Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
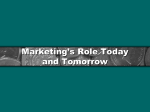
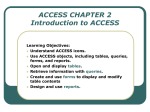
SPECIAL CONTRIBUTION Emergency Medicine Can Play a Leadership Role in Enterprise-wide Clinical Information Systems From the Department of Emergency Medicine, Washington Hospital Center, and the National Center for Emergency Medicine Informatics, Washington, DC*; Department of Emergency Medicine, Northwestern University School of Medicine, Chicago, IL‡; and the Department of Emergency Medicine, Prince George’s Hospital Center, Cheverly, MD.§ Received for publication November 9, 1998. Revision received July 12, 1999. Accepted for publication September 10, 1999. Reprints not available from the authors. Address for correspondence: Craig F. Feied, MD, Washington Hospital Center, Department of Emergency Medicine, 110 Irving Street NW, Washington, DC 20010; 202-8777574, fax 202-877-2468; E-mail [email protected]. Copyright © 2000 by the American College of Emergency Physicians. Craig F. Feied, MD* Mark S. Smith, MD* Jonathan A. Handler, MD‡ Meera Kanhouwa, MD§ At many institutions, the department of emergency medicine is uniquely suited to a leadership role in the deployment of new clinical decision support systems (computer systems that support clinical practice). Many factors favor such a leadership role, including institutional politics, organizational structure, extent of local control, clinician solidarity, openness to change, departmental size and scale, and willingness to take risks. Such a role should be undertaken in partnership with the institution’s information services (IS) department, and a clear understanding of goals and responsibilities will facilitate such a partnership. A leadership position with respect to new information systems entails a certain risk, but the potential benefit to an emergency department in today’s competitive environment is substantial. The authors’ experience with one such collaborative development project is presented. [Feied CF, Smith MS, Handler JA, Kanhouwa M. Emergency medicine can play a leadership role in enterprise-wide clinical information systems. Ann Emerg Med. February 2000;35:162167.] 0196-0644/2000/$12.00 + 0 47/1/103131 INTRODUCTION One of the most important transformations that will occur in medicine over the next 10 years is the application of new information technologies to clinical practice. We believe that at many institutions, the department of emergency medicine is in a unique position to assume a leadership position in this transformation through a partnership with the institution’s information services (IS) department. A revolution in the applications of new information technology is currently under way in medicine. As clinicians become more computer-savvy, health care enterprise IS departments struggle to meet the new needs of demanding clinical users at the same time that they strug- 1 6 2 ANNALS OF EMERGENCY MEDICINE 35:2 FEBRUARY 2000 ENTERPRISE-WIDE CLINICAL INFORMATION SYSTEMS Feied et al gle to shore up monolithic legacy mainframe systems. The highly publicized “year 2000 bug” is only one in a long list of perennial problems that threaten traditional billing, laboratory, and financial services systems. These missioncritical systems must be kept operational in an increasingly alien and rapidly changing modern computer systems environment. Because of the funds invested in these legacy systems, they cannot be easily abandoned. Yet clinical users are increasingly dissatisfied with traditional mainframe interfaces that require extended effort to deliver small aliquots of information about a single patient. Although integrated clinical information systems are highly desired by clinicians, most clinical departments will continue to work with manual systems until they can become passive end users of a generic enterprise-wide system. Unfortunately, today’s commercially available enterprise-level clinical information systems are designed with a “patient-centric” and “problem-centric” approach in which current and historical information is displayed about a single patient with well-characterized clinical problems that are followed over a prolonged period. These longitudinally organized, single-patient–focused, problem-oriented data systems are ill-suited to the needs of emergency departments, where episodic care is delivered simultaneously to many critically ill patients whose conditions are not yet diagnosed. Increased competition and declining reimbursement have made the need for more and better information critical to EDs.1 If integrated hospital-wide systems cannot immediately meet the information needs of EDs, many such departments will be forced to operate with standalone emergency medicine computer systems that are separate from the hospital system. Although this can be an effective short-term solution, such systems cannot persist for long. In the information age, connectivity is king and stand-alone clinical systems are at best a bridging technology, if not an anachronism. Systems that do not fully participate in standards-based connectivity and exchange of information will be abandoned as testaments to the shortsightedness of their developers and their purchasers. Collaboration between the ED and IS department in a joint implementation of solutions based on accepted standards makes sense for both parties. Much of the data needed by the ED to serve its patients already exist in the stewardship of others. To have access to those data, computer systems used by the ED should link to a variety of disparate legacy systems. The IS department can provide those critical links to many sources of real-time and his- FEBRUARY 2000 35:2 ANNALS OF EMERGENCY MEDICINE torical data throughout the institution, as well as a pathway by which to reintegrate new information and data generated within the ED. Conversely, the IS department of a health care delivery system often is in great need of a clinical partner, one who is engaged in delivering the actual service that the health care organization was created to provide (ie, clinical care). In many institutions, the IS department is