Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
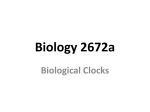
ARTICLE IN PRESS Sleep Medicine Reviews (2008) -, -e- www.elsevier.com/locate/smrv Clinical review A practical approach to circadian rhythm sleep disorders Bjørn Bjorvatn a,b,c,*, Ståle Pallesen b,c,d a Department of Public Health and Primary Health Care, University of Bergen, Kalfarveien 31, N-5018 Bergen, Norway b Norwegian Competence Center for Sleep Disorders, Haukeland University Hospital, Norway c Bergen Sleep Disorders Center, Bergen, Norway d Department of Psychosocial Science, University of Bergen, Norway KEYWORDS Circadian rhythm disorders; Bright light; Melatonin; Nadir; Sleep regulation Summary Circadian rhythm sleep disorders are common in clinical practice. The disorders covered in this review are delayed sleep phase disorder, advanced sleep phase disorder, free-running, irregular sleepewake rhythm, jet lag disorder and shift work disorder. Bright light treatment and exogenous melatonin administration are considered to be the treatments of choice for these circadian rhythm sleep disorders. Circadian phase needs to be estimated in order to time the treatments appropriately. Inappropriately timed bright light and melatonin will likely worsen the condition. Measurements of core body temperature or endogenous melatonin rhythms will objectively assess circadian phase; however, such measurements are seldom or never used in a busy clinical practice. This review will focus on how to estimate circadian phase based on a careful patient history. Based on such estimations of circadian phase, we will recommend appropriate timing of bright light and/ or melatonin in the different circadian rhythm sleep disorders. We hope this practical approach and simple recommendations will stimulate clinicians to treat patients with circadian rhythm sleep disorders. ª 2008 Elsevier Ltd. All rights reserved. Introduction * Corresponding author. Department of Public Health and Primary Health Care, University of Bergen, Kalfarveien 31, N-5018 Bergen, Norway. Tel.: þ47 55 58 61 00; fax: þ47 55 58 61 30. E-mail address: [email protected] (B. Bjorvatn). Circadian rhythm sleep disorders are caused by a misalignment between the endogenous circadian timing system and the external 24-h environment. The disorders typically result in complaints of insomnia and/or excessive sleepiness, in addition to impairment in normal functioning and quality of 1087-0792/$ - see front matter ª 2008 Elsevier Ltd. All rights reserved. doi:10.1016/j.smrv.2008.04.009 Please cite this article in press as: Bjorvatn Bjø, Pallesen Stå, A practical approach to circadian rhythm sleep disorders, Sleep Medicine Reviews (2008), doi:10.1016/j.smrv.2008.04.009 ARTICLE IN PRESS 2 life. Many clinicians face patients suffering from such complaints, but there is lack of evidencebased guidelines on how to diagnose, examine and treat these disorders.1,2 This review provides a practical approach to handling the different circadian rhythm sleep disorders, as they are defined in the International Classification of Sleep Disorders.3 Although the practical approach presented here is not based on firm evidence drawn from controlled clinical trials, the approach is based on well-researched basic principles of circadian entrainment. We would also like to emphasize that although there is a definite need for more research on practical issues concerning treatment, the clinical approach which is presented here will likely help many of the patients suffering from circadian rhythm sleep disorders. Based on our long-term clinical experience in diagnosing and treating such disorders, we have found that treating these patients is usually easier than many clinicians believe. To be able to treat patients with circadian rhythm sleep disorders, it is important to understand how sleep is regulated. Thus, we will initially focus on sleep regulation, and how to determine circadian phase. Then we will cover each separate circadian rhythm sleep disorder,3 and specify a simple and clinical approach on how to treat patients suffering from these disorders. The advantage of a clinical approach is that the specific interventions can be adjusted, if the treatment does not help or if the condition actually worsens. This is especially important in these disorders, where the timing of the treatment is crucial. This means that if treatment is instituted at the inappropriate circadian time, the patients are likely to get worse. The treatment options in ordinary clinical practice for circadian rhythm sleep disorders comprise bright light treatment and exogenous melatonin administration. How to use these treatment options will be covered under each specific circadian rhythm sleep disorder. Chronotherapy has been used for the treatment of some of the circadian rhythm sleep disorders, but we will not discuss this any further in our review, due to the difficulties of implementing such an approach and lack of data documenting its efficacy. Furthermore, we will not cover use of hypnotics or other medications, due to space limitations. We have epidemiological data for many of the different circadian rhythm sleep disorders, but the number of patients who actually seek treatment for these disorders is much less. The reasons may be many. One probable reason is lack of knowledge B. Bjorvatn, S. Pallesen about the disorders and their possible treatments, both among health professionals and patients. Sleep regulation Sleep is regulated by an interplay of different factors. The main focus has been on the interaction between the homeostatic and the endogenous circadian processes.4 The homeostatic process accumulates as a function of prior wakefulness, i.e., there is more homeostatic factor the longer you are awake.5 This factor is believed to be of main importance for sleep quality; that is, the longer you are awake, the deeper the following sleep episode will be (increased slow wave activity). The circadian factor on the other hand plays an important role in sleep quantity; that is, sleep duration is for the most part determined by when you go to bed. In other words, sleep length is not dependent on the sleep homeostatic factor, but largely dependent on when you go to sleep according to your own circadian rhythm.4 Night workers have experienced this as their sleep duration is usually shorter (often less than 6 h) than normal when going to bed in the morning, even though they often have been awake for more hours before going to bed than daytime workers.6 From a practical point of view, this interaction between the homeostatic and circadian processes means that it is important to be awake for a substantial amount of time to get sleep of high quality, and to have regular bed and rise times in order to have a stable sleep duration. Also habits and behavioral factors have large influences on sleep. We all go to bed at regular hours, not necessarily because we are very sleepy/ tired, but because we know we need to do so, to get enough sleep. Many people experience a high level of sleepiness early in the evening/afternoon, but avoid going to bed knowing that it is not time for bed yet. Behavioral factors can override both the homeostatic and circadian factors. For instance, a night worker is able to stay awake even though both the homeostatic and the circadian factors favor sleep in the middle of the night. In these instances behavioral factors, like talking to someone, walking around, drinking coffee, increasing illumination, etc., help the night workers to stay awake. Similarly, many teachers have experienced students falling asleep at 9 a.m., even though both the homeostatic and circadian factors favor wakefulness. In this instance, lack of stimulation may be a behavioral factor explaining the increase in sleepiness and risk of falling asleep; that is, a boring lecture, sitting in a dark room, lack of sensory input, etc. Please cite this article in press as: Bjorvatn Bjø, Pallesen Stå, A practical approach to circadian rhythm sleep disorders, Sleep Medicine Reviews (2008), doi:10.1016/j.smrv.2008.04.009 ARTICLE IN PRESS Estimating circadian phase in every day clinical practice Core body temperature and endogenous melatonin rhythms For the treatment of circadian rhythm sleep disorders, an understanding of the circadian timing system is of crucial importance. Of central importance is the determination of the circadian phase, i.e., the nadir of the core body temperature rhythm, or the endogenous melatonin rhythm. For simplicity, we will primarily