Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Polysubstance dependence wikipedia , lookup
Pharmacognosy wikipedia , lookup
Neuropharmacology wikipedia , lookup
Prescription drug prices in the United States wikipedia , lookup
Pharmaceutical industry wikipedia , lookup
Drug design wikipedia , lookup
Drug interaction wikipedia , lookup
Drug discovery wikipedia , lookup
Prescription costs wikipedia , lookup
Pharmacokinetics wikipedia , lookup
Pharmacogenomics wikipedia , lookup
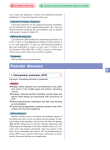
terbinafine Severe Generalized Pustular Psoriasis Provoked by Oral Terbinafine Jeng-Wei Tjiu Tsen-Fang Tsai Chia-Yu Chu Terbinafine is an allylamine antifungal agent. Its severe cutaneous adverse effects are rare, but toxic epidermal necrolysis, pustular drug eruption, acute generalized exanthematous pustulosis, Stevens-Johnson syndrome, and erythema multiforme had been reported. Terbinafine was also reported to induce flare-up of chronic psoriasis or development of pustular psoriasis. Here we report a psoriatic patient who developed pustular eruptions in four weeks after treatment with terbinafine for his presumptive tinia unguium without a definitive mycological evidence. The skin eruptions progressed to severe, generalized pustular psoriasis in the following two weeks even though he discontinued terbinafine treatment. It is well recognized that terbinafine may aggravate and induce psoriasis. Terbinafine is a highly effective antifungal agent. However, with the indiscriminate use, terbinafine may cause unnecessary risk, as in our patient. With the increased systemic administration of terbinafine, severe adverse effects might become more common. Therefore, we suggest mycological examinations are essential prior to commencing terbinafine therapy for suspected onychomycosis. (Dermatol Sinica 22 : 187-192, 2004) Key words: Terbinafine, Pustular psoriasis Terbinafine Stevens - Johnson Terbinafine terbinafine Terbinafine terbinafine Terbinafine terbinafine terbinafine terbinafine ( 22 : 187 - 192, 2004 ) From the Department of Dermatology, National Taiwan University Hospital, Taipei, Taiwan Accepted for publication: January 30, 2004 Reprint requests: Chia-Yu Chu, M.D., Department of Dermatology, National Taiwan University Hospital, No. 7, Chung-Shan South Road, Taipei 100, Taiwan, R.O.C. TEL: 886-2-23562141 FAX: 886-2-23934177 187 INTRODUCTION Terbinafine is an allylamine fungicidal agent widely used for the treatment of onychomycoses and other dermatophyte infection. Adverse effects occur in 10.4% of the patients, with cutaneous side-effects in 1.8%.1 The cutaneous adverse effects reported with terbinafine include erythema multiforme,2, 3 toxic epidermal necrolysis / Stevens - Johnson syndrome,4 - 6 fixed drug deruption,7 acute generalized exanthematous pustulosis ( AGEP ),8 - 13 erythema annulare centrifugum - like psoriatic drug eruption. 14 Terbinafine has recently been linked to flaring of stable chronic plaque psoriasis 15 - 17 and the development of pustular psoriasis. 15, 18-20 We report a further case of severe pustular psoriasis provoked by the oral administration of terbinafine. Fig. 1A Generalized pustular eruptions on erythematous, edematous plaques CASE REPORT A 59-year-old man had a 10-year history of localized pustular psoriasis involving his finger and toe nails as well as bilateral palms. There is no papular or plaque lesions on the trunk, extremities and scalp. He had no known drug allergy history before. None of his family member suffered from psoriasis. Onychomycosis had been diagnosed clinically by a general practitioner and he was treated with terbinafine 250 mg daily. No other skin lesion was noted at Fig. 2 Fig. 1B Close-up showing pustules on an erythematous background. 