Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
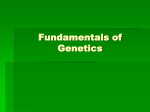
IJP International Journal of Pharmagenesis 2(1), January-June 2011, pp. 115-120 A Review on Hutchinson-gilford Syndrome “PROGERIA” Kinja K. and Gupta N. NIMS Institute of Pharmacy, Shobha Nagar, Jaipur-303121, Rajasthan, India Abstract: Progeria (also known as “Hutchinson-Gilford Progeria Syndrome “) is an extremely rare genetic condition wherein symptoms resembling aspects of aging are manifested at an early age. Progeria is a rare condition that is remarkable because its symptoms strongly resemble normal human aging, but occur in young children. It is never transmitted from parent to child since the individuals with Progeria do not live long enough to reproduce. Currently, there are about 50 known cases of HGPS in the world and most Progeria patients die at around 13 years of age. HGPS is caused by a mutation in the Lamin A gene (LMNA) that results in the synthesis of a mutant prelamin A (also called progerin). Progerin undergoes farnesylation but cannot be further processed to mature lamin A, a key structural component of the cell nucleus. In HGPS cells, progerin accumulates at the rim of the nucleus, causing misshapen nuclei. There is no cure for Progeria but we can treat some of the symptoms. Key Words: Premature aging, Progeria of childhood, Progerin. Introduction Progeria is also known as Hutchinson-Gilford Progeria Syndrome, Werner Syndrome (adult form), Cockayne Syndrome, and RothmundThomson Syndrome. The name stems from the Latin and Greek words of pro and geriaos which mean, in the simplest terms, ‘prematurely old’. Progeria occurs in two forms; Hutchinson Gilford syndrome and Werner Syndrome. It was first described by DR. Jonathan Hutchinson in 1886 and Dr. Hastings Gilford in 1904 (Hutchinson-Gilford) and by Otto Werner in 1904 (Werner)[1,2]. Progeria is an extremely rare genetic disease that accelerates the aging process to approximately 7 times the normal rate. Children with this disease will experience similar conditions, respiratory, cardiovascular, and arthritic, that a 70 year old person would[3]. Corresponding Author: Kuldeep Kinja E-mail: [email protected] Children with progeria look normal during their first years of life, but soon symptoms begin to appear. By the age of 1 or 2, their hair turns lighter in colour, and eventually begins to fall out. By 3 or 4, they are almost completely bald, thin skinned, wrinkled and spotted in various parts of their body, with a stooped appearance and large veiny heads, a pinched nose, delayed tooth formation, stiffness of joints, hip dislocations, cardiovascular problems, arteriosclerosis, wrinkled/aged-looking skin, dwarfism [4]. The children develop early arteriosclerosis, high blood pressure heart disease, and stroke. They do not, however, typically show other characteristics of aging such as Alzheimer’s disease, and arthritis of the hips unless caused by prior hip dislocations. They very rarely reach a height of 107cm or a weight of 18 kg. People with progeria seldom make it to the approximate age of 30, and for most the lifespan is the early teens. They all bear a remarkable resemblance to each other. They both look alike and are affected by very similar symptoms. Although their physical appearance 116 is beyond their years their mental development and intelligence is at the normal place for their actual age[5,6]. History of Progeria Dr. Jonathan Hutchinson recorded the first Progeria case in 1886 and in 1904; Dr. Hastings Gilford recorded another case. Progeria is a rare genetic condition that affects one in eight million new-borns worldwide. It can occur without any cause and can be seen in a family with no history of progeria. In very rare cases, more than one child from the same family can be affected by the disease. In the nearly 120 years since it was first identified, more than 130 cases have been reported in the scientific literature., At present there are 53 known cases of Progeria around the world and only 2 in the UK”. There is a reported incidence of Progeria of approximately 1 in every 4 to 8 million new-borns. Both boys and girls run an equal risk of having Progeria. Progeria appears to affect children of all races equally. Over the last 15 years the following countries have had reported cases - Algeria, Argentina, Australia, Austria, Canada, China, Cuba, England, France, Germany, Israel, Italy, Mexico, the Netherlands, Poland, Puerto Rico, South Africa, South America, South Korea, Switzerland, Turkey, the US, Venezuela, Vietnam and Yugoslavia. It is estimated that 97% of all children with Progeria are Caucasian