focus on the nadir of the core body temperature rhythm, and the role of this nadir when recommending correct timing of treatment of the different circadian rhythm sleep disorders. The core body temperature usually peaks in the late afternoon or evening hours, and reaches its lowest point, nadir, in the early morning (Fig. 1). Sleep normally occurs on the downward slope of the core body temperature rhythm and normally ends about 2 h following nadir. A similar coupling between the sleep/wake-rhythm and the rhythmicity of the melatonin secretion is also normally present. Melatonin secretion usually increases soon after the onset of darkness, peaks in the middle of the night and gradually falls during the second half of the night. Sleep usually takes place when the melatonin level is high, and wakefulness normally coexists with low plasma melatonin levels. Based on the close correspondence between sleep/wakefulness and body temperature/melatonin, the core body temperature and melatonin (measured in saliva, urine or plasma) constitute the two most common physiological measures of circadian rhythm.1,7,8 Interestingly, mammals continue to show periodic regularity in sleep and wakefulness also in the absence of light or other time signalling stimuli (zeitgebers). This has also been demonstrated in studies with human subjects, kept isolated in underground bunkers. However, the period of the sleep/wake-rhythm under such conditions was reported to be 37.4 Temperature in °C 37.2 37.0 36.8 36.6 36.4 36.2 36.0 19 21 23 1 3 5 7 9 11 13 15 17 Time of day Figure 1 Core body temperature rhythm. 3 somewhat longer than 24 h, approximately 25 h.9 Several studies have now confirmed that humans are in possession of an endogenous circadian rhythm, with a period length under controlled conditions of about 24.2 h.10 The main site of this endogenous rhythm has been located in the suprachiasmatic nuclei (SCN), situated bilaterally above the optic chiasm in the anterior basal hypothalamus.11 Ablation of the SCN in mammals has been shown to eliminate circadian rhythms, and transplantation restores the rhythm to the period of the donor animal.12 There exist several major input fiber systems in the SCN. The most important stems from photoreceptors in the retina, which convey signals to the suprachiasmatic nucleus via a monosynaptic pathway, the retinohypothalamic tract. Recently, it was discovered that the retinal rod and cone cells are not required for photoentraiment, but that there exists a subset of retinal cells (2500 of a total of 100 000 cells) containing a light-sensing pigment, melanopsin, which is assumed to be involved in circadian photoentrainment.13 There exists an important connection between the SCN and the pineal gland. Melatonin, which is the only known hormonal output from the pineal gland, affects the SCN by inhibiting firing.14 Hence, the SCN and pineal gland seem to be able to influence each other in a mutual way. Estimation of circadian phase To be able to measure the circadian phase of a patient in an objective manner, either core body temperature or melatonin (in saliva, urine or blood) must be assessed. In laboratory based studies core body temperature rhythm is normally measured by the so-called constant routine protocol. This protocol implies that the patient takes on a semi-recumbent position in a laboratory environment for several (often 26) consecutive hours. The light intensity is required to be less than 50 lux and the patient normally receives a meal of 100 kcal every hour.15 The commonly used circadian parameter obtained from this protocol is the nadir (time of the lowest level measured) of the core body temperature. Measurement of the circadian rhythm based upon melatonin comprises several samples (normally with a 30 or 60 min interval) of either saliva, urine or plasma. The level of illumination currently recommended for sampling is 10 lux.16 The most commonly used parameter from these measures is the dim light melatonin onset (DLMO), normally defined as the time when the melatonin level reaches 2 pg/ml in plasma17 or when a level of Please cite this article in press as: Bjorvatn Bjø, Pallesen Stå, A practical approach to circadian rhythm sleep disorders, Sleep Medicine Reviews (2008), doi:10.1016/j.smrv.2008.04.009 ARTICLE IN PRESS 4 4 pg/ml is reached in saliva.18 Alternatively, the threshold for DLMO can be defined as the mean of 3 daytime samples plus two times the standard deviation of these 3 daytime samples.19 Measurements as described above are cumbersome and expensive, and for these reasons seldom or never performed in a busy clinical practice. Thus, we will here emphasize how to estimate circadian phase by taking a careful patient history. As a rule of thumb, the nadir of the core body temperature is located about 2 h before habitual time of awakening. For patients with stable circadian rhythms, that is, stable bed and rise times, estimation of nadir is relatively easy. For instance, if the patient usually wakes up at about 8 a.m. every day, the nadir of the core body temperature rhythm is likely to be some time around 6 a.m. Some patients may have stable bed and rise times during the workweek, but during the weekend, this rhythm is delayed by several hours. Estimation of nadir is more complicated in such cases. Furthermore, use of medications/drugs, alcohol or irregular work schedules can make estimation of nadir very difficult. Before instituting treatment, it may be helpful to instruct the patient to sleep until she or he wakes up (without an alarm clock). It is likely that nadir will be about 2 h before his/her awakening. Previous studies have shown that subjective sleep data from uninterrupted sleep can be used as a reasonable good estimate of circadian phase,20,21 and that sleep offset correlates higher with different phase markers than sleep onset.21,22 Nadir is, in addition to being the lowest point on the core body temperature rhythm, the time where it is most difficult to stay awake.23 Night workers often experience an increase in sleepiness during the night until about 4 or 5 in the morning, and after that, they usually become less sleepy. Since the time point when the patient is most sleepy during the night corresponds to the nadir, this may be used as an additional help for estimating the nadir, particularly in night work and jet lag. For other circadian rhythm sleep disorders, where the patients may not have been awake during their regular sleep episode, this approach for estimating the nadir may not be possible. Bright light treatment An important function of the SCN is to adjust the output signals and the endogenous rhythm in accordance with external time signalling stimuli (zeitgebers). The afferent connections of the SCN indicate that it is particularly sensitive to light, and light is now considered the most important B. Bjorvatn, S. Pallesen zeitgeber. The process by which light synchronizes the SCN to a 24-h day is called entrainment. A human living in a natural habitat will adhere to a 24-h day, primarily due to light exposure. But the SCN is not equally sensitive to the effect of light at all time points during the day, and the type of effect light exposure has on the circadian rhythm is also related to the duration of the light exposure. Studies, using a variety of experimental designs, have now consistently shown that the effect of light on circadian rhythms follows a socalled phase-response curve (PRC).24 According to the PRC, light can have two opposite effects on the circadian rhythm (Fig. 2). Light exposure before the nadir of the core body temperature rhythm causes a phase delay, whereas light administered after nadir produces a phase advance. Thus, light in the evening normally causes phase delay, and light in the morning causes phase advance. Also, light exposure close to the nadir produces the greatest phase shifts. It follows that the further away from nadir light exposure takes place, the less effect it exerts.25 The magnitude of phase shifts is also a function of the dose and duration of the light exposure. In general, high intensity light doses and long durations of light exposure cause the greatest phase shifts.26 For long durations of light that fall on both the phase advance and delay portions of the PRC, the direction of the resulting phase shift is influenced by where most of the light falls.24,27,28 Hence, light can advance or delay the circadian rhythm depending on time of light exposure. Today, bright light is typically administered by portable units yielding