188 Histological examinations showed hyperkeratosis and parakeratosis with subcorneal and intraepidermal spongiotic pustules filled with neutrophils (H & E, x200). Dermatol Sinica, June 2004 terbinafine that time. No mycological investigations were performed. Terbinafine was discontinued four weeks later due to development of pustular eruptions. Terbinafine aggravated pustular psoriatic eruption was diagnosed. He was treated with oral antihistamine, potent topical corticosteroid and Calcipotriene ointment. The skin lesions progressed with diffuse erythematous macular eruption. Two weeks after onset of symptoms, the generalized, bright - red, symmetric plaques studded with flaccid pustules developed ( Fig. 1 ). Pus lakes formed on the trunk, thighs and arms. There was exfoliation of skin in some areas. His finger and toe nails showed irregular pitting, salmon patches of the nail bed, onycholysis with an erythematous border, but no evident whitish discoloration of the nail plate or subungual hyperkeratosis. He was admitted to our hospital two weeks after onset of the symptoms. On admission, he was acute illness looking with high fever ( 39˚C ). He had a widespread pustular eruption. Routine investigations showed a raised white cell count ( 22.68 x 10 9 / L, normal range 4 - 10 x 10 9 / L ), segments 81 %, banded neutrophils 2 %, lymphocytes 14 %, hyperbilirubinemia ( serum bilirubin 1.67 mg / dL, normal range: < 1 mg / dL) and slightly elevated liver enzyme ( aspartate aminotransferase 48 U / L, normal 0 - 35 U / L; alanine aminotransferase 88 U / L, normal < 40 U / L ). Anti-streptolysin O titer and immunoglobulin A were normal. Bacterial culture of the pustules was negative and a skin biopsy was made. Histopathological examinations showed several subcorneal neutrophil - rich pustules and also neutrophilic and lymphocytic infiltration in the upper dermis with spongiosis and mild dermal edema. It was consistent with a pustular psoriasis (Fig. 2). He was treated with acitretin 20 mg daily initially and the dose was increased gradually to 40 mg daily. Betamethasone dipropionate cream was applied twice daily. The pustules subsequently dried up and desquamated. One month after the treatment, the erythema faded and the skin was clear. The hospital course was complicated with pneumonia of nosocomial ori- Dermatol Sinica, June 2004 gin methicillin-resistant Staphylococcus aureus ( MRSA ) with empyema. He was treated with surgical drainage and intravenous vancomycin for 2 weeks and was discharged after recovery. Two months after recovery, patch tests were performed with European standard series; 5 %, 10 %, 50 %, and without dilution of terbinafine in petrolatum. Patch test reading and interpretation followed the International Contact Dermatitis Research Group ( ICDRG ) scoring system. In the ICDRG scoring system, 1+ represents erythema and edema; 2+ represents erythema, edema and vesicles, 3+ represents an extreme reaction with bullous formation.21 At the 72 hours reading, the result showed an ICDRG 1+ reaction to undiluted terbinafine. All other patch testing gave negative results. DISCUSSION Terbinafine is an antifungal agent that is effective for the oral treatment of dermatophytes causing onychomycosis and other dermatomycoses. Oral terbinafine causes adverse effects in 10.4 % of patients.22, 23 In a post marketing surveillance study performed in a cohort in the U.K. (n = 10,361 patients), dermatological medical events were reported by 341 ( 3 % ) of the patients.24 Most reactions were mild to moderate rashes occurring in the first 2 weeks and resolving within 2 - 3 weeks after discontinuation of terbinafine or despite continued treatment. The most common cutaneous adverse effects associated with oral terbinafine are rash, pruritus and urticaria. Generally, these manifestations are not severe, requiring discontinuation of therapy in only 1% of patients.22 With the increasing use of oral antifungal agents, it is likely that severe cutaneous