pressured to demonstrate clinical utility and to satisfy a demanding medical staff accustomed to modern Internet interfaces. In a hospital where essential services depend on legacy mainframe systems in which a huge investment already has been made, this is not an easy task. More than 50 years ago, George Pólya, a brilliant Hungarian mathematician, set forth guidelines for tackling difficult mathematical problems.2 For the most difficult classes of problems, he proposed first trying to solve a simpler problem derived by changing the scale of the problem or by dropping 1 or more constraints.3 This principle is also applicable outside mathematics.3 The general health care enterprise clinical information systems problem is very complex, and may be more easily approached by first solving it in the simplified environment of the ED. From a clinical information point of view, the ED is a much simpler system than the entire enterprise. Fewer people are involved in its operation, the area is geographically compact, most patient visits are of short duration, and most diagnostic tests are performed only once per visit. The ED is essentially a self-contained miniature health care delivery system in terms of the processes of care and categories of information that exist within its departmental walls. The menu and complexity of ED processes reflect those of the clinical operation of the whole clinical enterprise—patients are registered, insurance information is collected, clinical care is rendered, laboratory, radiology and other diagnostic tests are ordered and completed, results are returned in real time, diagnoses are assigned, disposition is made, and billing is performed. With the implementation of intensive diagnosis and treatment units in many EDs and the growth of observation medicine, selected ED patients may have an entire 48-hour hospital admission compressed into an intensive 12-hour stay. Patients who are admitted as inpatients may go to virtually any hospital area, and those who are discharged or transferred may go to almost any receiving facility. While physicians and nurses play a central role in the ED, housekeeping, dietary services, materials management, engineering, plant maintenance, and other personnel also are involved. From a practical point of view, EDs have 1 6 3 ENTERPRISE-WIDE CLINICAL INFORMATION SYSTEMS Feied et al more political autonomy, smaller and more centralized leadership and administration, and more unanimity of purpose among clinicians than many other departments. Issues that can require months or years of political wrangling in other departments can be decided more quickly in an ED. Simplicity of scale in the ED also applies to the physical installation of a clinical information system. Fewer than 40 computer terminals on a single network segment in a very small area of the hospital can supply all of the clinical information needs of a typical ED serving 50,000 patients a year, whereas more than 10 times as many terminals may be needed when the same number of patients are distributed throughout the rest of the hospital. A protected environment in the ED is an added bonus during the vulnerable period of early development and initial installation of a clinical information system. Because of the closed team structure of the ED, awareness of the inevitable deployment problems and pains can be confined to a small number of people. And after successful deployment, no site in the hospital can be made more visible to more members of the medical staff from more specialties. A successful system in the ED is an immediate high-visibility win for IS. Because the ED is a scale model of the totality of a health care enterprise’s administrative, financial, and clinical processes of care, it is a natural “best choice” as the primary site for the introduction and testing of new information technology that can later be generalized to meet the needs of the rest of the enterprise. It would be difficult to find or design a better small-scale test site for the introduction of information technology innovations. A systems solution that works in the ED usually is readily scalable to an entire hospital or health care system. For example, in most hospitals the total patient volume of the ED is of the same order of magnitude as the total number of inpatient admissions. Scaling is further facilitated because in most hospitals, 25% to 50% of all inpatients are admitted through the ED. (There are approximately 90 million ED visits in the United States annually, and approximately 30 million hospital admissions. Roughly 12 million ED visits result in admission each year. Thus ED admissions account for about 40% of all hospital admissions.4-6) To make such a partnership work is not always easy. It will be necessary for both parties to adapt to new ways and to make compromises based on poorly understood needs that must be taken on faith. Leaders of the IS department should accept their natural role as guardians and providers of “clinically owned clinical data” rather 1 6 4 than as owners of those data. Their self-perceived role must be to ensure that all available data can be made available to the authorized clinical user through secure, authenticated connections using industry-standard hardware and software protocols. They should accept the need for different end user tools that query the same data sets to meet the needs of different clinical users. They should accept the deployment of dedicated technical resource personnel whose appointments are entirely within the clinical departments they serve. They will be required to accept a pace of change that is faster than may be comfortable. Leaders of the ED should recognize that an investment in information technology has the potential to do more to improve clinical care in the next 10 years than any other advance in the field of medicine. The clinical department must be prepared to accept the financial and administrative costs of technical personnel whose appointments are entirely within the clinical department. These personnel will need to understand the needs of the clinician, as well as the technical requirements and