and males outnumber females by a 1.5:1 ratio. Sadly, death can occur between the ages of 7-28, but the average age is 13.4 years. It is estimated that 80% of Progeria deaths are caused by congestive heart failure or heart attacks. While the average life expectancy of a child with Progeria is less than 14 years, it is believed that the oldest case ever recorded 26 years of age. Not true. The oldest case ever recorded was a Japanese man who lived with the disease for 45 years. In this particular case, the child did not show signs of growth retardation until around 12 years of age. It was noted, however, that his head was larger than normal at the age of one and he did experience hair loss in childhood, but enjoyed International Journal of Pharmagenesis, 2(1) 2011 a rather normal life for 12 years. By age 20, this particular subject had total Alopecia and aging began to accelerate. The subject died at the age of 45 from myocardial infarction. Progeria Syndromes Following are 2 types of progeria syndromes[7]Hutchinson-Gilford Progeria • • • Nearly 1 out of 8 million children suffer from this syndrome. The child with this syndrome appears normal at birth, but the symptom begins to appear at the age of 6 to 12 months. The baby fails to gain weight and also there are changes in skin. Characteristics of Hutchinson-Gilford syndrome • • • • • • Face and Head – Prominent eyes and scalp veins, baldness, delayed tooth formation, small jaw. Bones – short stature, hip dislocations, joint stiffness, thin limbs and prominent joints. Artery and heart disease. About 97% affected children are Caucasian. All children who have this syndrome share a similar appearance, whether they are of same race or ethnic background. Children with this syndrome generally survive to an age of 13 years and most of them succumbing to heart diseases. Werner Syndrome • This syndrome is the most common type of progeria. • It occurs in about 1 person out of 1 million people. • When a child in adolescence fails to have a normal growth is the identification of Werner syndrome. • Hence, the result is the young person looks elderly. Characteristic of Werner Syndrome are – • There is a remarkable difference in a person’s real age and appearance. A Review on Hutchinson-Gilford Syndrome “PROGERIA” • • • • • Face and head – Face wrinkling, balding and greying of hair, cataracts, small jaw and sunken cheek, and voice of high pitch. Bones – small stature, osteoporosis, weakness. Cancer and diabetes are common in this syndrome. Werner syndrome mostly occurs in Sardinian and Japanese people. People with the syndrome mostly survive to an age of 46, mostly succumbing to cancer and heart diseases Cause of Progeria Due to the extreme rarity of progeria and the little research done on it. Scientific research has also shown that the chemical hyaluronic acid is found in elevated levels in the urine of both HutchinsonGilford and Werner patients. Another theory suggests that it is caused by a genetic defect in the repair of DNA, which with a single change to only one copy of a gene could be the cause. According to the Progeria Research Foundation “a group of leading scientists from The Progeria Research Foundation’s Genetics Consortium was able to isolate the Progeria gene in October 2002, and in April 2003, PRF led the announcement that Progeria is caused by a mutation of the gene LMNA, or Lamin A.” 90% of children with Progeria have a mutation on the gene that encodes Lamin A, a protein that holds the nucleus of the cell together. It is caused by a point mutation in position 1824 of the LMNA gene, replacing cytosine with thymine, creating an unusable form of the protein Lamin A. Lamin A is part of the building blocks of the nuclear envelope. It is believed that the defective Lamin A protein makes the nucleus unstable. This instability seems to lead to the process of premature aging among Progeria patients. Progeria appears to occur without cause - it is not seen in siblings of affected children. In extremely rare cases more than one child in the same family may have the condition[8,9,10]. Symptoms of Progeria Normal growth of a child slows down considerably in the initial year, though there is 117 normal motor development. The child looks old with narrowed face, conspicuous scalp veins and pinched nose. There is high risk of delayed tooth formation. Generally, the limbs shows fragility accompanied with joint stiffness. Listed below are some progeria symptoms: • • • • • • • • • • Premature and Rapid Aging Mental retardation Balding Beaked nose Thin skin Extreme growth delay begins at 9 months to 2 years of age Atherosclerosis Dwarfism Dental