Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
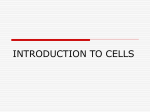
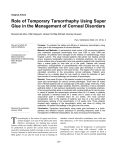
The Ocular Surface Research & Education Foundation Presents: Sutureless Cryopreserved Amnion Grafts: ProKera By Scheffer C.G. Tseng, M.D., Ph.D. ™ Volume 1, Number 2 Overview ProKera™ consists of a piece of AmnioGraft® (cryopreserved human amniotic membrane) clipped into a dual PMMA symblepharon ring system (see sketch left). ProKera™ is used as a biologic bandage for suppressing inflammation and promoting corneal surface healing without sutures. Illustration of inserted ProKera™ Supplies for Procedure ProKera™ is assembled so that the stromal (sticky) side of the tissue is in contact with the corneal surface and fits snugly between the cornea and the eyelids by conforming to the corneal surface. ProKera™ also functions like a symblepharon ring while delivering the therapeutic benefits of a cryopreserved amnion graft including anti-inflammation, antiscarring, anti-angiogenesis, promotion of healing and reduction of patient pain without sutures. After the biologic benefits of the tissue are delivered and healing is achieved, the ProKera™ ring set is removed. ProKera™ is intended for use in eyes where the ocular surface cells have been damaged, or the underlying stroma is inflamed and scarred. It often eiliminates the need for surgery and provides sight saving biologic actions. The most common indications for use are: 1. Sterile lid speculum 2. Sterile gloves 3. Anesthetic drops 4. Antibiotic drops 5. Sterile scissors (provided with the ProKera™ device) 6. Sterile forceps (provided with the ProKera™ device) 7. ProKera™ (by BioTissue™) call for info: 1-888-296-8858 ProKera™ sizes: Catalog # Size PK-15 15 mm PK-16 16 mm • Epithelial defects, erosion, or ulceration • Chemical/thermal burns (acute stage) • Following the removal of corneal lesions, e.g., band keratopathy • Chronic recalcitrant keratitis from HZO, HSV, or vernal keratitis • Stevens-Johnson syndrome (acute stage) • In conjunction with socket or fornix reconstruction (to prevent lid/lash rubbing) ProKera Usage by Application Epithelial Defect/Ulceration 52.1% Chemical/Thermal Burn 11.6% Together with PKP/LKP 9.3% Lid Problems 4.7% Removal of Lesions 3.7% Miscellaneous 18.6% Data provided by Bio-Tissue, Inc. from returned donor recipient information forms from transplanted devices (April 2005 - December 2005). 2 Estimated insertion time: 1 minute Key Surgical Steps NOTE: It is recommended that you view OSREF DVD Vol. 7 and call Dr. Tseng at 305-274-1299 with any questions BEFORE your first procedure. Pre-Insertion Tips: • Verify Eye Closure: If there is an eye closure problem, ProKera™ should not be used. Exposure problems will diminish the effects of the membrane and should be treated prior to ProKera™ insertion or at the time of ProKera™ insertion with additional temporary tarsorrhaphy. ProKera™ Inserted in eye What it looks like • Consider Eye Opening for Sizing: There are two different diameters of ProKera™ available: 15 mm and 16 mm. Most adult patients will tolerate a 16 mm ProKera™ device. ProKera™ should not be used for patients with unusually tight eyelids close to the eyeball making it difficult and/or painful to insert anything between the lid and the globe. • Handle Aseptically: ProKera™ can be inserted in an office setting using aseptic technique; the supplies listed on page 1 assist with handling the device. ProKera™ is packaged in a dual pouch (as shown to the left). The outer aluminum foil pouch should not be placed in the sterile field, but the inner, clear pouch may be placed in a sterile field. The membrane in the device is slippery. Thus, carefully grab the ring with fingers using a sterile glove or with sterile, blunt instruments. Do not trim off the extra membrane hanging over the sides of the ring. Key Insertion Steps: • Use a lid speculum to open the eye • Administer anesthetic drops • Insert ProKera™ into the upper lid first, and then tuck it under the lower lid • Administer prophylactic antibiotic drops after removing the speculum Using a tarsorrhaphy with ProKera™: ProKera™ is packaged in flat dual pack system for easy handling and storage Illustration of ProKera™ inserted under a full tarsorraphy After insertion, if there is no complaint of a foreign body sensation, and the patient seems to have reasonable blink and closure, then there is no need for a tarsorrhaphy. However, if the ProKera™ is a little too small for the eye, or the device does not center well on the corneal surface (e.g. with floppy lids or exophthalmos) or the eye does not blink/close well (e.g. neurotrophic), then add a temporary tarsorrhaphy (see illustration and photo below). Photo of ProKera™ inserted under a partial tarsorraphy Key Surgical Steps (continued) Post-Insertion Care: • Patient Instructions: Patients should be instructed not to rub their eyes, excessively blink or move the ProKera™ insert with their fingers. Patients should not swim or soak their face in water without protective eyewear. The eye should be closed tightly during showering. As vision will be blurred by the opacity of the tissue, patients should not drive, operate heavy machinery or perform any other task that requires unobstructed vision or good depth perception. • Topical Medications: Artificial tears or other eye drops should be used 3-4 times daily, especially if there is a concern about dry eye exposure. The cryopreserved amniotic membrane in ProKera™ does not interfere with antibiotics’ penetration. If desirable, ProKera™ can be soaked in antibiotic solution before placing it in the eye. • Routine Examination with ProKera™: Without removing ProKera™, healing can be assessed using fluorescein staining (see photo to the right) and the IOP can be measured with a Tonopen. If temporary removal is required, then handle the ProKera™ device aseptically and store it in a sterile container with BSS before re-insertion. • Length of Wear: The FDA approved ProKera™ can remain in the eye until the ocular surface has healed or the membrane has dissolved for up to 8 weeks after insertion. However, biologic actions are delivered and healing is complete within 1-2 weeks. For cases with severe inflammation (e.g. acute chemical burns), it is beneficial to insert a new ProKera™ device every 5 days to avoid PMN cells becoming trapped on the membrane which may lessen its therapeutic effect. • Membrane Dislodgment and Dissolution: As the biologic actions of the cryopreserved amniotic membrane are delivered and the ocular surface heals, the membrane will thin and dissolve. If the membrane dissolves after adequate healing has taken place, then remove the device. However, the membrane should not dissolve in less than one week. If it does, this is most likely due to an exposure problem which should be corrected before the insertion of another ProKera™ and/or add a tarsorrahaphy. Removal Tips: ProKera™ can be removed using blunt, sterile forceps with or without the help of a lid speculum. The application of an eye ointment can facilitate the removal. Testimonials (from ProKera™ Users) Neurotrophic Persistent and Non-healing Corneal Epithelial Defects/Ulcers Dr. Michael Ehrenhaus of NY, NY has used ProKera™ in patients with non-healing epithelial defects due to bacterial keratitis. The ProKera™ device stabilized their corneas and helped stop progression of the defects, some of which were deep, almost like a descemetocele. He can be reached for further comments or questions by phone at 718-780-2600. Dr. Lisa Chriss of Orlando, FL was very impressed after using ProKera™ for a patient with a nonhealing epithelial defect and scar due to HZO (under control) which failed to heal after using a bandage contact lens for 3 months. The defect healed 3 days after ProKera™ insertion. She can be reached for comments or questions by phone at 407-629-6646. Dr. George Rosenwasser of Hershey, PA used ProKera™ after EDTA chelation in a one-eyed neurotrophic child with band keratopathy and vascularization. He noted a rapid and impressive improvement. He observed that “This device has fast-tracked the relief of damage from alkali burns to the ocular surface. I recommend it to anyone who sees a serious alkali injury, and the faster it is placed, the better." He can be reached by phone at 717-533-5200. ProKera™ with fluorescein staining Reimbursement: Medicare recommended that HCPCS Level II Supply Code V2790 (preserved amniotic membrane) should be expanded to cover ProKera™ during a May 11, 2006 public hearing. The effective date is pending. Coverage and payment for V2790 is at the discretion of Medicare local carriers. A copy of the invoice should be submitted with the claim form. Due to the complexities in coding and the evolving technology of amniotic membrane transplantation, it is highly recommended that you consult your coding expert with detailed questions. As a general rule, it is advisable to prequalify the patient’s insurance or use an Advanced Beneficiary Notice (ABN) to insure the Medicare patient is aware of responsibility for any costs not covered by the insurance carrier. Testimonials (from ProKera™ Users cont.) High-risk Corneal Transplantation: V.K. Raju, M.D., FRCS, FACS who was a Clinical Professor in the Department of Ophthalmology at West Virginia University School of Medicine, has been treating high-risk corneal transplant cases with ProKera™. Dr. Raju said that ProKera™ proved to quieten the eye and reduce epithelial