Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
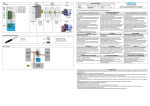
Eterophorias importance in pathogenesis of gnatho postural unbalance Dr. Piero Silvestrini Biavati MD*, DDS*, PhD**, Master in Posturology*** (* Genoa University, ** Siena University, ***Rome University “La Sapienza”) [email protected] Abstract Posturology is now part of practice dentistry. In this article we enphasize two different aspects of head and neck posture, probably strictly related: gnathologic and vision problems. Their alteration can determine a change in body posture. In gnathology, mandibular sidebending, free-way space alteration, abnormal vertical dimension and atypical swallowing, all determine head postural adaptations. In vision science, phorias, strabismus, astigmatisms and eyes motility problems as well , alter head posture. We believe that changes in head posture induced by gnathologic problems can modify visus and vice versa. Key Words gnathology, posturology, free way space, mandibular sidebending, phorias, vision, astigmatism, strabismus, ocular motility, ocular wryneck, head, neck The gnathology he is evolving, concepts off limits only a few years ago, by now accepted from all the gnathological schools. The fact to mostly consider the muscles, in the stomatognatic system, we owe it to Bernard Jankelson in the distant years 50 (9,10). This concept, adverse from the other gnathological schools that entirely centered the problem on occlusal morphology and condylar position in the glenoid fossa (centric relationship), strong of its obviousness and reasonableness, it has unhinged little by little preconceived mechanistic that appear nowadays obsolete. The fact, by now acquired, that the muscular determinant is the principal sub-judice, it sets us in front to other olistic questions type: what does it determine the anomalous muscular activity that brings temporo mandibular disorders ? (1) We can word here a long list, simply departing from the most important: the spatial position of the head, the swallowing, the dysgnathia, the free way space, the column problems etc. you is able therefore to notice that we can estrange there from the TMJ district, always finding anatomical functional correlations (3,11). The same anatomy is suffering a development by the research of many anatomists that, they often find new meniscal condyle insertions with other districts, they discover new muscles and new innervations, that put to hard probation the simplify mechanistic techniques. Our body is so full of variables that we are not able to know her of it all and to foresee with safety which is the origin of the problem of it, in a system so linked that it also prevents us a reliable statistic analysis (20). In the postural physiology they are different the way of imbalance. Every sensorial receptor is potentially able to create troubles in the postural system (4). We won't enter in this Article on the fine postural system (5), we will only deal there with the macros postural adaptations. Easily wiew to a careful objective examination from each of us. Our body is in continuous adaptation, because of the environmental problems that time in time succeed. We will investigate the system of adaptation and oculo-gnatho-postural imbalance. To define a gnatho postural imbalance caused by an eteroforia, we must first of all clarify these terms. Eterophoria: an imbalance of the visual system, generally a binocular vision alteration: they are that troubles of the ocular mobility that are maintained latent from the operation of the cerebral amalgamation; therefore they always admit the binocular vision and they are defined according to the type of bias, in comparison to the ortophoric position of the eyes. In practice they are strabismus that are able to be correct from reflex level. It results obvious that such problems they induce, or perhaps and better to say they force, our body to adaptations turns to a compensation, as far as possible, of the problem caused by the visual system (7). Gnatho postural syndrome: an interaction between mandibular position and head and neck posture. With this term we doesn't intend that only the tall bodily district influences the gnathological system, but simply the strictly correlation. Other districts can influence the cranio cervical posture, and from this to create gnathological alterations and vice versa. A gnathological problem doesn't hardly involve a cranio cervical adaptation. The two adaptations result strictly correlated (15, 17). Mandibular adaptations to the head posture. The muscular system complex depuit to the control of the mandibular position can be simplified in three subgroups, the elevator muscles, the down muscles and the nucal muscles, finalized to different functions (Fig. 2). In fact for mandibular posture we necessarily have to distinguish two different positions: mandibular rest position and closed bite. The muscles used for the rest position (rest position, RP) they are mainly the hyoid muscles. Them, using the hyoid bone as a caruncol, they determine