Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
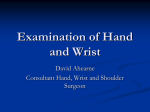
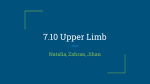
INJURY EVALUATION AND MANAGEMENT Recognition and Management of Triangular Fibrocartilage Complex Injury Gary E. McIlvain, EdD, LAT, ATC; Neil A. Evans, PT, DPT, OCS, CSCS; and Suzanne M. Konz, PhD, ATC, CSCS • Marshall University; Timothy A. Tolbert, PhD, ATC • Georgia Gwinnett College; John J. Jasko, MD and Charles E. Giangarra, MD, FAAOS • Marshall University O ne of the most common wrist complaints is vague ulnar-side pain.1-3 In many cases, a single traumatic event is the cause of pain, which may delay diagnosis of the cause.1-5 When evaluating the wrist, an athletic trainer should use a systematic process, since triangular fibrocartilage complex (TFCC) injury is often missed when it first occurs. A nonspecific diagnosis of wrist sprain is often associated with subsequent development of chronic Key Point ulnar-side wrist pain. Complaints of clicking, Triangular Fibrocartilage Complex (TFCC) popping, worsened pain injury is often dismissed as a wrist sprain. over time, ulnar-side pain Vague ulnar-side wrist pain may be the elicited by functional utiresult of TFCC injury. lization (e.g., attempting a hockey goal shot), grip Isolated ulnar styloid process fracture often strength weakness, and involves TFCC injury. unstable sense of instability are common. TFCC injury is sometimes referred to as the “wrist sprain that never goes away.” Acute TFCC injury is typically caused by a fall on a pronated and outstretched arm, which forces the wrist into extension. Some athletic activities, such as gymnastics, repetitively impose axial loading on the ulnocarpal, and radiocarpal joints may injure the TFCC, but sports that load the wrist during open-chain function, such as hockey, baseball, basketball, and football, can also damage the structure.2,3,5,6-9 A risk factor for TFCC injury is positive ulnar variance, which is a more distal position of the ulna in relation to that of the radius. Positive ulnar variance normally occurs during pronation of the forearm. Some athletes exhibit a positive ulnar variance in any position, however, which may be due to genetics or a previous fracture of the distal radius. This abnormal structural alignment has been associated with thickening of the TFCC and an altered distribution of forces created by rotational and compressive loads.10,11 Werner et al.12 reported that as little as 2.5 mm of ulnar length increase elevates compressive load-bearing on the ulnar side of the wrist by 18.4% to 41.9%. Because positive ulnar variance is a major predisposing factor for TFCC injury, a thorough history of previous wrist injuries and a clear description of the exact mechanism that caused an acute wrist injury may create a high index of suspicion that TFCC damage has occurred (Figure 1). Anatomy and Function The bony structure of the wrist includes the distal portions of the ulna and radius and the eight carpal bones. The proximal row of carpals and the transverse carpal ligament define the boundaries of the carpal tunnel.13 Many elongated soft tissue structures cross © 2013 Human Kinetics - IJATT 18(3), pp. 37-42 international journal of Athletic Therapy & training may 2013 37 the wrist, and numerous fibrous tissues stabilize the joints that collectively contribute to wrist function. Key passive stabilizers include the palmar and dorsal carpal ligaments, ulnocarpal ligaments, radiocarpal ligaments, and the TFCC.13 The three-dimensional structure of the TFCC is comprised of the dorsal and palmar radioulnar ligaments, the ulnar collateral ligament, the annular (articular) disc, the meniscus homologue, and the tendon sheath of the extensor carpi ulnaris muscle (Figure 2).1,5,17-20 The TFCC primarily stabilizes the distal radioulnar joint and helps to stabilize the ulnocarpal joint. The structure also dissipates axial loads and translational forces, transfers loads from the carpal bones to the ulna, and guides complex movements of the wrist.2,14-18 Identification of TFCC Because an athlete with a TFCC injury may relate a vague history and often cannot identify a clear mecha- nism of injury (MOI) associated