defects. Even previously problematic cases experience dramatic improvement with ProKera™ treatment. A patient that underwent two prior PKP procedures also had Herpetic Keratitis and extremely dry eyes. At one stage, autologous serum was used for his persistent epithelial dystrophy. He had corneal perforation repaired with a patch graft. Six months later a third PKP was performed with ProKera™. This patient commented after the third PKP in which ProKera™ was inserted that his eye “had never felt so good”. “ProKera™ definitely has a place in corneal transplantation surgery,” said Dr. Raju who is amazed by its rapid healing powers for this indication. You can learn more about Dr. Raju by visiting his website at www.vkraju.com or calling 304-598-0055. Dr. Arun Gulani of Jacksonville, FL reported “In my experience of using AmnioGraft® in an extended spectrum for corneal and ocular surface reconstruction, I envision ProKera™ to be the next logical step in providing an easy to use ‘Natural Bandage’. Its use in surface Laser vision surgery, high risk corneal transplants, chemical burns and emergency corneal situations including trauma is viably evident”. Dr. Gulani can be reached by phone at 904-296-7393 or online at www.gulanivision.com. Chemical/Thermal Burns: Dr. George Rosenwasser of Hershey, PA treated a 6-month-old’s eyes that were exposed to a concentrated alkali solution. Several days later she was seen by a pediatric ophthalmologist who recognized a near total defect and ProKera™ was inserted bilaterally, under topical anesthesia within 24 hours of seeing the child, and remained in the child’s eyes for 2 weeks after which time another set of PROKERA™ was inserted. After twelve weeks of treatment and observation the right eye was virtually normal, the left eye showed a minimal central stromal haze and approximately two clock hours of limbal superficial peripheral vascularization. Dr. Rosenwasser commented that “there's no question that the injury would have caused severe sight threatening damage without the PROKERA™. I recommend it to anyone who sees a serious alkali injury, and the faster it is placed, the better." He can be reached at 717-533-5200. Provided by FAQs: Volume 1, Number 2 1. How often does ProKera™ fall out? Due to the device construction and the placement of ProKera™ under the eyelids, ProKera™ will not fall out with normal wear or blink. However, the device may not be secured well in exophthalmos or severe floppy lid. A tarsorrhaphy can help to limit this. 2. If the sticky stromal side is down, when ProKera™ is removed, what keeps it from taking the epithelium with it? ProKera™ acts as a biologic bandage and the epithelial healing takes place with the help of the biologic actions of the membrane underneath. Once the corneal surface inflammation reduces and the defect heals (visible by fluorescein staining), the amniotic membrane clipped into the PMMA rings will thin out or dissolve completely. The remaining PMMA ring will need to be removed after this has happened. No epithelium will be removed with the ring, even if the membrane is still intact. 3. What happens if the graft is sloughing off even with a tarsorrhaphy? It is likely that there is an exposure problem if this happens. For example, in a recent case a patient suffering from the lack of Bell's phenomenon (after HZO) the eye was not rotating during sleep. This created a severe exposure of the lower portion of the cornea as it is never covered by tear film. Amniotic membrane healed the defect, but broke down again for the very same reason. To overcome this issue, blood vessels will have to be brought to the peripheral cornea using a conjunctival flap and then covering it with ProKera™. 4. What if the membrane slips out of the ProKera™ ring? Should I try to clip it back in? The amnion graft inserted in the ProKera™ ring will thin out as the healing of the corneal surface progresses. Occasionally this will cause the membrane to detach from the ring. If this occurs, remove the device. Do not try to reassemble it. Provided the healing is complete, another ProKera™ is unnecessary. 5. Why is there mucous debris with ProKera™ inserted? The membrane may show some degradation during wear and thus generate some mucous debris. If this occurs simply rinse with non-preserved saline. Financial interest disclosure: Dr Tseng and his family are >5% shareholders of TissueTech, Inc. and Bio-Tissue, Inc. which currently distributes AmnioGraft® and ProKera™. The Ocular Surface Research & Education Foundation (OSREF) To order Ocular Surface Research & Education Foundation DVD’s call 1-888-296-8858 For additional clinical information, contact Scheffer C.G. Tseng, M.D., Ph.D. by phone at 305-274-1299 or by e-mail at [email protected]