about 10 000 lux, and Figure 2 Phase-response curve for light (full line) and melatonin (dotted line) based upon Khalsa et al.24 and Lewy et al.8 A phase-response curve illustrates the relationship between the timing and the effect of a treatment designed to affect circadian rhythms. The differences in effect between light and melatonin are not necessary as shown in this figure but will depend on the doses of light and melatonin. Please cite this article in press as: Bjorvatn Bjø, Pallesen Stå, A practical approach to circadian rhythm sleep disorders, Sleep Medicine Reviews (2008), doi:10.1016/j.smrv.2008.04.009 ARTICLE IN PRESS Estimating circadian phase in every day clinical practice exposure time is about 30e45 min per day. Studies have also investigated the effects of presenting light of different wavelengths. Visible light with short wavelengths (blue light) has a stronger melatonin suppressing effect and a stronger phase shifting effect on the human circadian rhythm compared to light with longer wavelengths.1 During light exposure the patient is instructed to keep his gaze directed at the light source, but not to continuously stare into the light. A potential problem with small apparatus is that even small changes in head position sometimes can lead to substantial reductions in the light intensity that reaches the eyes, hence reducing the therapeutic effect.29 Light treatment can be self-administered at home, according to a therapeutic regime. To the extent that the timing of light treatment is important in order to obtain a therapeutic effect, compliance is sine qua non.29 Patients may read the newspaper, watch television, or eat while being exposed to bright light. Bright light of 10 000 lux for at least 30 min is recommended, but light of less intensity or shorter duration will be better than no light at all. Furthermore, whenever outdoor light of sufficient intensity is available, being outdoors is preferable to sitting in front of a light box. Side effects The side effects of bright light therapy are usually mild and of short-term duration. Side effects have primarily been investigated in patients with seasonal and nonseasonal mood disorders. Thus, information is by and large lacking for sleep disorders without mood disturbance.29 One of the most potential damaging consequences of bright light is permanent injuries of the eyes.30 However, in a longitudinal study with thorough ophthalmologic examinations performed before and after short-term treatment of 10 000 lux (2e8 weeks) of 50 patients, and before and after 3e6 years of treatment with 10 000 lux of 17 patients, with cumulative treatment durations of 60e1250 h, no ocular abnormalities were detected.31 We have no knowledge of any study that has documented eye damage due to light therapy administered according to the standard procedures. In the study by Pallesen et al.,32 investigating the effects of bright light treatment in older adults suffering from early morning awakening, the most common side effects were eyestrain (29%) and headache (19%). Unexpectedly, the number of side effects was greater in the placebo compared to the active treatment condition. Most of the side effects were transient.33 Some rare cases of mania as a side effect of phototherapy have been reported, also in 5 patients who prior to light treatment only had shown symptoms of unipolar depression.34,35 Melatonin treatment Exogenously administered melatonin has phase shifting properties, and the effect follows a phaseresponse curve (PRC) that is about 12 h out of phase with the PRC of light.1,8,36 Melatonin administered in the afternoon or early evening will phase advance the circadian rhythm, whereas melatonin administered in the morning will phase delay the circadian rhythm (Fig. 2). The magnitude of phase shifts is time-dependent, and the maximal phase shifts result when melatonin is scheduled around dusk or dawn.36 The effect of exogenous melatonin is minimal when administered during the night, at least during the first-half of the night.37 Furthermore, similar to the effects of bright light, melatonin administered at an inappropriate time can actually worsen the patient’s condition. Melatonin has, in addition to phase shifting properties, soporific effects. This is seen especially when taking melatonin medication during the daytime, when endogenous melatonin is low.36 This effect may account for some of its benefit in the treatment of jet lag and shift work disorder. There is no consensus regarding the appropriate dose or formulation of melatonin. Most studies use fast-release melatonin, but sustained-release preparations are commercially available. The doses used in most studies range from 0.5 to 5 mg. Several studies show that the effects of melatonin are not clearly dose-related,1 and the phase shifting effect is considered less than those associated with light exposure. Side effects In general, melatonin seems to be well-tolerated, and few serious side effects have been reported to date. However, there is a lack of long-term studies, and little is known about the possible drug interactions.36 Side effects may include elevation of blood pressure, headache, dizziness, nausea and drowsiness.38 Delayed sleep phase disorder Case history John, a 17-year-old high school student, seeks help because of problems of falling asleep at Please cite this article in press as: Bjorvatn Bjø, Pallesen Stå, A practical approach to circadian rhythm sleep disorders, Sleep Medicine Reviews (2008), doi:10.1016/j.smrv.2008.04.009 ARTICLE IN PRESS 6 night. He rarely gets any sleep until 3 a.m. in the morning, and he has major problems waking up in the morning in time for school. He has missed school many days because of this problem, and he will not pass the exams, if this continues. When allowed, he can easily sleep until noon or 1 p.m. Thus, he is able to sleep for more than 7 h in free periods/weekends, and he does not feel especially tired or sleepy when he gets up around noon. However, when he is forced up (usually by his parents) early in the morning, he often falls asleep during his classes. Delayed sleep phase disorder (DSPD) is assumed to be a frequent circadian rhythm sleep disorder,39 and is defined in ICSD-23 as ‘‘a delay in the phase of the major sleep period in relation to the desired sleep time and wake-up time, as evidenced by a chronic or recurrent complaint of inability to fall asleep at a desired conventional clock time together with the inability to awaken at a desired and socially acceptable time’’. When allowed to choose their preferred schedule, patients are assumed to exhibit normal sleep quality and duration for age and maintain a delayed, but stable, phase of entrainment to the 24-h sleepe wake pattern.3 However, some studies suggest that sleep quality may be poorer even when bed and wake times are self-selected.40 More studies are needed to explore these issues. The disorder is believed to be particularly common in young people, but more epidemiological studies are warranted to gain more knowledge about its prevalence.41 Studies have found a prevalence ranging from 0.13 to 0.17% in adult populations42,43 and 7.3% in adolescents.44,45 The peak of onset of DSPD seems to be in childhood or early adolescence.41 In terms of biology, DSPD is believed to be caused by anomalies of the mechanisms regulating the circadian rhythms (see review by Crowley et al.46). The subjects may have long endogenous circadian rhythms making it difficult to adjust to a 24-h sleepewake period, in particular when the light exposure is not optimal.47 The time from nadir to spontaneous awakening has been shown to be altered in patients suffering from DSPD,40,48 causing a tendency to be asleep at times when the circadian system is particularly sensitive for the phase advancing effects of light. It has been suggested that the circadian dysregulation may be linked to genetic factors, and genetic markers related to DSPD have been found.49 In addition to biological vulnerability, social factors and habits are believed to play an important role in the development of DSPD. Habits such as staying up late and ‘‘sleeping in’’ will phase B. Bjorvatn, S. Pallesen delay the circadian rhythm. Television, computers, Internet and cellular phones have made greater enticements for being awake at night,50 potentially causing a delay of sleep onset. As caffeine and nicotine have stimulating effects on the central nervous system, use of these drugs in the evening can lead to difficulties in initiating sleep. During puberty, a