abnormalities Hip dislocation Other symptoms include acro-osteolysis with its components of hypo plastic facial bones and sinuses, open cranial structures and fontanelles, Wormian bones, and coxa valga. They are extremely short due to the growth failure, have acrocephaly, micrographic, dry scaly, thin skin, atrophy of muscles and a limited range of motion. One may want to seek immediate medical advice after noticing slow growth, hair loss and skin change in a child. Diagnosis of Progeria Due to a lack of specific laboratory tests at this current time, a diagnosis of progeria must be made on the physical appearance of the child. Diagnosis are usually made in the 1st or 2nd year of the child life when the characteristic skin changes and weight gain failure become apparent. Some of the things that are looked for upon thought of diagnosis are: 1. Skin changes similar to that seen in scleroderma (the connective tissue becomes tough and hardened) 2. Insulin resistant diabetes (diabetes that does not respond readily to insulin injections) 3. There may be early atherosclerosis of blood vessels leading to abnormal stress tests of the heart. 118 At present there are no specific tests that could be performed to diagnose this condition. There is only the physical examination diagnosis made based on the symptoms and signs that are observed during the examination. Along with the diagnosis comes the prognosis, and unfortunately that is associated with an extremely short lifespan. This is usually caused by complications with the heart, stroke, and myocardial infarction. International Journal of Pharmagenesis, 2(1) 2011 relaxes muscle fibers in blood vessels causing them to expand or dilate. This permits proper blood flow to affected areas, which enables cells and tissues to receive adequate amounts of the oxygen necessary for cell maintenance. Experimental Research Management Recent evidence suggested the benefit of giving nutritional therapy and growth hormone supplementation. The combination treatment of nutritional therapy and growth hormone supplementation demonstrated an increase in growth of Progeria patients, an increase in growth factors (chemicals which promote formation) within the blood, and a decrease in the patient’s basal metabolic rate. Basal metabolic rate is the minimum amount of energy (calories) that an individual needs to ingest on a daily basis in order to execute normal activities and tasks[13]. Growth Hormone Treatment has been Attempted In HGPS patients, the cell nucleus has dramatically aberrant morphology (bottom right) rather than the uniform shape typically found in healthy individuals (top right)[11,12]. Is Progeria Hereditary? Experts do not believe that Progeria is hereditary. They say it is due to a rare gene change which happens purely by chance. A non-twin sibling runs the same risk of having Progeria as any other child from another family. In about 1 in every 100 cases of HGPS the syndrome is passed down to the next generation within the same family. Treatment and Management There is presently no treatment for progeria. Support groups are available for the families of children with progeria. Treatment is symptomatic and aimed at providing psychological support. Palliative measures such as wearing a wig may be beneficial. Relief from chest pain due to changes in arteries can be accomplished by nitroglycerin. Nitroglycerin is a medication that A type of anticancer drug, the farnesyl transferase inhibitors (FTIs), has been proposed, but their use has been mostly limited to animal models. A Phase II clinical trial using the FTI Lonafarnib began in May 2007. Farnesyl transferase inhibitors (FTIs), currently used for treating cancer might reverse the nuclear structure abnormalities that are believed to cause Progeria. Studies carried out on mice with Progeria-like signs and symptoms showed that FTIs appeared to offer some improvements. Of the 13 mice treated with FTI, only one died during the 20-week UCLS study.