the position of it, what resultant of the tension of all the muscles to it connected (Fig. 1). As the upperhyoids, as the underhyoids and as the correlated muscles with clavicle, cervical rachis, pharynx and language actively participate. The muscles used to intercuspal position (intercuspal position ICP) they are mainly the elevators, temporalis, masseter, pterygoid etc. (3,9,10,11) Naturally these are only front muscular chains, they could not work without a feedback control of the head position with the nucal muscles, in primis sternocleidomastoids and trapezius. In fact, without their operation, the tension of the undermandibular muscles would bring the mandible the more in possible lower part, while contemporarily the uppermandibolars would bring the mandible in ICP, with the outcome to have a head in maximum flexion in front and clenching teeth. The nucal muscles proper feed this effect and therefore are tightly correlated. That's the reason that mandibular posture variations, can involve variations of the cranial posture. Everything is in sagittal how in frontal view(Fig. 3). We can imagine therefore the hyoid mandibular system as a system to two-tier caruncola: an extension of the head will bring to a mandibular rest position more opened (mandibular muscles more lengthened), while a bending to a more closed position (mandibular muscles more shortened). In frontal view a bending of the head to Right, will inevitably cause a shortness of the mandibular muscles Fig. 1 spatial relationships among cranio, of the same side, determining a Right sidebending of the mandible mandible and hyoid (Fig.4). In frontal view, a rotation of the head to Left, it will drag from the same side, in comparison to a bodily median line, both mandible and hyoid (even if in proportionally low measure) but, in comparison to a median craniomandibular axle, the mandible will result sidebended to Right. Then with a gnathological disorder of Right deviation (Fig. 5), the opposite one of the sidebend of the head. Fig. 2 Cranio cervical mandibular hyoid posture Fig. 3 Ortho posture Fig. 4 Head flexed to R Fig. 5 Head flexed to L To notice the move of the ocular visual axis in the three different positions of the head. Muscles orange: more contracted; pink: more lengthened Every skew between RP and ICP causes an asymmetrical job of the muscles and the joints to reach the ICP, potentially becoming iatrogenous in the problematic neuromuscular pain disfunction and TMJ. If then the patient has match between RP and ICP (clench), problem list are subsequently amplified both to muscular and articular level for the job overload that these structures are submitted. The why of this whole examination on the influence of the posture of the head on the mandible we can synthesize in a simple postulation: all of this that is able to influence the posture of the head is able accordingly to determine gnathological problem (adaptation). But the problem can also be seen in opposite way, Fig. 6 Ocular muscles producing a second postulation: the mandibular unbalance (gnathological problem) it is able to influence the posture of the head and accordingly to determine other accommodation phenomenons. Here the forias enter in game …. Every visual defect can induce accommodation phenomenons of the head, to the functional compensation of the pathology. Such adaptations take the name of Ocular Wrynecks (OW) (Fig. 7) (6,14,16,18). From this we can be deduced that visual alterations that produce a OW force the mandible to suit himself for the new cranial posture. The skew has increased from the feedback of the hyoid bone and his muscles, that turn to them induce a further adaptation of the head. Often such compensations are “helped in their stabilization” from the dental clenching: a way to close a muscular chain and to allow the mandible to be “near” to the occlusion. The clenching, in a adaptative circle, will worsen all the gnathological disfunctional parameters. In these cases, you could be hypothesized that the night bruxism is a mean to allow a reoxigenation of the elevator muscles stopped all the day in isometric situation. Fig. 7 Ocular wryneck The opposite side is possibile also. By my experience I can say that Phorias can be modify by changing occlusion. The way is always the same: the adaptation. If the dental occlusion determine a pathological head position, then the visual system must make an adaptation to this head position, modifing the abitual ocular axis (Fig. 9, 3, 4, 5). Fig. 8 Phorias This determines an asymmetrical tension of the ocular muscles. Such imbalance, in a dissociated visual Fig. 9 ocular adaptation to the posture analysis, with the eyes that cannot of the head contemporarily sting the same aim, hands the axis in a not orthogonality situation: the phorias. (Fig. 9)The functional asymmetries of the ocular muscles (Fig. 6) can induce besides sprains of the corneal surface: the astigmatism (Fig. 18, 19, 20, 21), in turn possible carrier of OW.The differential diagnosis is not effortless or easy (2,12,19). Remarkable experiences