biological based delay of the circadian rhythm of about 2 h seems to occur,51 while the need for sleep at the same time seems to increase.52 Studies, however, indicate that adolescents do not take this into consideration and go to bed later than recommended and sleep in during weekends and holidays.46 Treatment with bright light Timed bright light has been shown to effectively phase advance the rhythm,53 but no standardized guidelines regarding the duration, intensity or timing of light exposure have been established. This is despite the fact that light has for long been known to be the most important modulator of our circadian rhythms.27 As light exposure prior to nadir causes a phase delay, subjects suffering from DSPD should avoid light during this phase, for example by wearing dark goggles in the evening. Moreover, it is very important not to wake the patient up too early in the morning, and start bright light treatment. Patients suffering from DSPD are likely to have nadir late in the morning, i.e., after 9 a.m., and bright light introduced in the early morning will phase delay the rhythm. Surprisingly, in some scientific studies bright light seems to be administered at inappropriate times, that is, before the nadir,53,54 and also recent reviews still advice early morning bright light in the treatment of delayed sleep phase disorder.45 Our clinical approach to these patients is to ask the patient to sleep without an alarm clock until she/he wakes up. This may be late morning, or for some patients in the afternoon. This procedure will make sure that the treatment is given after the nadir of the core body temperature rhythm. It is highly unlikely that any patient will wake up before his/her nadir. In our 17-year-old case history, John slept until 1 p.m., and was advised to obtain 30 min of bright light treatment (10 000 lux) immediately following rise time. The next day John was instructed to get up 1 h earlier (with help of alarm clock or parents), and start bright light treatment. The third day, bright light treatment was started at 11 a.m., the fourth day at 10 a.m., and so on. Such a procedure will ‘‘push’’ the circadian rhythm in the right Please cite this article in press as: Bjorvatn Bjø, Pallesen Stå, A practical approach to circadian rhythm sleep disorders, Sleep Medicine Reviews (2008), doi:10.1016/j.smrv.2008.04.009 ARTICLE IN PRESS Estimating circadian phase in every day clinical practice direction, and light exposure will be administered at about the same time point in the PRC from day to day. Some patients may find it very difficult to get up 1 h earlier from day to day, and the treatment can be adjusted, i.e., advancing bright light 30 min earlier from day to day. When the patient has reached the desired sleepewake rhythm, usually after less than 1 week of treatment, bright light therapy may be terminated. For most patients, however, treatment in some form should probably be continued in order to prevent relapse. Whether bright light treatment needs to be given every day, or more intermittently, for instance maintenance treatment 2e4 days per week, is unclear and likely to differ from patient to patient. In John’s case, he used bright light every day for 3 weeks, and then continued with bright light at a more intermittent manner and successfully completed his studies. Delayed sleep phase disorder and its treatment often involve family or other close relationships. Lack of school achievements may upset the parents. Adolescents who sleep until noon can cause great distress for the rest of the family. Often parents and siblings exert great effort to wake up the patient at an appropriate time in the morning. Also, during treatment the patient may need help in waking up in time for light exposure. When treatment is successful, tensions and conflicts centred around bedtime and wake-up time usually lessen. Compliance with bright light treatment is often poor, because it involves structuring the daily schedule, which may be difficult for the relevant age group. Our clinical experience is that several patients improve initially with this kind of treatment, but the compliance gradually deteriorates. Many young subjects are particularly unwilling to follow strict bed and rise time schedules during weekends. For some patients compliance may be improved by using a light visor instead of a stationary lamp, as the former allows for movement and execution of simple tasks during light exposure. The use of outdoor light if available, instead of sitting in front of a light box, may also be used to improve compliance. Treatment with melatonin Administration of melatonin in the evening has been shown to phase advance the rhythm,8,55 but similar to bright light, a standardized approach for dose, duration and timing is lacking. In clinical practice it is often recommended to administer melatonin 5e7 h before the regular time for sleep onset, in order to obtain maximal phase 7 advance.55 In a well-controlled double-blind treatment study with subjects suffering from DSPD it was found that administration of melatonin in the evening decreased sleep onset latency.56 On some subjective measures of fatigue and alertness the subjects in the melatonin group improved relative to the subjects in the placebo-group. Biological markers of circadian rhythms showed that the subjects in the melatonin-group phase advanced.56 In another study employing a similar design, therapeutic effects of melatonin on several sleep and circadian parameters, and on alertness in the morning, were found.18 In our clinical practice, we usually first recommend bright light treatment. For those patients where bright light does not work, or the effect is not satisfactory, exogenous melatonin is recommended, either alone or in combination with bright light. When melatonin and bright light treatment are employed together, melatonin is commonly administered about 12 h before the bright light exposure.57 One clinically effective method is to time melatonin similar to the way bright light is timed. To use John’s case as an illustration, melatonin will be administered 12 h before bright light treatment on day 1, i.e., at 1 a.m. On day 2, melatonin is taken at midnight, day 3 at 11 p.m., and so on. Using this method, the patient ends up with exogenous melatonin at about 8 p.m. and bright light at about 8 a.m. In clinical practice, the combined treatment seems to facilitate circadian adaptation more than each treatment alone. However, to our knowledge only one scientific paper has addressed this.58 Advanced sleep phase disorder Advanced sleep phase disorder (ASPD) is characterized by a habitual sleep period that is of normal quality and duration, but with a sleep onset and wake-up time that are several hours earlier than desired.3 ASPD is assumed to be a rare disorder and using strict criteria in a random sample of approximately 7700 adults, representative of the Norwegian population, no case of ASPD was detected.43 The prevalence in middle-aged and older adults is estimated to be 1%.3 The etiology of advanced sleep phase disorder is not well known, but studies have shown that there exists evidence in some cases suggesting that such a sleep disturbance runs in families,59 and it has been hypothesized to represent an autosomal dominant circadian rhythm variant.60 As sleep disturbances related to sleep phase advance increase with age,61 it has been suggested that this is Please cite this article in press as: Bjorvatn Bjø, Pallesen Stå, A practical approach to circadian rhythm sleep disorders, Sleep Medicine Reviews (2008), doi:10.1016/j.smrv.2008.04.009 ARTICLE IN PRESS 8 a consequence of a phase advance of the endogenous circadian pacemaker.62 Treatment Few studies have investigated the effects of bright light treatment for advanced sleep phase disorder. In one study, 16 subjects suffering from advanced sleep phase disorder were randomized to 10 days of evening bright light treatment (4000 lux for 2 h) or to a red dim light placebo condition. On completion of the treatment, there was no difference in the nocturnal awakenings between the two groups for the first two-thirds of the night, but for the last third of the night the reduction in nocturnal awakenings was significantly greater in the treatment compared to the placebo-group.63 However, negative studies are also published.32,64,65 To treat patients with ASPD, bright light should be given as close to bedtime as possible. This will likely delay the circadian rhythm, and thus delay wake-up time. One reason why the effects