Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
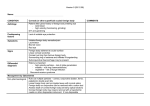
ARCH SOC ESP OFTALMOL 2007; 82: 475-482 ORIGINAL ARTICLE SUBCONJUNCTIVAL APPLICATION OF PLASMA PLATELET CONCENTRATE IN THE TREATMENT OF OCULAR BURNS. PRELIMINARY RESULTS APLICACIÓN SUBCONJUNTIVAL DE CONCENTRADO DE PLAQUETAS PLASMÁTICAS EN EL TRATAMIENTO DE QUEMADURAS OCULARES. RESULTADOS PRELIMINARES MÁRQUEZ-DE-ARACENA R1, MONTERO-DE-ESPINOSA I1, MUÑOZ M2, PEREIRA G3 ABSTRACT RESUMEN Purpose: The efficiency of the subconjunctival application of autologous platelet concentrate in patients with ocular burns was assessed. Methods: This was carried out by analysing the effect of treatment in the eyes of 10 patients suffering from ocular burns as a result of work-related accidents. Two types of treatment were evaluated: the first group only received conventional topical medical treatment; and the second group, in addition, had subconjunctival injection of plasma platelet concentrate. The clinical condition of the patient and the period in which the disease prevented the patient from working were studied; monitoring was carried out until the burns had fully healed. Results: Statistically significant differences were found between the group treated with subconjunctival autologous platelet concentrate and the group treated with conventional topical medications, with Objetivo: Se valoró la eficacia de la aplicación subconjuntival de concentrado de plaquetas plasmáticas autólogas en pacientes con quemaduras oculares. Método: Para ello se analizaron 10 ojos de 10 pacientes que sufrieron accidentes laborales por quemaduras oculares del mismo grado. Se establecieron dos tipos de tratamiento: al primer grupo, control, se le aplicó tratamiento médico tópico convencional; al segundo, se le añadió además, inyección subconjuntival de concentrado de plaquetas autólogas. Se estudió la evolución clínica, días que le incapacitaron dicha patología para su actividad laboral y seguimiento hasta su curación final. Resultados: Se encontraron diferencias entre el grupo de los tratados con concentrado de plaquetas autólogas subconjuntivales respecto al grupo con tratamiento médico tópico convencional, siendo más corto el tiempo de cicatrización de córnea (sig- Received: 17/7/06. Accepted: 12/6/07. FREMAP Hospital, Sevilla. Centro Cid Clinic, Sevilla. Surgery Dept. (Ophthalmology Area). Medicine Faculty of Seville University. 1 Ph.D. in Medicine. Seville University. Spain. 2 Ph.D. in Medicine. Virgen del Rocío Hospital. Seville. Spain. 3 Graduate in Medicine. Virgen del Rocío Hospital. Seville. Spain. Study financed by the Casa Real de los Godos Institution. Correspondence: Rafael Márquez de Aracena del Cid Servicio de Oftalmología Hospital FREMAP de Sevilla Avda. de Jerez, s/n Sevilla Spain E-mail: [email protected] MÁRQUEZ-DE-ARACENA R, et al. a shorter period of time in corneal and conjunctival healing, time on sick leave and time needed for full healing. Conclusions: Subconjunctival infiltration of autologous platelet concentrate should be considered as a straightforward, economical and possibly effective form of treatment for traumatic accidents (burns) of the ocular surface (Arch Soc Esp Oftalmol 2007; 82: 475-482). nificativamente estadístico), conjuntiva, baja laboral y tiempo hasta curación final. Conclusiones: Podemos considerar la autoplaquetoterapia subconjuntival (infiltración subconjuntival de concentrado de plaquetas autólogas) como un tratamiento sencillo y económico en el tratamiento de las alteraciones traumáticas (quemaduras) de la superficie ocular. Cuya eficacia deberá ser confirmada por series mayores. Key words: Ocular surface, ocular burns, platelet, growth factors, cornea. Palabras claves: Superficie ocular, quemaduras oculares, plaquetas, factores de crecimiento, córnea. INTRODUCTION morphnuclear (PMN) to the cornea (9). These will produce leucotrienes, chemotactics for new neutrophiles and collagenase which would cause the enzymatic degradation of the collagen and therefore corneal perforation. The epithelial growth factor which stimulate keratocytes to form