adverse effects will be recognized with a greater frequency. Less common cutaneous adverse effects reported with terbinafine include erythema multiforme,2, 3 toxic epidermal necrolysis / Stevens - Johnson syndrome,4 - 6 fixed drug deruption, 7 erythema annulare centrifugum-like psoriatic drug eruption,14 and pustular psoriasiform eruption.19 Recently, there are several reports linking terbinafine therapy with development of psoriasis de novo15 or worsening 189 Table I. Differentiation between AGEP and pustular psoriasis History of psoriasis Causation Onset Duration Systemic symptoms Clincical appearance Histology AGEP 8-13 Possible Usually drug Shorter, < 1 week or weeks Cleared spontaneously within 15 days High fever, leukocytosis, seldom arthralgia Erytheroderma with nonfollicular sterile pustules, predominance in the folds. Spongiform subcorneal/ intraepidermal pustules,papillary dermal edema, vasculitis, exocytosisof eosinophils, single-cell necrosis of keratinocyts. of pre-existing psoriasis.15-18 Terbinafine is also reported to induce acute generalized exanthematous pustulosis 8-13 and one case was confirmed by a positive patch-test result.13 The differential diagnosis of terbinafineindcued pustular eruption may include druginduced or drug-aggravated pustular psoriasis,1518 AGEP,8-13, 25, 26 or subcorneal pustular dermatosis (Snedden-Wilkinson disease),27 pustular vasculitis,28 IgA pemphigus, drug hypersensitivity syndrome,29 and infections ( i.e. bacterial folliculitis, impetigo ). AGEP is characterized by extensive formation of both follicular and nonfollicular sterile pustules on an erythematous background combined with fever and peripheral blood leukocytosis. 25 Five criteria have been suggested for the definition of AGEP: a numerous small, non-follicular pustules arising on edematous bases; b the pathological demonstration of intraepithelial or subcorneal pustules associated with one or more of the followings: dermal edema, vasculitis, perivascular eosinophils; c fever > 38˚C; d blood neutrophil count above 7 x 109 / L; e acute course with spontaneous resolution in 15 days.25 AGEP and pustular psoriasis of the von Zumbusch type have indistinguishable morphology. There are still no clear-cut rules for the differentiation of both entities until now. Table I is a summary of differences between pustular psoriasis and AGEP. The patient had a clinical course longer than 15 days, no spontaneous resolution of pus- 190 Pustular psoriasis 15,18-20 Mostly Infection>drug Longer, <1 week to years. Longer, can be recalcitrant or relapse Often fever, leukocytosis, often arthralgia (~30%) Generalized pustules on erythematous plaques, may have nail change, more generalized. Subcorneal/intraepidermal pustules, papillomatosis, acanthosis, elongated rete, parakeratosis. tules, despite early discontinuance of the offending drug. His psoriatic history and response to retinoid therapy also favor the diagnosis of generalized pustular psoriasis rather than AGEP. Subcorneal pustular dermatosis is characterized by larger flaccid blisters with hypopyon formation often arranged in a circinate distribution pattern. 27 Pustular vasculitis is a variant of leukocytoclastic vasculitis which is characterized by the development of many small pustules localized mainly on the dorsa of hands.28 Drug hypersensitivity syndrome, also called drug rash with eosinophilia and systemic symptoms (DRESS) may also show pustules. But it often presents with eosinophilia, mononucleosis, and more severe visceral involvement.29 The negative bacterial culture and sterile pustules did not support infection as a cause of the skin lesions. Reviewing the clinical course and histopathologic findings, all the above diagnosis except pustular psoriasis are not likely in this patient. In AGEP, the formation of sterile pustules with neutrophil aggregation may be caused by drug