of bright light may not be as clear as in DSP, is that light is given many hours before the nadir. As discussed earlier, the closer to nadir the treatment is given, the larger the phase shifts.24 But to wake up the patients in the middle of the night (just before nadir) is normally not an acceptable treatment option. For these patients, exogenous melatonin administration is not a good alternative. Based on circadian principles, melatonin should be given in the morning (after nadir). However, due to the potential sedating effect of melatonin, this is seldom recommended in clinical practice.45 To conclude, evening bright light may be beneficial in advanced sleep phase disorder, but more studies are warranted in order to draw firm conclusions. Free-running The non-24-h sleepewake syndrome consists of a chronic pattern comprising 1e2 h daily delays in sleep onset and wake time. The sleepewake pattern resembles that found in normal individuals living in isolation from environmental time cues, hence the sleepewake rhythm is said to be freerunning. If patients suffering from non-24-h sleepe wake syndrome arise continually at conventional social times progressively less sleep is achieved, accompanied by daytime sleepiness. The prevalence of this syndrome is low and the majority of patients described in the literature have been blind.2 The failure to entrain circadian rhythms is related to the lack of photic input to the circadian pacemaker. B. Bjorvatn, S. Pallesen Treatment Scientific studies are sparse, and mostly based on single case reports.2 In one study, a 40-year-old sighted woman with a free-running sleepewake rhythm was treated with bright light of 2500 lux for 2 h each day upon awakening. Clock time of light exposure was held constant for 6 days and then advanced 30 min until she was arising at 10 a.m. The subject continued the light treatment at home, and managed to live on a 24-h day for a 30day follow-up study.66 In blind people without photic input through the eyes (e.g., severe cataract), several studies show that exogenous melatonin is effective in entraining the circadian rhythm.67,68 To conclude, in sighted patients with a freerunning rhythm, bright light may be tried. One approach is to use a similar method as for delayed sleep phase disorder. That is, start bright light treatment after awakening, and then gradually advance the timing of the bright light from day to day, until entrainment. Then, continue with bright light, either intermittently, or if necessary, every day. A different approach is to start bright light treatment when the patient’s rhythm is in phase with the environment. In blind people (with no photic input) and in sighted people with unsatisfactory effect of bright light, try melatonin. Intake of melatonin (5e7 h before bedtime) may be started when the rhythm is phase aligned. A different approach is to start melatonin administration 12 h after the last awakening, and then advance the timing of intake from day to day until entrainment. However, more clinical studies are clearly warranted for this disorder. Irregular sleepewake rhythm Irregular sleepewake rhythm is characterized by lack of a clearly defined circadian rhythm of sleep and wake.3 Sleep and wake periods are variable in length throughout the 24-h day. Prevalence of this disorder is unknown. An irregular sleepewake rhythm is commonly associated with neurological impairment, i.e., dementia, and much of the research has focused on this patient population.2,45 It has also been found to be related to psychomotor retardation in children.2,69 Estimation of nadir in this disorder is difficult as no main sleep episode seems to be present. Instead a polycyclic sleepewake pattern occurs during the day. Irregular sleepewake rhythm is assumed partially to be caused by lack of stimuli, such as light, social activity and work, which normally entrain the circadian rhythm.2,45 Please cite this article in press as: Bjorvatn Bjø, Pallesen Stå, A practical approach to circadian rhythm sleep disorders, Sleep Medicine Reviews (2008), doi:10.1016/j.smrv.2008.04.009 ARTICLE IN PRESS Estimating circadian phase in every day clinical practice The aim of the treatment is to increase the amplitude of the circadian rhythm. Specifically, this has been done by introducing scheduled social and physical activities. In addition, exposure to morning bright light and administration of evening melatonin may also be effective in alleviating the symptoms.2,45 However, if the patient suffers from early morning awakening, bright light in the evening is more appropriate, and morning light should be avoided. The diagnosis of irregular sleepewake rhythm is problematic, since the diagnostic criteria of ICSD-2 specify that the disorder should not be better explained by a medical, neurological or mental disorder.3 Hence, in demented patients and in mentally retarded children making the diagnosis of a circadian rhythm sleep disorder is questionable. Jet lag disorder Case history Ann, a Norwegian 38-year-old scientist, is going to Baltimore, USA for a conference. She will be away for 10 days, and she usually adjusts her circadian rhythm without major problems on westbound travels. However, she usually experiences severe problems adjusting back to Norwegian time zone, when returning from such events. Often she complains of insomnia at night and sleepiness during the early day for up to 1 week or more following 6 h time zone changes. She wonders if there is anything to do with this jet lag. Jet lag disorder typically consists of insomnia and excessive daytime sleepiness associated with transmeridian jet travel. There is associated impairment of daytime function, general malaise and gastrointestinal disturbance.3 The symptoms occur because the endogenous circadian rhythm becomes misaligned to the external clock time. Following rapid travel, the endogenous circadian system remains aligned to the environmental time cues of the home time zone. Because the adjustment process of the circadian system is slow, averaging 60 min of phase adjustment per day after a phase advance shift (eastbound flight), and 90 min per day after a phase delay shift (westbound flight), symptoms can last for several days after the flight.70 However, the adjustment process can be modified. Eastbound flights are considered more problematic than westbound flights. One important reason is that for most people the endogenous period of the sleep/wakerhythm is slightly longer than 24 h,10 thus facilitating adaptation on westbound travels. 9 Treatment with bright light Adaptation to the new time zone can be accelerated by bright light treatment, applied according to the phase-response curve.71 Avoidance of light is also very important, as light exposure at the ‘‘wrong’’ circadian time can delay adaptation of the internal clock, or even facilitate adaptation in the wrong direction. This is also a reason why eastbound travels may be more problematic than westbound travels; light is often encountered at a ‘‘wrong’’ circadian time. For example, in our case history, Ann is travelling eastwards from Baltimore to Norway, a 6 h time zone change. If the nadir of her core body temperature rhythm in Baltimore is about 5 a.m., this will correspond to 11 a.m. Norwegian time. When she arrives at Norway in the morning, she may get exposed to bright light before her nadir, causing phase delays, thus hindering adaptation of the circadian rhythm. According to the phase-response curve, she should avoid light exposure (e.g., use dark sunglasses) prior to 11 a.m., and get bright light exposure after 11 a.m. Light after 11 a.m. will phase advance the rhythm. The timing of bright light is changed from day to day,72 similar to the method for delayed sleep phase disorder. In clinical practice, we often advance (or delay) the timing of light with up to 2 h per day. In Ann’s case, she was advised to avoid light before 9 a.m., and get exposed bright light after 9. a.m. the second day. The third day, Ann was advised to avoid light before 7 a.m. and get bright light exposure after 7 a.m. She will thus adjust her circadian rhythm within 2e3 days following a 6 h eastbound flight. Treatment with bright light can also be instituted prior to departure, if feasible and desirable. For eastbound travels, the treatment regime usually aims at adaptation of the circadian rhythm by phase advance. However, for eastbound travels over 10 h or more time zones, it may be easier to phase delay the circadian rhythm. This is partly due to the fact that for most