new anomalous collagen which will cause a whitish scar and develop intra-cytoplasmatic contractile fibrils which will cause scarring and possibly irregular astigmatism (4). The objective of the treatment is to achieve corneal and conjunctival epithelialization as fast as possible with the least possible permanent damage. Prolonged episodes of corneal de-epithelialization increase the production of collagenase in the corneal stroma, which may reach corneal perforation. The basis of conventional treatment, comprises abundant ocular washing, cleaning product remains from the ocular surface, debridling necrotic areas and applying topical treatment with corticoids, antibiotics and cyclopegics (3). Severe lesions may require, in addition to the above, systemic medical treatment such as tetracyclines (10), corticoids, antioxidants and collagen synthesis enhancers such as ascorbic acid (11). In serious burns, surgical treatment options may be necessary such as amniotic membrane transplant (12), or self grafting of sclerocorneal limbus (13) in order to regenerate limbar stem cells to promote epithelial formation and suppressing fibrosis. The classic techniques include self-hemotherapy —subconjunctival injection of autologous blood— in patients with important ocular burns, the inefficiency of which has been proven (14-17) even when associated to other substances (18). On the other hand, it is known that autologous serum seems to facilitate epithelial regeneration and Ocular burns account for 12-19% of eye traumatisms (1), generally involving young people in their working or domestic activities (2). This pathology requires quick and efficient action from which the final prognosis will depend. Burns can be chemical or physical. Most of chemical burns are produced by acid or alkaline substances. The severity of a chemical burden is related to the concentration of the product, the pH of the solution and the exposure time. Alkaline products cause more serious damages due to a denaturalization of proteins and saponification of membrane lipids, which allows the alkaline material to quickly penetrate the cornea and enter the eye. In turn, acid precipitate corneal proteins, which act as a buffer and barrier against deeper penetration. In general, the health professional must consider the degree of involvement of the cornea, of the conjunctiva and the sclerocorneal limbus, with the letter had been increased relevance because it hosts the stem cells in charge of epithelium regeneration (3). After a corneal burn, there is a first attempt at recovery, whereby the basal epithelial cells on the edges of the ulceration lose their hemidemosomes and migrate to cover the defect. The definitive recovery will be at the expense of the transitory cells and limbar stem cells (4). When these are destroyed, due to the action of chemical mediators found in the stroma and the absence of fibroblasts —which produce keratocyte growth factors— (5), the conjunctival epithelium undergoes a transformation and covers the cornea (6,7). The increased vascularization will end up conjunctivalizing the cornea (8). In the corneal stroma, the collagen is degraded, which stimulate the migration of poly- 476 ARCH SOC ESP OFTALMOL 2007; 82: 475-482 Treatment of ocular burns with plasma platelet healing of ocular surface pathologies (19-22) because, among other things, it provides growth factors. Said growth factors are proteins which play an essential function in complex tissue repair and regeneration processes. They intervene in intercellular communication, transmitting their information by interacting with receptors in the cellular membrane. In addition, they enhance cellular chemothaxis, proliferation and differentiation (23). Growth factors can be found inside platelets and stored in alpha granules, and several endogenous factors have been found to be involved in the repair of tissues (24), including the eye (25). The possible application of growth factors derived from platelet concentrates on epithelium corneal cells could enhance their trophism (26). In cell cultures, it has been observed that the