constraints of the information system. The administrative structure should permit change to be introduced into the department on a trial basis rapidly and in a nearly ad hoc manner without the need for layers of approval. Because of the rapidly changing and unproven nature of the field, both parties should have an a priori willingness to accept failure or serious delays in up to 20% of the leading-edge projects and project components that are undertaken. Both will need to trust that the other party is dealing in good faith, with an equal need for success in the project. Both will need to eschew and condemn efforts to divide the partners, and publicly and privately promote the fact and the perception that successful informatics projects in the ED result from a joint effort between the 2 departments. Neither IS nor the clinical department will be accustomed to technical people posted in (and paid by) a clinical department. Yet these clinically savvy technical personnel will be the key to the success of the entire operation. They will be responsible for the expression of the clinical information system within the clinical department. They will work closely with IS staff to establish and maintain standards-based departmental access to enterprise-wide clinical data sets. They will provide a buffer for IS technical staff by bearing the burden of the “typical unreasonable demands” of clinicians who do not fully appreciate the constraints of computer systems project schedules. They will provide a buffer for clinicians by bearing the burden of the “typical unreasonable refusals” ANNALS OF EMERGENCY MEDICINE 35:2 FEBRUARY 2000 ENTERPRISE-WIDE CLINICAL INFORMATION SYSTEMS Feied et al of purely technical staff who do not fully appreciate the clinical importance of features and timetables that consume precious resources. To illustrate the deployment of these concepts, we briefly describe the information flow strategy at one health care institution. Washington Hospital Center is the largest hospital in the Washington, DC, metropolitan region, and the largest single component of MedStar Health, a not-for-profit health care delivery system with approximately $1.4 billion in annual gross revenues. During 1996, a general purpose clinical information system (Active Query) was developed by the department of emergency medicine in partnership with the IS department of the enterprise. Since 1996, this system has been refined, expanded, and exported to meet the needs of clinical and administrative users beyond the walls of the ED. It has recently been deployed in a second MedStar Health hospital (Franklin Hospital Center, Baltimore, MD) and has become a model for systems development and deployment in the institution. From the start, responsibility for the project was divided along clear lines. The IS department is responsible for the acquisition and transport of clinical data from a variety of legacy systems and for the delivery of the data to the ED. The ED is responsible for the receipt, parsing, storage, retrieval, and presentation of the data that have been delivered. In practice, legacy data are received by IS through a number of proprietary interfaces in a variety of proprietary formats, and are then converted to the industry-standard health level 7 (HL7) medical data interchange format or are wrapped in HL7 wrappers. The HL7-compliant data are then passed from IS through a “sending” interface engine (a system used to translate data formats and to manage the process of sending and receiving data transactions across a network) over a standard Ethernet (IEEE 802.3) network to a “receiving” interface engine belonging to the department of emergency medicine. Transactions are passed from legacy system to sender to receiver in near–real time; laboratory results and radiology images appear at the ED interface engine within a few seconds after they are generated by laboratory equipment. The dividing line between IS and the ED is the link between the 2 interface engines, as these 2 devices regulate the flow of data between the 2 parties according to a series of standard and well-documented protocols (Figure 1). After being received from IS, data are handled by a series of software modules in a system that receives, parses, and stores each item. The architecture of this system is highly modular and fully object-oriented at every level, and uses a multitier transaction model in which the native data reside in an industry-standard structured query language (SQL) server, while rules governing the interpretation and presentation of the data are managed separately. Most clinicians and managers work with the data using a powerful custom-built Active Query client Figure 1. The IS department has responsibility for legacy systems and the IS interface engine. The ED has responsibility for all other data and hardware and software systems. SMS, Shared Medical Systems; MARS (radiology software application manufactured by Adac Systems); TCP/IP, Transmission control protocol/Internet protocol; NCEMI, National Center for Emergency Medicine Informatics. FEBRUARY 2000 35:2 ANNALS OF EMERGENCY MEDICINE 1 6 5 ENTERPRISE-WIDE CLINICAL INFORMATION SYSTEMS Feied et al that can load and run itself inside any modern Web browser using active-x or Java technology, but access to the data is possible using any tool or program that can form an SQL query (Figure 2). Commonly used tools that can easily be given access to the database include Microsoft Excel, Lotus 1-2-3, Microsoft Access, and Crystal Reports. The Active Query client offers an optimized interface that can handle the large majority of clinical and administrative information needs and is preferred by nearly all users. To meet the clinical needs of emergency physicians, the Active Query client was designed to display information for a cohort of patients all at one time, such as all patients currently in the ED, all patients belonging to a particular physician, or all patients admitted within the past year with a diagnosis of tuberculosis. By clicking on “filter” and “sort” options, in 30 seconds or less any clinician can answer an ad hoc question such