people our internal clock is longer than 24 h. However, for morning larks this may not apply. For westbound travels over 6e9 time zones, natural light exposure on the ‘‘wrong’’ circadian phase is usually not a problem as it is for eastbound travels. Thus, when travelling west, subjects are advised to get as much outdoor light as possible during the daytime. This will facilitate adaptation of the rhythm. During night-time at the destination, bright light should be avoided. Treatment with melatonin Several studies have shown that melatonin may successfully be applied to reduce jet lag.73,74 In Please cite this article in press as: Bjorvatn Bjø, Pallesen Stå, A practical approach to circadian rhythm sleep disorders, Sleep Medicine Reviews (2008), doi:10.1016/j.smrv.2008.04.009 ARTICLE IN PRESS 10 clinical practice, best and fastest adaptation may occur by timing the treatment according to the individual PRC. In our case history, Ann was advised to take melatonin 12 h after bright light exposure, that is, at 11 p.m. on day 1. On day 2, melatonin was taken at 9 p.m., and at about 7e8 p.m. on day 3. A simpler recommendation is to administer melatonin every day between 10 and 12 p.m. at the new destination. This normally corresponds well to the ideal timing of melatonin according to the PRC.73 Combined melatonin and bright light treatment may facilitate adaptation of the circadian rhythm even faster than either treatment alone. However, scientific evidence is lacking. From a clinical standpoint, we advise such combination in people suffering from severe jet lag. Treatment for jet lag usually lasts only 3e4 days, at the most. Shift work disorder Case history Thomas (48 years) works 14 consecutive nights (7 p.m. to 7 a.m.) at an oil platform in the North Sea. He suffers from severe sleepiness the first nights, until his rhythm gradually adjusts. Similarly, following return home after this 14-night working period, he struggles with re-adaptation back to his normal day-oriented rhythm. He wonders if something can help him adapt more easily. Shift work, and night work in particular, is associated with negative effects, such as shortened and disturbed sleep, fatigue, decreased alertness, cognitive decrements, increased injuries and accidents, reproductive problems and risks to cardiovascular and gastrointestinal health.75,76 These symptoms are experienced because shift workers rarely shift their endogenous circadian rhythms to align with the sleepewake schedule demanded by their occupations. Night workers are therefore often in a constant state of circadian misalignment, and both work and sleep at the ‘‘wrong’’ circadian phase. The symptoms due to circadian misalignment can be reduced even if the optimal phase relationship is not completely established. The magnitude of phase shift is positively related to the extent of improved performance and alertness during the night, and better daytime sleep at home.77 Treatment with bright light Several studies have shown that timed bright light and darkness can promote adaptation to night work.76e80 In our case history, bright light timed B. Bjorvatn, S. Pallesen before nadir of the core body temperature rhythm will facilitate adaptation to night work. Nadir is estimated based on a clinical interview with Thomas. Thomas usually gets up at 7 a.m., and based on prior night work experience, he is especially sleepy at around 5 a.m. Hence, nadir of the core body temperature rhythm is likely to be at about 5 a.m. Thus, bright light is advised before his nadir (30 min, 10 000 lux). In addition, he is advised to avoid bright light after 5 a.m. on night 1. Night 2 he is advised to get bright light at 6 a.m., and avoid light after 7 a.m. Thomas will likely feel less sleepy during the night and sleep better during the day the moment nadir is ‘‘pushed’’ to after the work period. Usually 2e4 days of treatment may be sufficient for a night worker. Following the 14-night working period, Thomas will again be advised to get bright light exposure. Timing of treatment is more complicated following the work period, because nadir is difficult to estimate. In clinical practice, we advise that a thorough interview may give an indication of the nadir. Thomas experienced sleeping until about 5 p.m. towards the end of the 14-night working period. We may assume that nadir may be at about 3 p.m. Thus, in order to phase delay the circadian rhythm, bright light exposure was advised before 3 p.m. Usually, we ask the subjects to receive as much light as possible (natural or artificial light) before 3 p.m. Importantly, Thomas is advised to avoid bright light after 3 p.m., that is, use dark sunglasses or stay inside. The next day, he is advised to get exposed to bright light before 5 p.m., and avoid light after 5 p.m. Day 3: bright light exposure before 7 p.m., avoid after 7 p.m., and so on. In this case history, a phase delay was advised, also for the re-adaptation following the night work period. In other cases, a phase advance may be more appropriate, i.e., when the nadir of the core body temperature rhythm is earlier in the day. Individual treatment is advised, not only based on nadir estimations, but also on the worker’s circadian type (morning lark or evening owl). Evening owls adapt easier by phase delays, than by phase advances, due to their endogenous circadian rhythm. Treatment with melatonin Melatonin has also been shown to be efficient in alleviating the complaints associated with night work.77,80e82 However, most studies were done under simulated night work conditions. Similar to the other circadian rhythm sleep disorders, the timing of melatonin is important for the effect. And similarly, the timing of melatonin may be changed from day to day, in order to maximize the effect on the circadian rhythm. Please cite this article in press as: Bjorvatn Bjø, Pallesen Stå, A practical approach to circadian rhythm sleep disorders, Sleep Medicine Reviews (2008), doi:10.1016/j.smrv.2008.04.009 ARTICLE IN PRESS Estimating circadian phase in every day clinical practice Although both bright light and melatonin may be effective in alleviating the complaints during night work, it is questionable whether night workers on rapid rotating schedules (e.g., 2e3 consecutive nights) should aim at adapting their circadian rhythms. If adaptation is successful, re-adaptation back to day-oriented life is likely impeded. Treatment based on circadian principles is best applied to shift schedules lasting 1 week or longer. We have here focused on the treatment for realigning the circadian rhythm, but strategies to improve sleep (hypnotics) and alertness (caffeine, modafinil, scheduled naps) can also be used.45 Such treatment options are not discussed in this paper. Summary Bright light and melatonin can be used successfully in the treatment of circadian rhythm sleep disorders. However, appropriate timing of the treatments is crucial for the effect. An estimation of the patient’s circadian phase is therefore important before the treatment is started. In clinical practice, a careful patient history may give sufficient information in order to estimate the circadian phase. The nadir of the core body temperature rhythm is about 2 h before the habitual wake-up time. Bright light administered before the nadir of the core body temperature rhythm will phase delay, whereas bright light administered after the nadir will phase advance the rhythm. Similarly, the effect of melatonin is dependent on the timing of treatment. Melatonin in the late afternoon or evening will phase advance, whereas melatonin in the morning will phase delay the circadian rhythm. In clinical practice, bright light of about 10 000 lux is usually administered daily for 30e45 min. The dose of melatonin does not seem to be of great importance, and for most disorders we use 3 mg tablets. In order to maximize the effects of treatment, the timing of both bright light and melatonin is often changed from day to day. With such an approach, the treatments are administered at about the same time point in the phase-response curve from day to day. Importantly, if the treatment effects are not satisfactory, or if the patient’s condition actually worsens, you may have incorrectly estimated the circadian phase! Try to estimate once more, and adjust the timing of bright light/melatonin accordingly. This is the advantage in clinical practice (compared to a scientific protocol); it is always possible to adjust treatment. 