application of specific serum and plasma fractions enhance the growth, migration and differentiation of cells (27). In addition, a possibility has opened for the utilization of asthmatic platelet concentrates in ocular surface pathologies such as transplants (28). The efficiency of topical application of autologous serum and of autohemotherapy in specific alterations of the ocular surface may lead to the conclusion that the therapeutic potential of this technique resides in the content of the platelet fraction containing the blood. To date, it has not been proved that growth factors are the only blood derivatives which enhance corneal epithelialization processes. At this point, it is necessary to determine whether the application of plasma platelet concentrates act efficiently in the regeneration of ocular surface alterations. For this, the regeneration of burned ocular surface tissues after the subconjunctival application of plasmatic platelet concentrates was clinically analyzed, assessing the utility and inefficiency of the said technique. The preliminary results are presented below. SUBJECTS, MATERIAL AND METHOD We analyzed ten eyes of ten patients who attended the urgency practice of our hospital (Labor pathology monographic) due to Labor accidents: grade 3 ocular burns as per Dua classification (29), that is with corneal defects with three to six hours of corneal involvement and with 30-50% of conjunctival lesion. After receiving prescribed treatment according to method and protocol, we made clinical follow up until healing. The patients were selected in sequential manner among the first who attended the urgency service with said pathologies and authorized the corresponding treatments. In those who had burns in both eyes the one with the more severe injury was chosen for the study. Distribution in groups The patients were divided in two groups depending on the treatment they received: — Group A (5 patients) received conventional topical treatment. — Group B (5 patients) received topical treatment + subconjunctival platelet concentrate (SPC). Conventional medical treatment was given to all patients of the study, as follows: After a profuse ocular wash with saline solution and cleaning with swab, the following medical treatment was established: cycloplentolate eye drops, 1 drop every 12 hours; dexametasone eye drops, 1 mg and tobramycine 3 mg (tobradex, Alcon-Cusí Labs) 1 drop every 6 hours: retinol palmitate cream, 10.000 U.I. + gentamicine sulphate 3 mg + DL-Methionine 5 mg (epithelializing eye cream, Novartis) every 6 hours + occlusion of the eye. When found necessary, antitetanus procedure was adopted. For Group B the following protocol was used: 1. Detailed information was given to the patient who then signed the informed consent. 2. Extraction of 20 cc of peripheral blood in 4.5 ml sterile tubes with 0.5 ml sodium citrate base as anticoagulant. In addition, blood was extracted for clinical analysis comprising complete hemogram and biochemistry, hepatitis and HIV. The tubes with the blood samples were centrifuged 7 minutes at 2,100 rpm, separating the plasma in fractions. For our study we utilized the plasma fraction with more platelets, i.e., the 200400 µl (0.2-0.4 cc.) immediately above the red series. 1-2 ml were obtained after centrifugation when hematocrite is within the usual clinical parameters. ARCH SOC ESP OFTALMOL 2007; 82: 475-482 477 MÁRQUEZ-DE-ARACENA R, et al. Subconjunctival treatment RESULTS In a sterile environment (operating theatre) and after 3 applications in the eye to be treated of 1 drop every 3 minutes of 1mg clorhydrate tetracaine + 4mg of clorhydrate oxybuprocaine (Colircusi double anesthetic®, Alcon-Cusí), the platelet concentrate was subconjunctivally injected in the bulbar conjunctiva (fig. 1) 0.5-1 ml as 12 o’clock and another one at 6 o’clock. Antibiotic cream + antiinflammatory eye drops were applied, with 24-hour occlusion. Clinical evaluation method The patient’s subjective symptoms and the clinical evaluation of the lesions were assessed by slit lamp biomicroscopy with/without topical fluorescein dyeing. To