specific T cells. These T cells secrete high amount of interleukin - 8, now also known as CXC chemokine ligand 8 (CXCL8).30 Drug specific T cells from the blood and skin are activated and cytotoxic. Perforin / granzyme B and Fas / FasL - mediated mechanism cause tissue destruction and formation of vesicles. CXCL8 released from T cells and keratinocytes attracts neutrophils to the vesicles and transform them Dermatol Sinica, June 2004 terbinafine to pustules.31 In drug induced pustular psoriasis, similar mechanisms may be involved in the pathogenesis of pustules. Drug specific T cells in pustular psoriasis may release acute phase cytokines, including IL-1, IL-6, CXCL8, and TNF-α, that trigger flare-up of psoriasis and formation of generalized pustules. The latency periods between the administration of different drugs and the exacerbation or de novo appearance of psoriasis had been summarized by Gupta et al.15 The latency period of terbinafine and nonsteroidal anti-inflammatory drugs are denoted short ( less than 4 weeks ); antimalarials and angiotensin converting enzyme inhibitors are intermediate (4-12 weeks); lithium and beta-blockers are long (more than 12 weeks).15 Using systemic challenge test to identify an offending drug in an suspected drug allergic patient is unethical and sometimes dangerous. Patch testing may be used as an alternative way to identify the possible drug induced reactions. The role of patch testing in confirming the causative agent of AGEP has been well recognized in recent years.32 Wolkenstein et al. have shown a 50 % sensitivity of patch testing in cases of AGEP.32 In terbinafine-induced AGEP, patch testing was reported to be positive by Kempinaire et al.13 Therefore, some cases of drug-induced generalized pustular eruption could be due to type 4 reactions. We performed patch testing in this case because of the similarity between AGEP and generalized pustular psoriasis both clinically and histopathologically. Although the role of patch testing in most cases of drug eruption is uncertain, the positive reaction to terbinafine in our case suggests that delayed type hypersensitivity could play a role in the pathogenesis of drug-induced generalized pustular psoriasis as has been described previously.33 With the increasing administration of oral antifungal agents, it is likely that severe cutaneous adverse effects will be recognized with a greater frequency. This should be taken into account when prescribing terbinafine for suspected onychomycosis without definite myco- Dermatol Sinica, June 2004 logical evidence. In addition, the use of systemic antifungal agents makes interpretation of subsequent mycological investigation difficult. We propose fungal examinations be essential before starting oral terbinafine for suspected onychomycosis. REFERENCES: 1. Villars VV, Jones TC: Special features of the clinical use of oral terbinafine in the treatement of fungal diseases. Br J Dermatol 126 (Suppl. 39): 6169, 1992. 2. McGregor JM, Rustin MHA: Terbinatinfe and erythema multiforme. Br J Dermatol 131: 587-588, 1994. 3. Todd P, Halpern S, Munro DD: Oral terbinafine and erythema multiforme. Clin Exp Dermatol 20: 247-248, 1995. 4. Carstens J, Wendelboe P, Sogaard H, et al.: Toxic epidermal necrolysis and erythema multiforme following therapy with terbinafine. Acta Derm Venereol [Stockh] 74: 391-392, 1994. 5. White SI, Bowen-Johns D: Toxic epidermal necrolysis induced by terbinafine in a patient on longterm anti-epileptics. Br J Dermatol 134: 188-189, 1996. 6. Rzany B, Mockenhaupt M, Gehring W, et al.: Stevens-Johnson syndrome after terbinafine. Arch Dermatol 30: 509, 1996. 7. Munn SE, Russell Jones R: Terbinafine and fixed drug eruption. Br J Dermatol 133: 815-816, 1995. 8. Dupin N, Gorin I, Djien V, et al.: Acute generalized erythematous pustulosis induced by terbinafine. Arch Dermatol 132: 1253-1254, 1996. 