are necessary in gnathological, postural and vision fields. Diagnostic instrumentations are necessary and the strictly collaboration with specialists of the visual sector: oculists, strabologist, ortottist, comportamental optometrists. Within the physioterapic treatment, the opposite problem is had, to trace the occlusal influences and to appreciate its importance (2,4,19). We introduce some interesting cases, all with correlation between occlusion and visus. First case: evidence of a phoria with occlusal compensation. To normalization occlusal test show ocular wryneck and phorias. Fig. 11 Fig. 10 Balanced Abitual bite: bite: ocular orthophorias wryneck with iperphoria R: R rotation and flexion L Second case: cycloversion normalization (8) after occlusal normalization Fig. 12 Fig. 13 Abitual Balanced bite: bite: cyclovers orthophor ion Left ias eye with Maddox cylinders Third case: normalization of flexion of the head and plantar support that needs the substitution of the lenses. Fig. 14 Abitual bite: false ocular wryneck Fig. 15 Balanced bite: symmetry of the posture of the head with reducingastigmatism Fig. 16 Abitual bite: asymmetry of the Fig. 17 Balanced bite: symmetry of the plantar support plantar support Fourth case: astigmatism variation after occlusal normalization. Fig. 18 Right eye: corneal map before and Fig 19 Left eye: corneal map before and after occlusal balancing. after occlusal balancing. Fig. 20 Right eye: To notice the simulation of the visual sprain to the ototype and the night-blooming reflexes before and after normalization Fig. 21 Left eye: To notice the simulation of the visual sprain to the ototype and the night-blooming reflexes before and after normalization As is been able to notice can be present important interactions between visual apparatus and dental occlusion, between dental occlusion and head posture, among head posture and visual apparatus (2,8). The fine interaction among these districts can induce our diagnosis in bug invalidating the result of these treatments. We always must consider that our body is tightly a complexes of correlated compartments either anatomically or neurologically, with the purpose to be able to make that marvelous function that takes the name of “adaptation.” The only fact to want to correct a adaptation pathology necessarily implicates the taking in consideration of the correlated adaptations. . Bibliography 1) Andorlini M, La saggezza del corpo, Ed. Castello, Milano 2) Bourdiol R. Occhio e Statica, Ed. C.S.T.N.F. Torino 1994 3) Bousquet L, Le catene muscolari, Ed. Marrapese, Roma, 1996 4) Bricot B, La riprogrammazione posturale globale, Ed. Sauramps, Montpellier 5) Gagey PM, Posturologia, Ed. Marrapese, Roma 6) Gambari M, Silvestrini Biavati P, Diagnosi forie e ipomobilità oculare, Atti Congresso Nazionale Patologie di confine di Oculistica, Odontoiatria, Neurologia Otorinolaringoiatria, Cenacolo Ligure, Aqui Terme 5-7 Novembre 2004. 7) Gambari M, Postura e Visione, Atti III Convegno di Posturologia AIFiMM 18-19 Giugno 2005, Genova. 8) Guidetti G, Marchioni D, Vestibolo e sport, Ed Martina, Bologna 9) Jankelson B, Modern diagnosis and management of musculoskeletal dysfunction of the head and neck, Mosby Co., 1982 10) Jankelson B, Neuromuscular aspect of occlusion. Effects of occlusal position on the physiology and dysfunction of the mandibular musculature, Dent. Cl. N.A. 23, 1979 11) Lentini S, Ortodonzia e Postura, Ed. Martina, Bologna 12) Lerman M, A revised view of the dynamics, physiology, and treatment of occlusion: a new paradigm, Cranio, January 2004 13) Silvestrini Biavati P, "Correlazioni fra postura, occlusione e visus. Approccio diagnostico" Atti del X Congresso Nazionale A.I.K.E.C.M. Alessandria 15-16-17 Novembre 1997 14) Silvestrini Biavati P, “Postural variations induced by occlusion and visus: correlation with rachis pathologies” Atti 5° Meeting Ceramics, cells and tissues: Implant for spine. Faenza 1-3 Ottobre 1998 Ed. IRTEC-CNR, Faenza, Consiglio Nazionale delle Ricerche 15) Silvestrini Biavati P, Lastrico M, " Il trattamento neuromuscolare globale posturale e occlusale nella sindrome occluso-posturale" Atti XII Congresso Nazionale A.I.K.E.C.M. I Meeting Internazionale I.C.C.M.O. "Sindrome occluso posturale: ruolo dell'odontoiatria in una patologia multidisciplinare" Vicenza 10-12 Novembre 2000 16) Silvestrini Biavati P, Gambari M, Correlazioni fra occlusione dentale ed astigmatismo Atti Giornate Internazionali di Posturologia, Roma, 12-13 Marzo 2005 17) Silvestrini Biavati P, Correlazioni tra occlusione dentale, ATM ed atteggiamenti posturali, Atti III Convegno di Posturologia AIFiMM 18-19 Giugno 2005, Genova 18) Silvestrini Biavati P, Gambari M, Interazione tra postura mandibolare ed eteroforie, Atti Congresso Nazionale Patologie di confine di Oculistica, Odontoiatria, Neurologia Otorinolaringoiatria, Cenacolo Ligure, Aqui Terme 5-7 Novembre 2004. 19) Villeneuve PH, Piede equilibrio e postura, Ed Marrapese, Roma, 1998 20) Voss DE, Ionta MK, Meyers BJ, Facilitazione neuromuscolare propriocettiva, Piccin Ed. Padova, 1991