Body Positive Contrast • Iodinated contrast – Prefer over barium sulfate – Adverse reactions not reported with leakage into the mediastinum – Can cause pulmonary edema if aspirated • Volume dependent • May be more severe with ionic compared to non-ionic Esophageal Foreign Body • If there is a clinical concern for an esophageal FB, make sure to also radiograph the cervical esophagus Esophageal Foreign Body • Patient had endoscopy and the foreign body was pushed into the stomach • Followed with surgery/gastrotomy Case 2 • 5 yr old FS Chihuahua • Vomiting Small intestinal mechanical obstruction Small intestinal mechanical obstruction Radiographic signs • Distention of small intestines orad to the obstruction – Two populations/diameters of bowel Small intestinal mechanical obstruction Radiographic signs • Ratio small intestinal diameter to height of L5 vertebral body – SI/L5 ratio of 1.95 = 77% probability of obstruction – SI/L5 ratio of 2.07 = 86% chance of obstruction • However, the SI/L5 ratio was not associated with increased accuracy for observers, regardless of level of experience Ciasca TC. Does measurement of small intestinal diameter increase diagnostic accuracy of radiography in dogs with suspected intestinal obstruction? Veterinary Radiology and Ultrasound 2013;54:207-211. Small intestinal mechanical obstruction Radiographic signs • Ratio of small intestinal diameter to height of L5 vertebral body 0.4 cm 0.4 cm 1.1 cm 1.1 cm 1.1/0.4 = 2.75 Small intestinal mechanical obstruction Radiographic signs • Make sure to measure from serosal to serosal margin, not just the gas filled lumen Incorrect! Correct! Small intestinal mechanical obstruction Radiographic signs • Decreased serosal detail within the abdomen – Effusion and/or peritonitis Small intestinal mechanical obstruction Radiographic signs • The more distal the obstruction, the greater number of distended segments Small intestinal mechanical obstruction Radiographic signs • With progressive distension, the distended segments can have a stacked appearance Small intestinal mechanical obstruction Radiographic signs • Partial obstructions can be difficult – Can see a gravel sign with a chronic partial obstruction – Fluid can pass through however larger pieces cannot and become dessicated Thrall Textbook of Veterinary Radiology; sixth edition Small intestinal mechanical obstruction Radiographic signs • Pneumoperitoneum if ruptured – Make sure to include the cranial abdomen – Commonly accumulates between liver and diaphragm Small intestinal mechanical obstruction • Right AND left lateral projections – Redistributes gas and fluid in the stomach and intestines Left lateral Right lateral Small intestinal mechanical obstruction • Not always due to foreign body – Intestinal masses (especially in older patients without history of foreign body ingestion) • Ultrasound may be helpful if presence of a mass will preclude surgery – Intussusception, adhesions, extraluminal masses Functional ileus • Functional ileus results in decreased motility due to a neurologic or muscular dysfunction • Distention of small intestine (usually not as severe as an obstruction) • Can be seen with enteritis (HGE and parvo), dysautonomia, certain drugs • Usually generalized dilation of bowel in contrast to two populations of bowel • A distal small intestinal mechanical obstruction can mimic • Clinical signs/signalment Case 3 • 9 wk old MI Golden Retriever • Vomiting for 2 days and diarrhea for 2 weeks • Lethargic Findings • A few intestinal segments are gas distended • Not all are in the plane of the colon Pneumocolon Pneumocolon Intussusception Intussusception • One intestinal segment (intussesceptum) telescopes/invaginates into the lumen of the adjacent segment (intussuscipiens). – Difference in motility between adjacent segments – Ileocolic or cecocolic junction most common location Intussusception Radiographic signs • Intestinal distention depends on location and severity of obstruction • Obstruction may be transient • If causing a distal obstruction, can get diffuse small intestinal distention • Can sometimes see intussusception if there is enough surrounding gas • Can be a difficult