measure the injuries as well as the evolution thereof, the eye was divided in 12 hourly Due sections (29), analyzing the fluorescein-dyed area and hyperemia. Data were collected in a Type Excel base.. The statistical study was made as follows: mean values with standard deviation; percentages by means of Tukey pivots and signification by means of the Kruskal-Wallis test, as well as Pearson correlations (parametric and non-parametric). Ten male patients who had suffered Type III caustic eye burns as per Dua classification (35) due to labor accidents. The mean age of these patients was of 32.25 years (SD=15.52). Four were right eyes (40%), five were left eyes (50%) and one had both eyes involved (10%). In what concerns the labor field of the patients, 50% (five patients) were from the construction industry, followed by the services sector (30%, three patients) and 20% from manufacturing (two patients). The most frequent etiological agents were six patients with alkali burns (60%), three due to solvents (30%) frequently used in construction and services, and one patient due to acids (10%). As regards the cicatrization time of the cornea, it was of 6 days for group A (conventional treatment) and 3 days for group B (platelet self-therapy), with statistically significant differences being found (0,001) between both groups. The conjunctival cicatrization time was longer in group A (6 days) than in group B (4 days), although the difference was not statistically significant (0.017). In what concerns keratitis, shortening was evident in group B patients (6 days) vis-à-vis group A (9 days) but, as above, the difference was not statistically significant. As for the time off work, no statistically significant differences were found between group A (7 days) and group B (6 days). In contrast, the final healing time exhibited differences between group A (10 days) and B (6 days) but, as with other parameters, these were not statistically significant (0.017). The analytical study of patients treated with autologous plasma concentrates did not reveal any correlations with the parameters of the study (parametric and non-parametric Pearson correlation). Side effects of the treatments Fig. 1: Conjunctival chemosis after infiltration of subconjunctival plasmatic platelet concentrate in an eye with alkali burns. 478 Group A did not evidence undesirable effects. In Group B, 100% of the patients treated with subconjunctival platelet concentrate exhibited no chemosis after 24 hours (fig. 2). Three patients (60%) referred ocular irritation one minute after injection, which disappeared within 3-5 minutes. Three patients (60%) exhibited highly localized and slightly ele- ARCH SOC ESP OFTALMOL 2007; 82: 475-482 Treatment of ocular burns with plasma platelet (EGF) and neural growth factor (NGF) seem to enhance the healing of corneal defects (36-38), improving vision and corneal sensitivity (39). Endothelial vascular factors could play an important role in the physiology of epithelial conjunctival cells (25). It has also been proven that the exogenous application of factors (KGF-2) in experimental animals (rabbits) could stimulate the migration of limbar stem cells to the center of the cornea, thus enhancing the healing of a burnt cornea (40). Said stimulation seems to be related to the concentration of growth factors (41). The growth factors in the amniotic membrane enhance the growth of cultivated limbar stem cells (42). The topical application of mice growth factors in three patients with persistent epithelial defects due to neurotrophic keratitis improved the condition, but application problems were noted due to costs as well as technical difficulties (43). In this study it can be seen that the subconjunctival injection of autologous platelet concentrates produces a statistically significant reduction of the cicatrization time in Type III corneal burns (0.001). In what concerns the cicatrization of the conjunctiva, a certain degree of activity of endogenous growth factors had been described in the regeneration thereof (25). Our study evidences a reduction of the conjunctival