9. Lombardo M, Cerati M, Pazzaglia A: Acute generalized exanthematous pustulosis induced by terbinafine. J Am Acad Dermatol 49: 158-159, 2003. 10. Taberner R, Puig L, Gilaberte M, et al.: Acute generalized exanthematous pustulosis induced by terbinafine. Eur J Dermatol 13: 313-4, 2003. 11.Condon CA, Downs AMR, Archer CB: Terbinafine-induced acute generalized exanthematous pustulosis. Br J Dermatol 138: 709-710, 1998. 12. Hall AP, Tae B: Acute generalized exanthematous pustulosis associated with oral terbinafine. Austral J Dermatol 41: 42-45, 2000. 13. Kempinaire A, De Raeve L, Merckx M, et al.: Terbinafine-induced acute generalized exanthema- 191 tous pustulosis confirmed by a positive patch-test result. J Am Acad Dermatol 37: 653-655, 1997. 14. Wach F, Stolz W, Rudiger R, et al.: Severe erythema annulare centrifugum-like psoriatic eruption induced by terbinafine. Arch Dermatol 131: 960961, 1995. 15.Gupta AK, Sibbald Rg, Knowles SR, et al.: Terbinafine therapy may be associated with the development of psoriasis de novo or its exacerbation: four case reports and a review of druginduced psoriasis. J Am Acad Dermatol 36: 858862, 1997. 16.Gupta AK, Lynde CW, Lauzon GJ, et al.: Cutaneous adverse effects associated with terbinafine therapy: 10 case reports and a review of the literature. Br J Dermatol 138: 529-532, 1998. 17. Tsankov N, Angelova I, Kazandjieva J: Drug induced psoriasis recognition and management. Am J Clin Dermatol 1: 159-165, 2000. 18. Wilson NJ, Evans S: Severe pustular psoriasis provoked by oral terbinafine. Br J Dermatol 139: 168, 1998. 19. Papa CA, Miller OF: Pustular psoriasiform eruption with leukocytosis associated with terbinafine. J Am Acad Dermatol 39: 115-117, 1998. 20. Bennett ML, Jorizzo JL, White WL.: Generalized pustular eruptions associated with oral terbinafine. Int J Dermatol 38: 596-600, 1999. 21. Rietschel RL, Fowler JF Jr.: Fisher's contact dermatitis, 5th edn. Philadelphia: Lippincott Williams & Wilkins, 9-26, 2001. 22. Gupta AK, Sauder DN, Shear NH: Antifungal agents: an overview. Part II. J Am Acad Dermatol 30: 911-933,1994. 23. Shear NH, Gupta AK: Terbinafine for the treatment of pedal onychomycosis: a foot closer to the promised land of cured nails. Arch Dermatol 131: 937-942, 1995. 192 24. O'Sullivan DP, Needman CA, Banges A, et al.: Postmarketing surveillance of oral terbinafine in the UK: report of a large cohort study. Br J Clin Pharmacol 42: 559-565, 1996. 25. Roujeau JC, Bioulac-Sage P, Bourseau C, et al.: Acute generalized exanthematous pustulosis. Analysis of 63 cases. Arch Dermatol 127: 13331338, 1991. 26. Sidoroff A, Halevy S, Bavinck JNB, et al.: Acute generalized exanthematous pustulosis (AGEP)-A clinical reaction pattern. J Cutan Pathol 28: 113119, 2001. 27. Mandel EH, Gonzales V.: Subcorneal pustular dermatosis (Sneddon-Wilkinson). Arch Dermatol 99:246-247, 1963. 28. Strutton G, Weedon D, Robertson I.: Pustular vasculitis of the hands. J Am Acad Dermatol 32:192198, 1995. 29. Descamps V, Valance A, Edlinger C, et al.: Association of human herpesvirus 6 infection with drug reaction with eosinophilia and systemic symptoms. Arch Deramtol 137: 301-304, 2001. 30. Britschgi M, Steiner UC, Schmid S, et al.: T-cells involvement in drug-induced acute generalized exanthematous pustulosis. J Clin Invest 107: 14331441, 2001. 31. Schmid S, Kuechler PC, Britschgi M, et al.: Acute generalized exanthematous pustulosis: role of cytotoxic T cells in pustule formation. Am J Pathol 161: 2079-2086, 2002. 32. Wolkenstein P, Chosidow O, Flechet M-L, et al.: Patch testing in severe cutaneous adverse drug reaction including Stevens-Johnson syndrome and toxic epidermal necrolysis. Contact Dermatitis 35: 234-236, 1996. 33. Whittam LR, Wakelin SH, Barker JN: Generalized pustular psoriasis or drug-induced toxic pustoloderma? The use of patch testing. Clin Exp Dermatol 25: 122-124, 2000. Dermatol Sinica, June 2004