with a single traumatic event, such an injury tends to be perplexing and is often treated as a simple wrist sprain.1-6 The athletic trainer should include TFCC injury in the differential diagnosis when gathering information about the history of the injury and attempting to identify the MOI. A detailed history of all previous wrist injuries is important to consider. Injury to the TFCC often involves a cycle of initial pain, resolution of pain, and recurrence of pain that coincides with return to normal activity. This pattern should create a high index of suspicion that a TFCC injury may have occurred, and the condition should be included in the differential diagnosis with fracture, sprain, strain, and carpal dislocation/ instability.9,14,21 TFCC injury can be degenerative in the older populaton.2 A classification system for TFCC tears was developed by Palmer,2 who reported that acute tears typically occur in patients who are less than 30 years of age, whereas degenerative injury is more common among patients who are older than 30 years of age. Figure 1 (A) depicts a negative ulnar variance, (B) depicts a neutral ulnar variance, while (C) depicts a positive ulnar variance. Figure 2 The TFCC. Used by permission. Illustrations by Dr. Michael E. Stadnick, MD. Http://www.radsource.us/clinic/0507. 38 may 2013 international journal of Athletic Therapy & training Physical Exam Acquisition of a detailed history is crucial for determination of the likelihood that the TFCC has been injured, which may require an athletic trainer to ask the same questions in a variety of ways by using different terminology.9,13,14 Typically, the patient will report pain when he or she tries to grip, pronate, or supinate the forearm (e.g., turning a doorknob or putting a spin on a basketball when bounce passing). Observation of the wrist should include a visual search for any evidence of pallor, edema, ecchymosis, or structural deviations, including assessment of the alignment of the metacarpophalangeal joints (Figure 3). Palpation of bony structures is important for determination of any specific sites of point tenderness. TFCC pain might not be elicited by palpation, but the space beyond the distal end of the ulna that is between the extensor carpi ulnaris and flexor carpi ulnaris tendons may be painful. Active ROM is often limited in the presence of a TFCC injury, which primarily restricts extension and ulnar deviation. Specific clinical tests may be helpful in differentiating a TFCC injury from other wrist pathology.3,11,12,18 The TFCC Compression Test involves axial loading, ulnar deviation, and rotation, which is also referred to as loaded circumduction (Figure 4). The Active Pronation/Supination Test involves repetitive performance of active pronation and supination of the forearm while the examiner palpates the distal radioulnar joint for snapping and popping (Figure 5). The Active Press Test is performed by the patient through an attempt to vertically lift his or her body mass from a seated position (Figure 6). The Ulnomeniscal-Triquetral Dorsal Glide Test involves the examiner’s attempt to manually displace the triquetrum dorsally, while stabilizing the distal ulna (Figure 7). The Ballottement Test involves manual translation of the distal ulna and radius in opposite directions within the saggital plane (Figure 8).9,14 Diagnosis Diagnostic imaging is necessary to conclusively establish a diagnosis of TFCC injury, and MRI is considered to be the best method.4,14 Leakage of injected dye into the substance of the TFCC, or leakage from the carpus into the distal radioulnar joint, will confirm the diagnosis (Figure 9). Because the TFCC has an attachment to Figure 4 TFCC Compression Test. The examiner axially loads the patient’s wrist, passively ulnar deviates the patient’s wrist, and circumducts the wrist. Figure 5 Active pronation/ supiFigure 3 Murphy’s Sign — A visual appearance of depressed 3rd MCP, typically associated with a Lunate dislocation or Metacarpal fracture. In this normal 2–4 MCP curvature, if the 3rd MCP would drop to or below the dotted line, it would be considered positive. international journal of Athletic Therapy & training nation test. Examiner