cicatrization time in Type III burns with platelets vis-à-vis the conventional treatment (group A) which is not statistically significant (0.017). These results should be verified in larger trials. In relation to keratitis, a shorter healing period was seen in group B patients (6 days) in comparison to group A (9 days) which, however, was not statistically significant. Fig. 2: Bulbar conjunctiva 24 hrs after subconjunctival infiltration of plasmatic platelet concentrate. vated small orange-colored subconjunctival deposits in the infiltration points, which disappeared after 8 days (average). No permanent sequels were found in any of the treated eyes. DISCUSSION The treatments for correcting corneal epithelializing defects include the application of autologous serum, in neuroparalytic, neurotrophic keratitis (30), chronic eye surface diseases (31), keratoconjunctivitis sicca (32,33) and persistent defects of the corneal epithelium (34,35). Autologous serum seems to facilitate the epithelializing healing and regeneration of eye surface pathologies (19-22) because it provides growth factors and improves corneal sensitivity after application (30). In addition, the topical use of other growth factors such as the epidermic growth factor Table I. Summary of results Days off Type III Healing time Type III Corneal healing Type III Conjunctival healing Type III Group A Group B M 5 5 P50 7 6 [P25-P75] [6-9] [4-6] P 0.053 Group A Group B 5 5 10 6 [8-15] [6-7] 0.017 Group A Group B 5 5 6 3 [4-7] [2-3] 0.001 Group A Group B 5 5 6 4 [6-7] [4-6] 0.017 ARCH SOC ESP OFTALMOL 2007; 82: 475-482 479 MÁRQUEZ-DE-ARACENA R, et al. Even though it is not a strictly clinical factor, the time off work of patients seemed to be a convenient value to be included due to its social and economic relevance. The results are very similar (7 days in group A and 6 days in group B). As for the final healing time of the burns, differences were found between group A (10 days) and group B (6 days) which were not statistically significant (0.017). The shorter corneal cicatrization period (statistically significant), of the conjunctiva, the time off work and the final healing time of the patients treated with plasmatic platelet concentration (group B) as compared to the group treated with conventional procedures (group A) could indicate that the subconjunctival application thereof plays an active and efficient function in the external ocular regeneration processes of traumatic etiology (burns). Therefore, the topical utilization thereof could be considered. The patients treated with autologous platelet concentrates (group B) did not evidence any correlation between the different analytical results (hematic and biochemical) vis-à-vis the parameters of the study. The efficacy of this treatment is evidenced in the generally shorter healing and cicatrization time of the conjunctiva and healing time of Type III ocular burns (35), which becomes statistically significant in corneal cicatrization. The presence of small localized conjunctival elevations seems to indicate the location of platelet concentrate deposits which could be released later on, prolonging the effect of said treatment. The subconjunctival application of plasma rich in plasmatic platelets seems to accelerate the healing of clinical signs existing in ocular pathologies such as corneal and conjunctival ulcers. In processes appearing several days after said application, such as keratitis, it does not seem to be particularly efficient. Accordingly, the topical use thereof could be considered. In our experience, the clinical efficacy of subconjunctival application of platelet fraction allows us to deduce that it is not necessary to activate the platelet concentrate for it to be efficient and that the possibility of a new application for treating ocular burns could be of interest. In addition, the tissular regeneration action of blood can be found mainly in the platelet fraction. The technique utilized in our study allows for the exclusive obtainment of platelets, excluding inflammatory interleukines of leucocytic origin. Disease 480 transmission