diagnosis Intussusception • Ultrasound helpful! – Transverse view • Bull’s-eye, concentric rings like onion – Mesenteric fat can be pulled into lumen of intussuscipiens Intussusception • Ultrasound helpful! – Longitudinal view • Linear layers of intestinal wall Case 4 • 2 yr MN DSH • vomiting Linear foreign body Linear foreign body Radiographic Signs • Plication of small intestines – Proximal portion of the linear foreign body becomes stuck at a fixed location and rest extends into the small intestine – Most commonly pylorus in dogs and base of tongue in cats – Peristalsis of small intestines causes the bowel to ride up the foreign body Linear foreign body Radiographic Signs • Plication of small intestines Linear foreign body Radiographic Signs • Plication of small intestines Linear foreign body Radiographic Signs • Plication of small intestines – Fragmented gas pattern – Comma shaped/angular gas bubbles instead of normal round gas bubbles Linear foreign body Radiographic Signs • Plication of small intestines Linear foreign body Radiographic Signs • Typically DOES NOT cause small intestinal distention • Partial mechanical obstruction Linear foreign body • Can be a challenging diagnosis • Ultrasound can be helpful if radiographs are not definitive – Undulating mucosa surrounding a hyperechoic central line Case 5 • 6 yr old MN Labrador • Retching/gagging Gastric dilation and volvulus (GDV) Gastric dilation and volvulus • The stomach is freely movable around its point of attachment to the diaphragm • It is attached by the gastrophrenic ligament at the esophageal hiatus and by the gastrohepatic ligament which connects the lesser curvature and pylorus to the hilus of the liver. • The gastroduodenal and gastrosplenic ligaments do not limit rotation except for the influence of the splenic vessels. • The main features that prevent undue movement of the stomach are the other abdominal organs and the abdominal wall Gastric dilation and volvulus • The stomach usually rotates in a clockwise direction (viewing the patient from the caudal direction) http://drstephenbirchard.blogspot.com/2013/09/gastric-dilatationvolvulus-which-dogs_2.html Gastric dilation and volvulus • In a normal dog, the pylorus is within the right abdomen and fundus is within the left abdomen • With a GDV, the pylorus usually deviates craniodorsally and to the left of midline pylorus fundus Gastric dilation and volvulus • Right lateral most diagnostic • DV if patient is stable enough – Concurrent splenic torsion – Evaluate if pylorus is to the right or left of midline Gastric dilation and volvulus Radiographic signs • Large gas and fluid (more gas than fluid) distended stomach Gastric dilation and volvulus Radiographic signs • Location of the pylorus near or to the left of midline and dorsally • DV helpful if patient stable enough Gastric dilation and volvulus Radiographic signs • Soft tissue line across the distended stomach separating the gas containing sections of the stomach into compartments – Stomach fold projects into the lumen and is outline by gas – Runs approximately in craniocaudal direction Gastric dilation and volvulus Radiographic signs • +/- Splenomegaly – impaired circulation • • Variable location of the body of the spleen DV helpful Gastric dilation and volvulus Radiographic signs • Thin gastric wall • Gas sometimes seen in the wall (pneumatosis) – Theories include gastric wall necrosis, prior trocharization, gas under pressure forced into submucosa, increased mucosal permeability. – Radiographic evidence has low sensitivity for gastric necrosis (14.1%) but high specificity (92.7%). – Not reliable indicator for gastric resection during surgery. Fischetti AJ, Pneumatosis in canine gastric dilatation-volvulus syndrome. Veterinary Radiology and Ultrasound. 