palpates the radioulnar joint while the patient actively pronates and supinates noting any popping or clicking. Figure 6 Active press test. Patient attempts to lift him/ herself vertically off of a surface. may 2013 39 Figure 7 Ulnomeniscal-Triquetral Dorsal Glide Test. With the forearm in neutral, the therapist places his/her same thumb on the head of the ulna and the 2nd/ 3rd distal phalange on the pisiform/triquitrum. The examiner then applies a pinch grip moving the pisiform/triquitrum dorsally with the 2nd/ 3rd finger while stabilizing the distal ulna with the thumb. A positive test is indicated by laxity of the TFCC and pain on or near the patient’s pisiform/triquitrum. Figure 8 Ballottement Test. Grasping the uylna and radium (1) attempt to translate the ulna anteriorly and the radium posteriorly simultaneously, then (2) attempt to translate the ulna posteriorly and the radius anteriorly simultaneously (oscillating the ulna a radius in opposite directions stressing the TFCC). the styloid process of the ulna, evidence of an isolated ulnar styloid process fracture on a plain radiograph should create a high index of suspicion that a TFCC injury exists.22 Treatment of TFCC Conservative treatment of a peripheral TFCC injury that resulted from an acute traumatic event often involves immobilization for 4–6 weeks, which is followed by a rehabilitation program (Table 1). Acute tears of the peripheral portion have an adequate blood supply to permit tissue healing.8,15,16 If conservative treatment is not effective, or the injury to the TFCC is located in the central portion, arthroscopic or open surgery is often warranted.16,23-26 Postsurgical rehabilitation differs on the basis of surgical debridement versus TFCC repair. Any type of surgical repair requires up to 6 weeks of cast immobilization, whereas postsurgical management of a debridement procedure simply requires splinting in a neutral position for 2 weeks 40 may 2013 Figure 9 Arthrogram MRI. (A) shows a TFCC tear while (B) shows dye that has leaked from the wrist space into the distal radioulnar joint space (Table 2). Recently, platelet-rick plasma injection has been advocated as a treatment option, but insufficient research evidence currently exists to establish the clinical effectiveness of the procedure.8, 27-30 Nonsurgical management of a TFCC injury generally consists of a period of immobilization, which is followed by emphasis on restoration of normal ROM. Active-assistive ROM exercises are initially used, which are followed with passive ROM exercises. Strengthening is progressed from isometric exercises to isotonic open-chain exercises and gradual progression to the application of weight-bearing loads to the upper extremity during a late stage of the rehabilitation process. Compressive loading in a position of forearm pronation should be avoided for a period of 8–10 weeks due to the positive ulnar variance that is produced.28 With proper rehabilitation, an athlete should be able to return to play around 12–14 weeks postinjury.29-31 Shih and Lee32 reported that 90% of patients reported a good to excellent outcome following proper treatment. Conclusion Persistent ulnar-side wrist pain should prompt a thorough assessment for the possible existence of a TFCC injury. TFCC injury may result from an acute wrist sprain and may be associated with a fracture, but it can also result from repetitive trauma cannot be related to a single traumatic event.2,3,5-9 It is often overlooked or misdiagnosed as a wrist sprain until recurrent pain motivates the patient to seek further care. The patient will typically complain of ulnar-side wrist pain during activity, which resolves when activity international journal of Athletic Therapy & training Table 1. Nonsurgical Rehabilitation Week Exercise 1-6 Splinted in neutral 7 Active-Assistive ROM for wrist and forearm 8 Passive ROM for wrist and forearm. Weighted static stretches. Isometric strengthening for wrist and forearm 9 Continue ROM. Begin PRE strengthening with putty and/or hand grip strength exerciser 10-18 Continue ROM. Begin isotonic PRE exercises for wrist and forearm Baseball and Softball Sport Specific Progression 11 Begin swinging light bat and short throwing 12 Begin swinging regular bat and increasing throwing distance gradually 13 Begin hitting off of a tee and increasing throwing distance and speed 14 Increase hitting/throwing repetitions and progress intensity 15 Progress to hitting live pitches (only making contact and swinging through) 16-18 Progress to full batting and pitching/throwing Table 2. Postsurgical Management of a Debridement Procedure Central Debridement Peripheral Repair Week Exercise Week Exercise 1 NONE; focus is on wound care, pain control, and immobilization. 