Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Reuse of excreta wikipedia , lookup
Human microbiota wikipedia , lookup
Ulcerative colitis wikipedia , lookup
Gastric bypass surgery wikipedia , lookup
Rectal prolapse wikipedia , lookup
Mariko Aoki phenomenon wikipedia , lookup
Colorectal cancer wikipedia , lookup
Intestine transplantation wikipedia , lookup
Colonoscopy wikipedia , lookup
Fecal incontinence wikipedia , lookup
Surgical management of fecal incontinence wikipedia , lookup
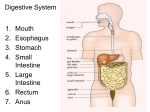
Title: The Large Intestine Introduction – In the large intestine churning and peristalsis drive the chyme toward the rectum, and the final secretion and absorption of nutrients and water occurs A- Anatomy of the large Intestine 1- The large intestine is about 5 feet long and 2.5 inches in diameter. It extends from the ileocecal sphincter to the anus 2- The large intestine is divided structurally into 4 major sections: The cecum, colon, rectum and anus. 3- Hanging inferiorly to the ileocecal sphincter is the cecum. The cecum is a small pouch from which the verifirm appendix (appendix) is connected. 4- The colon is further subdivided into four sections: The ascending colon, transverse colon, descending colon and the sigmoid flexure. a- The ascending colon abruptly turns right at the hepatic flexure (liver). The transverse colon turns inferiorly at the splenic flexure (spleen). The sigmoid colon is S-shaped which starts at the end of the transverse colon and ends at the rectum. The final 1 inch of the rectum is called the anus. b- The anus is protected by the internal anal sphincter (involuntary) and the external anal sphincter (voluntary) both are kept closed except during the elimination of feces. 5- Diagram – B- Histology of the Large Intestine 1- Compared to the small intestine the large has much fewer structural adaptations. There are no folds or villi. Microvilli are present on absorptive cells. Hence much more absorption occurs in the small intestine 2- 3 large thickened bands called the Tenie coli are present on the major portions of the intestine. Contractions of these muscles form the characteristic pouches of the large intestine giving it a puckered appearance. These pouches are called haustra 3- Coming off the tenia coli are little pouches of fat called epiploic appendages. There function is not known. C- Mechanical Digestion 1- Movement of chyme from the ileum into the cecum is controlled ilieocecal sphincter. Right after eating the gastroilial reflex intensifies, the hormone gastrin loosens the sphincter and chyme is forced into sphincter. 2- Haustral churning – The haustra remain relaxed until full and then they push there contents into the next haustra and so on until they are all full. 312 contractions per minute 3- Mass peristalsis – This is a strong peristaltic wave which occurs when chyme reaches about the middle of the transverse colon. This wave rapidly pushes chyme into the rectum. This gastrocolonic reflex usually occurs 34 times a day. D- Chemical Digestion 1- Final digestion in the large intestine occurs due to the bacteria present in the large intestine. These bacteria ferment any remaining CHO’s into carbon dioxide, hydrogen and methane gas. Thes contribute to flatus or gas in the colon. 2- Bilirubin is broken down into stercobilin 3- Vitamin K produced by the bacteria is absorbed into the blood. E- Feces Formation 1- Cyme usually remains in the large intestine for about 3 – 10 hours where it becomes solid or semi-solid depending on the amount of water absorption. It is now called feces 2- Feces consists of inorganic salts, epithelial cells, bacteria, unabsorbed digested materials and indigestible parts of food. 3- Of the 0.5 – 1.0 liters of water that enter the large intestine all but about 100 mls is absorbed by osmosis. F- The Defecation Reflex 1- The mass movement of feces into the rectum stimulates the defecation reflex 2- In response to distention of the rectal wall, receptors send a signal to sensory spinal nerves. The brain then signals down parasympathetic motor pathways to the rectum and anus causing contraction of longitudinal rectal muscles. This shortens the rectum increasing the pressure. This pressure opens the internal anal sphincter 3- If the external anal sphincter is voluntarily relaxed then defecation will occurs and feces is expelled through the anus. 4- If it is voluntarily controlled then defecation can be postponed. 5- If defecation does not occur the feces is pushed back into the sigmoid colon until the next wave occurs increasing the urge to defecate or the “need to go” 6- In infants the defecation reflex causes automatic emptying of the rectum because voluntary control of the external anal sphincter has not been developed.