2004;45:205-209. Gastric dilation and volvulus Radiographic signs • Hypovolemia, with small caudal vena cava and cardiac silhouette Thrall Textbook of Veterinary Radiology; sixth edition Gastric dilation and volvulus Radiographic signs • Caudal esophageal distention – The rotation of the stomach twists the terminal esophagus, causing obstruction that prevents eructation and vomition of gastric contents. Case 6 • 12 yr old Akita • Painful abdomen Case 6 Case 6 Gastric dilation Gastric dilation • Acute gaseous distension of the stomach may be secondary to aerophagia or gastric atony/ileus – Pain, drugs, panting, etc. • Radiographic determination of the location of the pylorus is the key differentiating feature between dilation and volvulus. – Look for location of spleen • Typically not a surgical emergency, but evaluate clinical signs Gastric dilation • Gas filled – Aerophagia – Gastric atony • Gastritis • Medications (e.g. opioids) • Fluid filled – Gastric atony – Pyloric outflow obstruction • Heterogeneous gas and soft tissue – Gastric atony – Food bloat – Pyloric outflow obstruction (sometimes gravel sign) Case 7 • 12 yr old Rhodesian Ridgeback • Gagging/retching 360o gastric dilation and volvulus • RARE!!! • Similar to severe gastric dilation – Pylorus and fundus seem to be in appropriate location 360o gastric dilation and volvulus • Spleen not in normal location… • Poor clinical status of patient • DV helpful! Case 8 • 8 yr old Golden Retriever • Tachypnea Pneumothorax Pneumothorax • Due to air accumulation within the pleural space • Due to air leaking from – penetrating wound - OPEN – Airways - CLOSED – Pneumomediastinum - CLOSED • A pneumomediastinum can cause a pneumothorax however a pneumothorax cannot cause a pneumomediastinum Pneumothorax • Air leaking from airways – Bulla/bleb – Rupture of a cavitary lung mass Pneumothorax Radiographic signs • Usually bilateral due to incomplete fenestration of the mediastinum in dogs and cats • However can be unilateral if the mediastinal fenestrations become closed due to pleural pathology (e.g. fibrin/adhesions) Pneumothorax • Unilateral pneumothorax Pneumothorax Radiographic signs • Retraction of lung from the body wall – Severity depends on amount of pleural gas/pressure • Caudal displacement of diaphragm depending on severity Pneumothorax Radiographic signs • Pulmonary markings/vessels do not extend to the body wall Pneumothorax Radiographic Signs • Do not be fooled by skin folds • Look for pulmonary markings/vessels over the fold • Margin of the fold extends beyond margins of thorax • No air between lung and diaphragm Pneumothorax Radiographic Signs • Do not be fooled by skin folds • Look for pulmonary markings/vessels over the fold • Margin of the fold extends beyond margins of thorax • No air between lung and diaphragm Pneumothorax Radiographic Signs • Separation of the cardiac silhouette from the sternum on lateral – Do not confuse with ventral mediastinal fat – Look for lack of pulmonary markings Pneumothorax Radiographic Signs • Separation of the cardiac silhouette from the sternum • Not really elevated • Heart is displaced laterally into the dependent thorax due to underinflation of the lung Thrall Textbook of Veterinary Radiology; sixth edition Pneumothorax Radiographic Signs • Increased opacity/unstructured interstitial pattern in lungs due to secondary atelectasis Case 9 • 5 yr old MN DMH • Severe tachypnea Tension Pneumothorax Tension pneumothorax • Pleural pressure exceeds atomspheric pressure during both phases of respiration – Check valve mechanism at the origin • Air enters during inspiration and does not escape during expiration • Pleural pressure rises, compromising ventilation and circulation • Requires IMMEDIATE thoracocentesis and ultimately chest tubes Tension pneumothorax • Treat the patient first based on physical examination findings – If air spontaneously fills the syringe during thoracocentesis, a tension pneumothorax is confirmed. Tension pneumothorax Radiographic Signs • SEVERE retraction of the lungs from the body wall • May be so severe that it does not resemble the shape of the lung Tension pneumothorax Radiographic Signs • Contralateral mediastinal shift if unilateral – In a regular pneumothorax the shift is toward the most collapsed side Tension pneumothorax Radiographic Signs • +/- caudal displacement of the diaphragm Case 10 • 10 yr old mixed breed dog • Difficulty breathing Left sided congestive heart failure Left Sided Congestive Heart Failure Radiographic signs • Perihilar and caudodorsal