1-6 Casted in neutral 2 Active-assistive ROM for wrist and forearm. 7 Active-assistive ROM for wrist and forearm. 3-4 Passive ROM for wrist and forearm. Weighted static stretches. 8 Passive ROM for wrist and forearm. Weighted static stretches. Isometric strengthening for wrist and forearm. 6 Continue ROM. Begin PRE strengthening with putty and/or hand grip strength exerciser. 9 Continue ROM. Begin PRE strengthening with putty and/or hand grip strength exerciser. 7-14 Continue ROM. Begin isotonic PRE exercises for wrist and forearm. 10-18 Continue ROM. Begin isotonic PRE exercises for wrist and forearm. Baseball and Softball Sport Specific Progression Baseball and Softball Sport Specific Progression 8 Begin swinging light bat and short throwing. 11 Begin swinging light bat and short throwing. 9 Begin swinging regular bat and increasing throwing distance gradually. 12 Begin swinging regular bat and increasing throwing distance gradually. 10 Begin hitting off of a tee and increasing throwing distance and speed. 13 Begin hitting off of a tee and increasing throwing distance and speed. 11 Increase hitting/throwing repetitions and progress intensity. 14 Increase hitting/throwing repetitions and progress intensity. 12 Progress to hitting live pitches (only making contact and swinging through). 15 Progress to hitting live pitches (only making contact and swinging through). 13-14 Progress to full batting and pitching. 16-18 Progress to full batting and pitching/throwing. international journal of Athletic Therapy & training may 2013 41 is stopped, and he or she often cannot relate it to any specific incident.1-3Diagnosis of a TFCC injury requires a systematic physical examination, which guides referral for appropriate diagnostic imaging. Conservative treatment is not always successful, but surgical management and proper rehabilitation typically produce a favorable outcome. References 1. Palmer AK. The distal radioulnar joint: anatomy, biomechanics, and triangular fibrocartilage complex abnormalities. Hand Clin. 1987;3;3140. 2. Palmer AK. Triangular fibrocartilage complex lesions: a classification. J. Hand Surg Am 1989;14(4):594-606. 3.Haugstvedt J, Berger RA, Nakumura T, Neale P, Berglund L, An K. Relative contributions of the ulnar attachments of the triangular fibrocartilage complex to the dynamic stability of the distal radioulnar joint. J Hand Surg Am. 2006;31(3):445-451. 4. Nishikawa S, Toh S, Miura H, Arai K. The carpal detachment injury of the triangular fibrocartilage complex. J Hand Surg Br. 2002;27(1):8689. 5. Palmer K, Werner FW, Mech-Eng M. The triangular fibrocartilage complex of the wrist – anatomy and function. J Hand Surg Am. 1981:6(2) 6.Baratz M. Central TFCC tears in baseball players. Hand Clin. 2012;28(3):339. 7. Birbeck, DP. Overview of hand and wrist injuries in athletics. Athl Ther Today. 2001;6(1):6-12. 8. Wiedrich TA. The treatment of TFCC injuries in football players. Hand Clin. 2012;28(3):327-328. 9.Poirier M, Demont R. Complication from triangular fibrocartilagecomplex degenerative tear. Athl Ther Today. 2002;7(1):30-31. 10. Yoshioka H, Tanaka T, Ueno T, et.al. Study of ulnar variance with highresolution MRI: correlation with triangular fibrocartilage complex and cartilage of ulnar side of wrist. J Magn Reson Imaging. 2007;26(3):714719. 11.Markolf KL, Tejwani SG, Benhaim P. Effects of wafer resection and hemiresection from the distal ulna on load-sharing at the wrist: a cadaveric study. J Hand Surg Am. 2005;30(2):351-358. 