risks are avoided because the plasma is autologous and in addition it is prepared immediately on an outpatient basis, as well as having a null antigenic effect and a very low cost. The fact that the platelet concentrate evidences regenerating activity in the ocular surface opens a new range of applications for treating ocular surface pathologies. The subconjunctival application of autologous plasmatic platelets (platelet self-therapy) in traumatic eye lesions – burns – is a simple and economic treatment for ocular surface burns, free of undesirable side effects. However, the efficiency thereof must be confirmed with larger series. REFERENCES 1. Reim M, Redbrake C, Schrage N. Heridas oculares químicas y térmicas. Tratamiento quirúrgico y médico basado en hallazgos clínicos y patofisiológicos. Arch Soc Esp Oftalmol 2001; 76; 79-124. 2. Morgan SJ. Chemical burns of the eye: causes and management. Br J Ophthalmol 1987; 71: 854-857. 3. Rapuano CJ, Luchs J, Kim T. Requisitos en Oftalmología. Segmento Anterior. Madrid: Harcourt 2001; 288-293. 4. Cameron JD. Corneal reaction to injury. In Krachmer JH, Mannis MJ, Holland EJ. Cornea: Fundamentals of cornea and external diseases. St. Louis: Mosby; 1997. 5. Kruse FE, Tseng SC. Epithelial growth is promoted by a mitogen from fibroblast conditioned medium. Invest Ophthalmol Vis Sci (ARVO Suppl) 1991; 34: 1011. 6. Harris TM, Berry ER, Pakurar AS, Sheppard LB. Biochemical transformation of bulbar conjunctiva into corneal epithelium: an electrophoretic analisys. Exp Eye Res 1985; 41: 597-605. 7. Buck RC. Ultrastructure of conjunctival epithelium replacing corneal epithelium. Curr Eye Res 1986; 5: 149-159. 8. Huang AJ, Watson BD, Hernandez E, Tseng SC. Induction of conjunctival transdifferentiation by photothrombotic occlusion of corneal neovascularization. Ophthalmology 1988; 95: 228-235. 9. Pfister RR, Haddox JL, Dodson RW, Harkins LE. Alkali-burned collagen produces a locomotory and metabolic stimulant neutrophils. Invest Opthalmol Vis Sci 1987; 28: 295-304. 10. Ralph RA. Tetracyclines and the treatment of corneal stromal ulceration: a review. Cornea 2000; 19: 274-282. 11. Pfister RR, Paterson CA, Spiers JW, Hayes SA. The efficacy of ascorbate treatment after severe experimental alkali burns depends upon the route of administration. Invest Ophthalmol Vis Sci 1980; 19: 1526-1529. 12. Kruse FE, Rohrschneider K, Völcker HE. Multilayer amniotic membrane transplantation for reconstruction of deep corneal ulcers. Ophthalmology 1999; 106: 1504-1510. 13. Morgan S, Murray A. Limbal autotransplantation in the acute and chronic phases of severe chemical injures. Eye 1996; 10: 349-354. 14. Trusov MS, Rozenkrants KB. Surgical treatment of chemical burns of the eye in combination with irrigation with ARCH SOC ESP OFTALMOL 2007; 82: 475-482 Treatment of ocular burns with plasma platelet 15. 16. 17. 18. 19. 20. 21. 22. 23. 24. 25. 26. 27. 28. defibrinated blood and subconjunctival administration of autoblood with antibiotics. Vestn Oftalmol 1966; 79: 6165. Sallai S, Fehér J, Podhorányi G. Experience with autologous blood therapy in burns. Klin Monatsbl Augenheilkd 1967; 150: 879-886. Dolezalova V. Kutskova L. Subconjunctival injection of autogenous blood in the eye after thermical and chemical burns. Cesk Oftalmol 1973; 29: 207-212. Lenkiewicz E, Ferencowa A, Szewczykowa E. Subconjuctival autohemotherapy of eye burns in our cases. Klin Oczna 1992; 94: 113-114. Kuprianowicz W, Czesnel H. Results of treatment of calcium eye burns with subconjunctival injections of blood. Klin Oczna 1969; 39: 51-54. Fox RI, Chan R, Michelson JB, Belmont JB, Michelson PE. Beneficial effect of artificial tears made with autologous serum in patients with keratoconjunctivitis sicca. Arthritis Rheum 1984; 27: 459-461. Tsubota K, Goto E, Shimmura S, Shimazaki J. Treatment of persistent corneal epithelial defect by autologous serum application. Ophthalmology 1999; 106: 1984-1989. Tsubota K, Goto E, Fujita H, Ono M, Inoue H, Saito I, et al. Treatment of dry eye by autologous serum application in Sjogren's syndrome. Br J Ophthalmol 1999; 83: 390-395. Goto