11 In all patients, a differential diagnosis must always be considered. In order to diagnose a circadian rhythm sleep disorder, the criteria state that the sleep disturbance should not be better explained by another current sleep disorder, medical or neurological disorder, mental disorder, medication use, or substance use disorder. Practice points 1. Circadian phase can in many instances be estimated by careful patient history. 2. Nadir of the core body temperature rhythm is normally located at about 2 h before the habitual wake-up time, and corresponds to the time point where it is most difficult to stay awake. 3. The phase-response curve to melatonin is about 12 h out of phase with the phaseresponse curve to light. 4. Bright light exposure before the nadir induces phase delays, whereas bright light after the nadir induces phase advances. 5. Exogenous melatonin administration in the late afternoon or evening induces phase advances, whereas melatonin administered in the morning induces phase delays. 6. Circadian rhythm sleep disorders can effectively be treated by appropriately timed bright light and/or melatonin. 7. Do not start bright light treatment for delayed sleep phase disorder in the early morning, but wait until the patient wakes up in a natural way (without an alarm clock). Bright light is subsequently administered 1 h earlier per day until entrainment. 8. Appropriate timing of melatonin administration is about 12 h after bright light treatment. Research agenda 1. Scientific studies comparing the circadian phase measured objectively (by melatonin assays or core body temperature) and the circadian phase estimated by careful patient history should be carried out. Please cite this article in press as: Bjorvatn Bjø, Pallesen Stå, A practical approach to circadian rhythm sleep disorders, Sleep Medicine Reviews (2008), doi:10.1016/j.smrv.2008.04.009 ARTICLE IN PRESS 12 B. Bjorvatn, S. Pallesen 2. Studies examining the clinical effectiveness of bright light, melatonin and combined bright light/melatonin in circadian rhythm sleep disorders are needed. 3. Comparisons between the effects of bright light and melatonin in circadian rhythm sleep disorders. What treatment works best, and for whom? 4. Studies investigating long-term effectiveness of bright light and/or melatonin in circadian rhythm sleep disorders should be conducted. 5. Studies on how to implement treatment for circadian rhythm sleep disorders in general clinical practice are necessary. 6. Studies investigating different light intensities and different doses of melatonin in the treatment of circadian rhythm sleep disorders are warranted. 7. Studies investigating safety issues associated with long-term use of light and/or melatonin are needed. 9. 10. 11. 12. 13. 14. 15. 16. 17. References 18. *1. Sack RL, Auckley D, Auger RR, Carskadon MA, Wright Jr KP, Vitiello MV, et al. Circadian rhythm sleep disorders: part I, basic principles, shift work and jet lag disorders. An American Academy of Sleep Medicine review. Sleep 2007; 30(11):1460e83. *2. Sack RL, Auckley D, Auger RR, Carskadon MA, Wright Jr KP, Vitiello MV, et al. Circadian rhythm sleep disorders: part II, advanced sleep phase disorder, delayed sleep phase disorder, free-running disorder, and irregular sleepewake rhythm. An American Academy of Sleep Medicine review. Sleep 2007;30(11):1484e501. 3. American Academy of Sleep Medicine. International classification of sleep disorders: diagnostic and coding manual. 2nd ed. Westchester, IL: American Academy of Sleep Medicine; 2005. 4. Dijk DJ, Czeisler CA. Contribution of the circadian pacemaker and the sleep homeostat to sleep propensity, sleep structure, electroencephalographic slow waves, and sleep spindle activity in humans. J Neurosci 1995; 15(5 Pt 1):3526e38. 5. Dijk DJ, Brunner DP, Beersma DG, Borbely AA. Electroencephalogram power density and slow wave sleep as a function of prior waking and circadian phase. Sleep 1990;13(5): 430e40. 6. Akerstedt T. Shift work and disturbed sleep/wakefulness. Occup Med (Lond) 2003;53(2):89e94. 7. Brown EN, Czeisler CA. The statistical analysis of circadian phase and amplitude in constant-routine core-temperature data. J Biol Rhythms 1992;7(3):177e202. *8. Lewy AJ, Bauer VK, Ahmed S, Thomas KH, Cutler NL, Singer CM, et al. The human phase response curve (PRC) * The most important references are denoted by an asterisk. 19. 20. 21. 22. *23. *24. 25. 26. 27. to melatonin is about 12 hours out of phase with the PRC to light. Chronobiol Int 1998;15(1):71e83. Aschoff J. Circadian rhythms in man. Science 1965;148: 1427e32. Czeisler CA, Duffy JF, Shanahan TL, Brown EN, Mitchell JF, Rimmer DW, et al. Stability, precision, and near-24-hour period of the human circadian pacemaker. Science 1999; 284(5423):2177e81. Gillette MU, Tischkau SA. Suprachiasmatic nucleus: the brain’s circadian clock. Recent Prog Horm Res 1999;54: 33e58. discussion-9. Ralph MR, Foster RG, Davis FC, Menaker M. Transplanted suprachiasmatic nucleus determines circadian period. Science 1990;247(4945):975e8. Hattar S, Liao HW, Takao M, Berson DM, Yau KW. Melanopsin-containing retinal ganglion cells: architecture, projections, and intrinsic photosensitivity. Science 2002; 295(5557):1065e70. Borjigin J, Li X, Snyder SH. The pineal gland and melatonin: molecular and pharmacologic regulation. Annu Rev Pharmacol Toxicol 1999;39:53e65. Minors DS, Waterhouse JM. The use of constant routines in unmasking the endogenous component of human circadian rhythms. Chronobiol Int 1984;1(3):205e16. Pandi-Perumal SR, Smits M, Spence W, Srinivasan V, Cardinali DP, Lowe AD, et al. Dim light melatonin onset (DLMO): a tool for the analysis of circadian phase in human sleep and chronobiological disorders. Prog Neuropsychopharmacol Biol Psychiatry 2007;31(1):1e11. Lewy AJ, Cutler NL, Sack RL. The endogenous melatonin profile as a marker for circadian phase position. J Biol Rhythms 1999;14(3):227e36. Nagtegaal JE, Kerkhof GA, Smits MG, Swart AC, Van Der Meer YG. Delayed sleep phase syndrome: a placebocontrolled cross-over study on the effects of melatonin administered five hours before the individual dim light melatonin onset. J Sleep Res 1998;7(2):135e43. Voultsios A, Kennaway DJ, Dawson D. Salivary melatonin as a circadian phase marker: validation and comparison to plasma melatonin. J Biol Rhythms 1997;12(5):457e66. Wright H, Lack L, Bootzin R. Relationships between dim light melatonin onset and the timing of sleep in sleep onset insomniacs. Sleep Biol Rhythms 2006;4:78e80. Burgess HJ, Eastman CI. The dim light melatonin onset following fixed and free sleep schedules. J Sleep Res 2005;14(3):229e37. Benloucif S, Guico MJ, Reid KJ, Wolfe LF, L’HermiteBaleriaux M, Zee PC. Stability of melatonin and temperature as circadian phase markers and their relation to sleep times in humans. J Biol Rhythms 2005;20(2):178e88. Dijk DJ, Boulos Z, Eastman CI, Lewy AJ, Campbell SS, Terman M. Light treatment for sleep disorders: consensus report. II. Basic properties of circadian physiology and sleep regulation. J Biol Rhythms 1995;10(2):113e25. Khalsa SB, Jewett ME, Cajochen C, Czeisler CA. A phase response curve to single bright light pulses in human subjects. J Physiol 2003;549(Pt 3):945e52. Minors DS, Waterhouse JM, Wirz-Justice A. A human phaseresponse curve to light. Neurosci Lett 1991;133(1):36e40. Zeitzer JM, Dijk DJ, Kronauer R, Brown E, Czeisler C. Sensitivity of the human circadian pacemaker to nocturnal light: melatonin phase resetting and suppression. J Physiol 2000; 526(Pt 3):695e702. Czeisler CA, Kronauer RE, Allan JS, Duffy JF, Jewett ME, Brown EN, et al. Bright light induction of strong (type 0) resetting of the human circadian pacemaker. Science 1989;244(4910):1328e33. Please cite this article in press as: Bjorvatn Bjø, Pallesen Stå, A practical approach to circadian rhythm sleep disorders, Sleep Medicine Reviews (2008), doi:10.1016/j.smrv.2008.04.009 ARTICLE IN PRESS Estimating circadian phase in every day clinical practice 28. Jewett ME, Kronauer RE, Czeisler CA. Phase-amplitude resetting of the human circadian pacemaker via bright light: a further analysis. J Biol Rhythms 1994;9(3e4): 295e314. 29. Terman M, Terman JS. Light therapy. In: Kryger MH, Roth T, Dement WC, editors. Principles and practice of sleep medicine. 3rd ed. Elsevier Saunders; 2000. p. 1258e74. 30. Reme CE, Terman M. Does light therapy present an ocular hazard? Am J Psychiatry 1992;149(12):1762e3. 31. Gallin PF, Terman M, Reme CE, Rafferty B, Terman JS, Burde RM. Ophthalmologic examination of patients with seasonal affective disorder, before and after bright light therapy. Am J Ophthalmol 1995;119(2):202e10. 