12.Werner FW, Glisson RR, Murphy DJ, Palmer AK. Force transmission through the distal radioulnar carpal joint: effect of ulnar lengthening and shortening. Handchir Mikrochir Plast Chir. 1986;18(5):304308. http://www.scopus.com/record/display.url?eid=2-s2.00022512751&origin=inward&txGid=DD1AEDDB6A51BF931F1 D2FB87C2CCFC9.WlW7NKKC52nnQNxjqAQrlA%3a2. Retrieved 12/19/2012. 13.Starkey C, Ryan J, Evaluation of Orthopedics and Athletic Injuries. Philadelphia, PA: F.A. Davis; 2002: 86-126 14.Bae DS, Waters PM. Pediatric distal radius fractures and triangular fibrocartilage complex injuries. Hand Clin. 2006;212(1):43-53. 15. Dell PC. Distal radioulnar joint dysfunction. Hand Clin. 1987;3(4):563583. 16.Gerlach DJ, Chun KF, Trumble TE. Triangular fibrocartilage complex repair through bone tunnels (Palmwer Type 1D). Oper Tech Sports Med. 2010;18(3):173-180. 17. Nakamura T, Yabe Y, Horiuchi Y. Functional anatomy of the triangular fibrocartilage complex. J Hand Surg Br. 1996;21(5):581-586. 18.Palmer AK, Werner FW, Mech-Eng M. Biomechanics of the distal radioulnar joint. Clin Orthop RelatRes. 1984;187:26-36. 42 may 2013 19. Nakamura T, Takayama S, Houriuchi Y, Yabe Y. Origins and insertions of the triangular fibrocartilage complex: a histological study. J Hand Surgery Br. 2001;26(5)446-454. 20.Nakamura T, Makita A. The proximal ligamenous component of the triangular fibrocartilage complex. J Hand Surg Br. 2000;25(5):479-486. 21. De Smet LD, Claessens A, Fabry G. Gymnast wrist. Acta Orthop Belg. 1993;59(4):377-380. 22.Atzei A, Luchetti R. Foveal TFCC tear classification and treatment. Hand Clin.2011;27(3):263-272. 23.Kalainov DM. Arthroscopic treatment of TFCC tears. Tech Hand Up ExtremSurg. 1997;1(3):175-182. 24.Ko JH, Wiedrich TA. Triangular fibrocartilage complex injuries in the elite athlete. Hand Clin. 2012;28(3);307-321. 25.Nakamura T, Sato K, Okazaki M, Toyama Y, Ikegami H. Repair of foveal detachment of the triangular fibrocartilage complex: open and arthroscopic transosseous techniques. Hand Clin. 2011;27(3):281-290. 26. Wysocki Rw, Ruch DS. Outside-in repair of peripheral triangular fibrocartilage complex tears. Oper Tech Sports Med. 2010;18(3):163-167. 27. Chong CH. Platelet rich plasma injection for musculoskeletal injuries. http://orthopaedicsports.com/2011/04/22/platelet-rich-plasma-injectionfor-musculoskeletal-injuries/. Retrieved 12/16/2012. 28. Lox D. Triangular fibrocartilaginous complex (TFCC). http://www.drlox. com/index.php?option=com_content&view=article&id=82. Retrieved 12/16/2012. 29.Harvey NM. Baseball commentary ‘Traumatic TFCC tear’. Hand Clin. 2012;28(3):323-324. 30.Nagle DJ. Triangular fibrocartilage complex tears in the athlete. Clin Sports Med. 2001;20(1):155-166. 31. Green JB, Ranger HE, Draghetti JG, Groat LC, Schumer ED, Leslie BM. Hand, wrist, and digit injuries. In: Magee D, Zachazewski J, Quillen W. Pathology and Intervention in Musculoskeletal Rehabilitation. St. Louis, MO: Saunders, Elsevier; 286-287. 32.Shih, J, Lee, H. Functional results post-triangular fibrocartilage complex reconstruction with extensor carpi ulnaris with or without ulnar shortening in chronic distal radioulnar joint instability. Hand Surg. 2005;10(2 &3):169-176. Gary McIlvain is an associate dean for the College of Health Professions, Chair of the School of Kinesiology, and an associate professor at Marshall University in Huntington, WV. Neil Evans is an assistant professor in the School of Physical Therapy at Marshall University, Huntington, WV. Suzanne Konz is the Director of the Biomechanics Laboratory and an assistant professor in the School of Kinesiology at Marshall University, Huntington, WV. Timothy Tolbert is an assistant professor in the School of Science and Technology at Georgia Guinnett College in Lawrenceville, GA. John J. Jasko is an orthropedic surgeon and a team physician for Marshall University Athletics and an assistant professor in the Joan C. Edwards School of Medicine Department of Orthropedic Surgery, Marshall University in Huntington, WV. Charles Giangarra is Chief of Marshall Athletics and Orthopaedic Sports Medicine and a professor in the Joan C. Edwards School of Medicine Department of Orthopedic Surgery, Marshall University in Huntington, WV. Monique Mokha, PhD, ATC, Nova Southeastern University, is the report editor for this article. international journal of Athletic Therapy & training