E, Shimmura S, Shimazaki J, Tsubota K. Treatment of superior limbic keratoconjunctivitis by application of autologous serum. Cornea 2001; 20: 807-810. Bennet NT, Schultz GS. Growth factors and wound healing: biochemical properties of growth factors and their receptors. Am J Surg 1993; 165: 728-737. Rendu F, Brohard-Bohn B. The platelet release reaction: granules´ constituents, secretion and functions. Platelets 2001; 12: 261-273. Gebhardt M, Mentlein R, Schaudig U, Pufe T, Recker K, Nölle B, et al. Differential expression of vascular endotehial growth factor implies the limbal origin of pterygia. Ophthalmology 2005; 112: 1023-1030. Hartwig D, Harloff S, Liu L, Schlenke P, Wedel T, Geerling G. Epitheliotrophic capacity of a growth factor preparation produced form platelet concentrates on corneal epithelial cells: a potencial agent fort the treatment of ocular surface defects? Transfusion 2004; 44: 1724-1731. Hartwig D, Herminghaus P, Wedel T, Liu L, Schlenke P, Dibbelt L, et al. Topycal treatment of ocular surface defects: comparison of epitheliotrophic capacity of fresh frozen plasma and serum on corneal epithelial cells in an in vitro cell culture model. Tranfus Med 2005; 15: 107-113. Marquez de Aracena del Cid R, Montero de Espinosa Escoriaza I, Muñoz Sáez M, Pereira Gutiérrez G, Martín Leal F. Tratamiento con concentrado plaquetario plasmático subconjuntival y tópico en el trasplante de limbo. Mapfre Medicina 2006; 17: 280-285. 29. Dua HS, King AJ, Joseph A. A new classification of ocular surface burns. Br J Ophthalmol 2001; 85: 1379-1383. 30. Matsumoto Y, Dogru M, Goto E, Ohashi Y, Kojima T, Ishida R, et al. Autologous serum application in the treatment of neurotrophic keratopathy. Ophthalmology 2004; 111: 1115-1120. 31. Ogawa Y, Okamoto S, Mori T, Yamada M, Mashima Y, Watanabe R, et al. Autologous serum eye drops for the treatment of severe dry eye in patients with chronic graft-versus-host disease. Bone Marrow Trasnplant 2003; 31: 579583. 32. Fox RI, Chan R, Michelson JB, Belmont JB, Michelson PE. Beneficial effect of artificial tears made with autologous serum in patients with keratoconjunctivitis sicca. Arthritis Rheum 1984; 27: 459-461. 33. Tananuvant N, Daniell M, Sullivan LJ, Yi Q, Mckelvie P, McCarty DJ, et al. Controlled study of the use of autologous serum in dry eye patients. Cornea 2001; 20: 802-806. 34. Tsubota K, Goto E, Shimmura S, Shimazaki J. Treatment of persistent corneal epithelial defect by autologous serum application. Ophthalmology 1999; 106: 1984-1989. 35. Tsubota K, Goto E, Fujita H, Ono M, Inoue H, Saito I, et al. Treatment of dry eye by autologous serum application in Sjogren's syndrome. Br J Ophthalmol 1999; 83: 390395. 36. Lambiase A, Manni L, Rama P, Bonini S. Clinical application of nerve growth factor on human corneal ulcer. Arch Ital Biol 2003; 141: 141-148. 37. Baum J. Topical treatment with nerve growth factor for corneal neurotrophic ulcers. Surv Ophthalmol 1999; 43: 372-373. 38. Lambiase A, Rama P, Bonini S, Caprioglio G, Aloe L. Topical treatment with nerve growth factor for corneal neurotrophic ulcers. N Engl J Med 1998; 338: 1174-1180. 39. Bonini S, Lambiase A, Rama P, Caprioglio G, Aloe L. Topical treatment with nerve growth factor for neurotrophic keratitis. Ophthalmology 2000; 107: 1347-1351. 40. Liu L, Li YP, Huang SQ, Lin JX, Zhang WX. Mechanism of keratinocyte growth factor-2 accelerating corneal epithelial wound healing on rabbit alkali burned cornea. Zhonghua Yan Ke Za Zhi 2005; 41: 364-368. 41. Mathers WD, Sherman M, Fryczkowski A, Jester JV. Dose-dependent effects of epidermal growth factor on corneal wound healing. Invest Ophthalmol Vis Sci 1989; 30: 2403-2406. 42. Yam HF, Pang CP, Fan DS, Fan BJ, Yu EY, Lam DS. Growth factor changes in ex vivo expansion of human limbal epithelial cells on human amniotic membrane. Cornea 2002; 21: 101-105. 43. Daniele S, Gilbard JP, Schepens CL. Treatment of persistent epithelial defects in neurotrophic keratitis with epidermal growth factor: a preliminary open study. Graefes Arch Clin Exp Ophthalmol 1992; 230: 314-317. ARCH SOC ESP OFTALMOL 2007; 82: 475-482 481