pulmonary edema – The high diastolic pressures in the left ventricle and/or left atrium “backs up” into the pulmonary veins and capillaries, causing transudation of fluid from the capillaries into the pulmonary interstitium and alveoli (pulmonary edema). • Can have a more patchy distribution in cats and some dogs Left Sided Congestive Heart Failure Radiographic signs • Pulmonary edema Left Sided Congestive Heart Failure Radiographic signs • Venous distention Enlarged cranial lobar veins Normal thorax Left Sided Congestive Heart Failure Radiographic signs • Increased height of the cardiac silhouette with dorsal displacement of the trachea – Left ventricular enlargement Left ventricular enlargement Normal thorax Left Sided Congestive Heart Failure Radiographic signs • Straightening of the caudal cardiac waist – Left atrial enlargement Left ventricular enlargement Normal thorax Left Sided Congestive Heart Failure Radiographic signs • Straightening of the caudal cardiac waist – Left atrial enlargement Left ventricular enlargement Normal thorax Left Sided Congestive Heart Failure Radiographic signs • Left atrial enlargement Left Sided Congestive Heart Failure Radiographic signs • +/- left auricular enlargement Left Sided Congestive Heart Failure • Cats can get pleural effusion with left sided congestive heart failure – Increased pulmonary vein pressure as a result of left heart failure can lead to the formation of pleural effusion because visceral pleural veins (the veins on the surface of the lung) also drain into the pulmonary veins in cats and dogs. • Pleural effusion does not happen in left sided heart failure with dogs. More concern for right sided heart failure. Left sided congestive heart failure vs bronchopneumonia • Bronchopneumonia typically has a ventral distribution of disease, not perihilar or caudodorsal Left sided congestive heart failure vs bronchopneumonia • Bronchopneumonia typically has a ventral distribution of disease, not perihilar or caudodorsal Left sided congestive heart failure vs bronchopneumonia • Evaluate size of the cardiac silouette and veins Left sided congestive heart failure vs bronchopneumonia • If in doubt, treat with lasix and look for response Case 11 • 3 yr old Chihuahua • 3 day history of ptyalism, decreased appetite, and abdominal pain Lung lobe torsion Lung lobe torsion • Lung lobe rotates along its long axis • Twisting of the bronchus and vessels at the level of the hilus • Depending on the severity of the torsion, the veins are compressed, impeding venous return – Less compressible arteries continue to supply blood venous congestion and sequestered blood in the lobe – Fluid and blood enter airways and also leak from the surface pleural effusion Lung lobe torsion – Can be difficult to diagnose with radiographs – CT may be more sensitive however patient may not have enough time • If the lobe is torsing intermittently, may not see it on CT – Suspicion increased in patients with an initial nonhemorrhagic effusion that has suddenly changed to a hemorrhagic effusion combined with a decline in clinical status Lung lobe torsion Typical radiographic signs • Alveolar pattern in affected lung lobe • Mass effect • Pleural effusion – Can mask the affected lung lobe – Repeat radiographs after thoracocentesis Lung lobe torsion Typical radiographic signs • Can progress into a vesicular pattern – Due to abscessation Lung lobe torsion Typical radiographic signs • Sometimes can see blunted termination of bronchus • Bronchus or vessels coursing in an abnormal direction • CT may allow visualization of torsed bronchus, however patient may need to go to surgery based on radiographic suspicion and clinical signs Lung lobe torsion • Differentials – Abscess • Causes – If effusion was present prior due to other disease, may predispose patient to developing a lung lobe torsion – effusion displaces lung lobes – Pugs predisposed? – Less common in cats? • Right middle lung lobe most affected, left cranial next common affected – Right middle lung lobe most mobile and has a long , narrow shape • Swelling of lung lobe and rapid adhesion formation do not permit the lung to reposition itself Questions???