32. Pallesen S, Nordhus IH, Skelton SH, Bjorvatn B, Skjerve A. Bright light treatment has limited effect in subjects over 55 years with mild early morning awakening. Percept Mot Skills 2005;101(3):759e70. 33. Kogan AO, Guilford PM. Side effects of short-term 10,000lux light therapy. Am J Psychiatry 1998;155(2):293e4. 34. Chan PK, Lam RW, Perry KF. Mania precipitated by light therapy for patients with SAD. J Clin Psychiatry 1994; 55(10):454. 35. Schwitzer J, Neudorfer C, Blecha HG, Fleischhacker WW. Mania as a side effect of phototherapy. Biol Psychiatry 1990;28(6):532e4. *36. Arendt J, Skene DJ. Melatonin as a chronobiotic. Sleep Med Rev 2005;9(1):25e39. 37. Lewy AJ, Sack RL. The role of melatonin and light in the human circadian system. Prog Brain Res 1996;111:205e16. 38. Buscemi N, Vandermeer B, Hooton N, Pandya R, Tjosvold L, Hartling L, et al. Efficacy and safety of exogenous melatonin for secondary sleep disorders and sleep disorders accompanying sleep restriction: meta-analysis. BMJ 2006; 332(7538):385e93. 39. Dagan Y, Eisenstein M. Circadian rhythm sleep disorders: toward a more precise definition and diagnosis. Chronobiol Int 1999;16(2):213e22. 40. Campbell SS, Murphy PJ. Delayed sleep phase disorder in temporal isolation. Sleep 2007;30(9):1225e8. *41. Dagan Y. Circadian rhythm sleep disorders (CRSD). Sleep Med Rev 2002;6(1):45e54. 42. Yazaki M, Shirakawa S, Okawa M, Takahashi K. Demography of sleep disturbances associated with circadian rhythm disorders in Japan. Psychiatry Clin Neurosci 1999;53(2): 267e8. 43. Schrader H, Bovim G, Sand T. The prevalence of delayed and advanced sleep phase syndromes. J Sleep Res 1993; 2(1):51e5. 44. Pelayo RP, Thorpy MJ, Glovinsky P. Prevalence of delayed sleep phase syndrome among adolescents. Sleep Res 1988;17:392. 45. Barion A, Zee PC. A clinical approach to circadian rhythm sleep disorders. Sleep Med 2007;8(6):566e77. 46. Crowley SJ, Acebo C, Carskadon MA. Sleep, circadian rhythms, and delayed phase in adolescence. Sleep Med 2007;8(6):602e12. 47. Regestein QR, Monk TH. Delayed sleep phase syndrome: a review of its clinical aspects. Am J Psychiatry 1995; 152(4):602e8. 48. Ozaki S, Uchiyama M, Shirakawa S, Okawa M. Prolonged interval from body temperature nadir to sleep offset in patients with delayed sleep phase syndrome. Sleep 1996; 19(1):36e40. 49. Archer SN, Robilliard DL, Skene DJ, Smits M, Williams A, Arendt J, et al. A length polymorphism in the circadian clock gene Per3 is linked to delayed sleep phase syndrome and extreme diurnal preference. Sleep 2003;26(4):413e5. 13 50. Ferrara M, De Gennaro L. How much sleep do we need? Sleep Med Rev 2001;5(2):155e79. 51. Carskadon MA, Vieira C, Acebo C. Association between puberty and delayed phase preference. Sleep 1993;16(3): 258e62. 52. Carskadon MA, Harvey K, Duke P, Anders TF, Litt IF, Dement WC. Pubertal changes in daytime sleepiness. Sleep 1980;2(4):453e60. 53. Rosenthal NE, Joseph-Vanderpool JR, Levendosky AA, Johnston SH, Allen R, Kelly KA, et al. Phase-shifting effects of bright morning light as treatment for delayed sleep phase syndrome. Sleep 1990;13(4):354e61. 54. Okawa M, Uchiyama M, Ozaki S, Shibui K, Ichikawa H. Circadian rhythm sleep disorders in adolescents: clinical trials of combined treatments based on chronobiology. Psychiatry Clin Neurosci 1998;52(5):483e90. 55. Mundey K, Benloucif S, Harsanyi K, Dubocovich ML, Zee PC. Phase-dependent treatment of delayed sleep phase syndrome with melatonin. Sleep 2005;28(10):1271e8. *56. Kayumov L, Brown G, Jindal R, Buttoo K, Shapiro CM. A randomized, double-blind, placebo-controlled crossover study of the effect of exogenous melatonin on delayed sleep phase syndrome. Psychosom Med 2001;63(1):40e8. 57. Baker SK, Zee PC. Circadian disorders of the sleepewake cycle. In: Kryger MH, Roth T, Dement WC, editors. Principles and practice of sleep medicine. 3rd ed. Philadelphia: W.B. Saunders; 2000. p. 606e14. *58. Revell VL, Burgess HJ, Gazda CJ, Smith MR, Fogg LF, Eastman CI. Advancing human circadian rhythms with afternoon melatonin and morning intermittent bright light. J Clin Endocrinol Metab 2006;91(1):54e9. 59. Satoh K, Mishima K, Inoue Y, Ebisawa T, Shimizu T. Two pedigrees of familial advanced sleep phase syndrome in Japan. Sleep 2003;26(4):416e7. 60. Toh KL, Jones CR, He Y, Eide EJ, Hinz WA, Virshup DM, et al. An hPer2 phosphorylation site mutation in familial advanced sleep phase syndrome. Science 2001;291(5506): 1040e3. 61. Pallesen S, Nordhus IH, Nielsen GH, Havik OE, Kvale G, Johnsen BH, et al. Prevalence of insomnia in the adult Norwegian population. Sleep 2001;24(7):771e9. 62. Campbell SS, Murphy PJ, van den Heuvel CJ, Roberts ML, Stauble TN. Etiology and treatment of intrinsic circadian rhythm sleep disorders. Sleep Med Rev 1999;3(3):179e200. 63. Campbell SS, Dawson D, Anderson MW. Alleviation of sleep maintenance insomnia with timed exposure to bright light. J Am Geriatr Soc 1993;41(8):829e36. 64. Palmer CR, Kripke DF, Savage Jr HC, Cindrich LA, Loving RT, Elliott JA. Efficacy of enhanced evening light for advanced sleep phase syndrome. Behav Sleep Med 2003;1(4): 213e26. 65. Suhner AG, Murphy PJ, Campbell SS. Failure of timed bright light exposure to alleviate age-related sleep maintenance insomnia. J Am Geriatr Soc 2002;50(4):617e23. 66. Hoban TM, Sack RL, Lewy AJ, Miller LS, Singer CM. Entrainment of a free-running human with bright light? Chronobiol Int 1989;6(4):347e53. 67. Sack RL, Brandes RW, Kendall AR, Lewy AJ. Entrainment of free-running circadian rhythms by melatonin in blind people. N Engl J Med 2000;343(15):1070e7. 68. Lewy AJ, Bauer VK, Hasler BP, Kendall AR, Pires ML, Sack RL. Capturing the circadian rhythms of free-running blind people with 0.5 mg melatonin. Brain Res 2001; 918(1e2):96e100. 69. Pillar G, Shahar E, Peled N, Ravid S, Lavie P, Etzioni A. Melatonin improves sleepewake patterns in psychomotor retarded children. Pediatr Neurol 2000;23(3):225e8. Please cite this article in press as: Bjorvatn Bjø, Pallesen Stå, A practical approach to circadian rhythm sleep disorders, Sleep Medicine Reviews (2008), doi:10.1016/j.smrv.2008.04.009 ARTICLE IN PRESS 14 B. Bjorvatn, S. Pallesen 70. Boulos Z, Campbell SS, Lewy AJ, Terman M, Dijk DJ, Eastman CI. Light treatment for sleep disorders: consensus report. VII. Jet lag. J Biol Rhythms 1995; 10(2):167e76. 71. Burgess HJ, Crowley SJ, Gazda CJ, Fogg LF, Eastman CI. Preflight adjustment to eastward travel: 3 days of advancing sleep with and without morning bright light. J Biol Rhythms 2003;18(4):318e28. 72. Haimov I, Arendt J. The prevention and treatment of jet lag. Sleep Med Rev 1999;3(3):229e40. 73. Herxheimer A, Petrie KJ. Melatonin for the prevention and treatment of jet lag. Cochrane Database Syst Rev 2006; (Disk issue 2):CD00484. 74. Suhner A, Schlagenhauf P, Johnson R, Tschopp A, Steffen R. Comparative study to determine the optimal melatonin dosage form for the alleviation of jet lag. Chronobiol Int 1998;15(6):655e66. 75. Akerstedt T. Psychological and psychophysiological effects of shift work. Scand J Work Environ Health 1990; 16(Suppl. 1):67e73. *76. Boivin DB, Tremblay GM, James FO. Working on atypical schedules. Sleep Med 2007;8(6):578e89. 77. Burgess HJ, Sharkey KM, Eastman CI. Bright light, dark and melatonin can promote circadian adaptation in night shift workers. Sleep Med Rev 2002;6(5):407e20. 78. Czeisler CA, Johnson MP, Duffy JF, Brown EN, Ronda JM, Kronauer RE. Exposure to bright light and darkness to treat physiologic maladaptation to night work. N Engl J Med 1990;322(18):1253e9. 79. Bjorvatn B, Kecklund G, Akerstedt T. Bright light treatment used for adaptation to night work and re-adaptation back to day life. A field study at an oil platform in the North Sea. J Sleep Res 1999;8(2):105e12. 80. Bjorvatn B, Stangenes K, Oyane N, Forberg K, Lowden A, Holsten F, et al. Randomized placebo-controlled field study of the effects of bright light and melatonin in adaptation to night work. Scand J Work Environ Health 2007; 33(3):204e14. 81. Dawson D, Encel N, Lushington K. Improving adaptation to simulated night shift: timed exposure to bright light versus daytime melatonin administration. Sleep 1995;18(1):11e21. 82. Sharkey KM, Fogg LF, Eastman CI. Effects of melatonin administration on daytime sleep after simulated night shift work. J Sleep Res 2001;10(3):181e92. Available online at www.sciencedirect.com Please cite this article in press as: Bjorvatn Bjø, Pallesen Stå, A practical approach to circadian rhythm sleep disorders, Sleep Medicine Reviews (2008), doi:10.1016/j.smrv.2008.04.009