[14, 15] Outlook (Prognosis) Progeria is associated with a short lifespan. The average patient survives to the early teens. However, some patients can live up to 30 years. The cause of death is usually related to the heart or a stroke as a result of the progressive atherosclerosis. Mental development is not affected. The development of symptoms is comparable to aging at a rate six to eight times faster than normal, although certain age-related conditions do not occur. Specifically, patients show no neurodegeneration or cancer predisposition. They do not develop “wear and A Review on Hutchinson-Gilford Syndrome “PROGERIA” tear” conditions commonly associated with aging, like cataracts and osteoarthritis years. Possible Complications[16] • • • Heart attack (myocardial infarction) Stroke Coronary artery blockage Progeria in India The disease which infects one in four lakh people is present in India too. Bisul khan and Razia Khatooon,’s family in Chhapra, Bihar; has seven children, of which five are Progeria patients. Out of the five, three daughters, Guriya, Rehana and Rubina are dead; having passed away at the ages of 17, 24 and 13 respectively. Two sons Ikramul (23) and Ali Hosain (22) are still alive, but their medical ages are 70 and 66. Two children Sanjita (21 year old) and Gulab Shah (7 year old) are normal. . Bisul Khan’s family in India is the ONLY FAMILY in the world that has more than one case of progeria. Conclusion While there is no treatment for progeria, according to the Progeria Research Foundation, there are steps parents and doctors can take to improve a child’s quality of life. For example, children with progeria often have poor appetites, and certain nutritional supplements, such as Pediasure and Boost, can help them get the nutrition and calories they need. This, in turn, can improve their mood, energy levels and skin and hair health. Likewise, physical or occupational therapy two to three times a week can help children stay active. Additionally, daily low-dose aspirin therapy may be recommended to prevent heart disease, as it is in at-risk adults. 119 References [1] Hutchinson J . “Case of Congenital Absence of Hair, with Atrophic Condition of the Skin and its Appendages, in a Boy whose Mother had been almost Wholly Bald from Alopecia Areata from the Age of Six”. Lancet 1886; 923. [2] Gilford H. “Ateleiosis and Progeria: Continuous Youth and Premature Old Age”. Brit. Med. J. 1904; 2; 914–8. [3] James, William; Berger, Timothy; Elston, Dirk. Andrews’ Diseases of the Skin: Clinical Dermatology (10th ed.). Saunders, 2005; 574. [4] Rapini, Ronald P.; Bolognia, Jean L.; Jorizzo, Joseph L. Dermatology: 2-Volume Set. St. Louis: Mosby, 2007; 762. [5] Ewell Steve Roach & Van S. Miller (2004), Neurocutaneous Disorders. Cambridge University Press, 2004; 150. [6] Kwang-Jen Hsiao. Advances in Clinical Chemistry: 33. Academic Press, 1998; 10. [7] The Progeria Research Foundation Homepage http:// www.progeriaresearch.org/ Last Updated: 12/26/2002 Copyright (c) 1999 The Progeria Research Foundation, Inc. [8] De Sandre-Giovannoli A., Bernard R., Cau P., Navarro C., Amiel J., Boccaccio I., Lyonnet S., Stewart C. L., Munnich A., Le Merrer M., Levy N. Lamin a Truncation in Hutchinson-Gilford Progeria. Science. 2003; 300, (5628): 2055. [9] Eriksson M., Brown W. T., Gordon L. B., Glynn M. W., Singer J., Scott L., Erdos M. R., Robbins C. M., Moses T. Y., Berglund P., Dutra A., Pak E., Durkin S., Csoka A. B., Boehnke M., Glover T. W., Collins F. S. Recurrent de novo point mutations in lamin A Cause HutchinsonGilford Progeria Syndrome. Nature. 2003; 423(6937): 293-8. [10] Goldman R. D., Shumaker D. K., Erdos M. R., Eriksson M., Goldman A. E., Gordon L. B., Gruenbaum Y., Khuon S., Mendez M., Varga R., Collins F. S. Accumulation of Mutant Lamin A Causes Progressive Changes in Nuclear Architecture in Hutchinson-Gilford Progeria Syndrome. Proc Natl Acad Sci U S A. 2004; 101(24): 8963-8. [11] Korf B. “Hutchinson-Gilford Progeria Syndrome, Aging, and the Nuclear Lamina”. N. Engl. J. Med. 2008; 358(6): 552–5. Parents and children with progeria are hopeful that the future will bring therapies that treat the underlying genetic abnormalities. [12] Merideth M. A., Gordon L. B., Clauss S., et al. “Phenotype and Course of Hutchinson-Gilford Progeria Syndrome”. N. Engl. J. Med. 2008; 358 (6): 592– 604. As for the prevention of heart disease in children with progeria, the next step in research will be to understand the relationship between the lamin A protein and HDL cholesterol levels. Such research, she believes, could have “huge implications for everybody.” [13] Varela I., Pereira S., Ugalde A. P., et al. “Combined Treatment with Statins and Aminobisphosphonates Extends Longevity in a Mouse Model of Human Premature Aging”. Nat. Med. 2008; 14 (7): 767–72. [14] Sadeghi-Nejad A., Demmer L. “Growth Hormone Therapy in Progeria”. J. Pediatr. Endocrinol. Metab. 2007; 20 (5): 633–7. 120 [15] Meta M., Yang S. H., Bergo M. O., Fong L. G., Young S. G. “Protein Farnesyltransferase Inhibitors and progeria”. Trends Mol Med 2006; 12 (10): 480–7. International Journal of Pharmagenesis, 2(1) 2011 [16] Brown W. T. Progeria. In: Kliegman R. M., Behrman R. E., Jenson H. B., Stanton B. F., eds. Nelson Textbook of Pediatrics. 18th Ed. Philadelphia, Pa: Saunders Elsevier; 2007: chap 90.