as, “How many patients did I see last year with elevated cardiac enzymes, and which of them received a fibrinolytic agent in the emergency department?” Because of the power of such a cohort-oriented display, a more limited (Web-based) single-patient lookup system also has been deployed for use in areas where full-system access is considered too risky. The system is able to support a variety of strong and weak security schemata, ranging from login passwords (for access from “secure” clinical sites such as the clinical ED) to biometric authentication using fingerprint recognition or iris scanning technology (for access to the cohort-oriented display from unsecured or remote sites). Before 1996, Washington Hospital Center did not maintain any long-term storage of clinical data, with the exception of radiographic interpretations, which were stored in a proprietary radiology system. At deployment, the ED Active Query system became the institution’s only comprehensive source of historical clinical data. This data resource now includes detailed laboratory results, radiology results, radiographic images, historical diagnoses, procedures, medications, clinical photographs, scanned paper charts, financial account information, and a number of other types of clinical and administrative information. Because it provided rapid, intuitively easy access to a variety of information that was otherwise hard to find, the system quickly became indispensable to the clinical, administrative, and research functions of the ED. Although initially limited to ED patients, the system now receives and can display information on all inpatients and outpatients at Washington Hospital Center and has been adopted for use in a number of areas outside that institution’s ED. In addition to being fully deployed in the ED at a second hospital in the MedStar Health group, the Active Query system also has been targeted for spot deployment to meet critical information needs in selected areas at several other hospitals in the group. In this collaboration, a clinical department had wellrecognized specific information needs and the resources and ability to develop and deploy a clinical information system within the department in a very short time frame (13 months). The IS department had control of the flow of data from legacy systems, and the ability to translate and Figure 2. After the data are received by the ED interface engine, they are parsed and stored in an open, industry-standard database. Off-the-shelf and custom-built client software uses the data as needed for clinical decision support, departmental management, teaching, and research. Hct, Hematocrit; ODBC, open database connectivity. 1 6 6 ANNALS OF EMERGENCY MEDICINE 35:2 FEBRUARY 2000 ENTERPRISE-WIDE CLINICAL INFORMATION SYSTEMS Feied et al repackage those data to deliver them in an industry-standard format according to standard protocols. The collaboration produced a highly successful outcome that has improved clinical care both inside and outside the ED and has become a highly visible success with benefits for both departments. Emergency physicians regularly make split-second life-or-death decisions and take decisive action on the basis of incomplete information. Culture clash can make it frustrating to work with a department such as IS that depends on lengthy, detailed project planning. The problem is compounded by the reality that new information systems development must always take a “back seat” to the support of mission-critical legacy systems. Nonetheless, EDs will find many tangible benefits that outweigh the inherent frustrations of this collaboration. When the specific benefits of new information technologies accrue first to the ED, the department gains a competitive advantage over other departments in the hospital, because accurate financial and clinical analyses lead to a stronger showing in the competition for scarce institutional resources. With better information, the ED can enhance its operations to obtain a competitive advantage over other EDs in the region. Perhaps equally importantly, the ED’s long-term leadership role in the enterprise can be enhanced through a successful partnership with the IS department to pursue what will be recognized as one of the most important future directions of the entire enterprise. Over the past quarter century, emergency medicine has gained expertise and skills that can be of great value to the changing health care system. EDs are well positioned to serve as test beds for enterprise-wide clinical information systems because they are important care delivery nodes in the overall system, because they are to a great degree selfcontained in their clinical and ancillary operations, and because they are at the crossroads of information flow in the enterprise. A successful test project will require a partnership with IS departments and a commitment to use ED talent and resources to help improve clinical information management beyond the walls of the ED. At this pivotal time in the reformation of health care, emergency medicine has a singular and wonderful opportunity to assume a leadership role in the development and deployment of enterprise-wide clinical information systems. 2. Polya G. How to Solve It. 1st ed. Princeton, NJ: Princeton University Press; 1945. 3. Adams JL. Conceptual Blockbusting. 1st ed. San Francisco, CA: WH Freeman; 1974. 4. Kleinman JC, Tanner MM, Soodalter DL, et al. Planning for emergency medical services in Boston. Public Health Rep. 1975;90:460-466. 5. Graves EJ, Kozak LJ: National hospital discharge survey: annual summary, 1996. Vital Health Stat 13. 1998;134:1-46. 6. Nourjah P. National hospital ambulatory medical care survey: 1997 emergency department summary. National Center for Health Statistics. Advance data from vital health statistics; No 304. Hyattsville, MD: National Center for Health Statistics, 1999. REFERENCES 1. Cordell WH, Overhage JM, Waeckerle JF, et al. Strategies for improving information management in emergency medicine to meet clinical, research, and administrative needs. Ann Emerg Med. 1998;31:172-178. FEBRUARY 2000 35:2 ANNALS OF EMERGENCY MEDICINE 1 6 7