Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
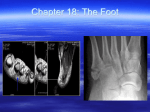
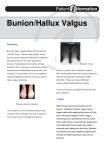
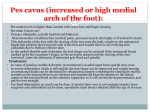
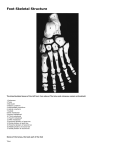
Primary function of the foot • Transfer load through multiple planes during multiple movements. Propels the body forward during the gait cycle anatomy and motor control • Significant anatomical variations make it hard to completely define normal. Currently limited evidence for motor control in the forefoot particularly of the intrinsic muscles Divisions of the foot: Divisions of the foot: Rear foot • Includes the talus and calcaneus with the talus resting on the anterior aspect of the calcaneus. Midfoot Forefoot • Includes 5 metatarsal bones with base, shaft and head. • Metatarsal heads bear the greatest load in the forefoot • The phalanges make up the toes with the hallux having two and the other toes having 3 • The cuneiforms and navicular located medially • Beneath the big toe joint bones called sesamoids • Cuboid located laterally • Hallux has 2 joints Metatarsophalangeal and hallux interphalangeal joint • Separating the midfoot from the forefoot is the lisfranc complex of ligaments. • Other toes have 3 joints proximal and distal interphalangeal joints Arches of the foot: Medial Longitudinal arch • Runs between the calcaneus, talus, medial cuneiform and 1st metatarsal. • Navicular key stone of the arch. • Passive stability predominately from plantar fascia Arches of the foot: Transverse arch • Forefoot: 5 metatarsal heads, keystone is the 2nd metatarsal head • Relatively weak inter-metatarsal ligaments for support Lateral Longitudinal arch • Calcaneus, cuboid (key stone) and 5th metatarsal Muscles of the foot: Muscles of the foot: Medial Longitudinal arch Medial Longitudinal arch The muscles that can influence the MLA are: Tibialis Posterior: •Tibialis Posterior •9 •Tibialis Anterior •Flexor Digitorum Longus •Abductor Hallucis •Flexor Digitorum Brevis insertions ~ navicular tuberosity, plantar medial cuneiform, intermediate, and lateral cuneiform, cuboid and the BASE of the second, third and fourth metatarsals. •Aids in control of pronation from heel strike to mid stance. Muscles of the foot: Muscles of the foot: Medial Longitudinal arch Medial Longitudinal arch Tibialis anterior: Abductor hallucis: Note the attachment to medial aspect of the medial cuneiform and base of 1st metatarsal. •Medial and lateral plantar nerves running through muscle can cause neuroma type symptoms. •Lies along medial border of the foot. Flexor digitorum longus: •Medial to tibialis posterior •Note the attachment of the FDL tendon to the quadratus plantae muscle in the foot inserting to the bases of the last phalanges of toes 2 to 5. •It flexes the toes and is a weak plantar flexor. Flexor Hallucis Brevis: •Originates divides into a medial and lateral part which contain the medial and lateral sesamoids respectively. Muscles of the foot: Lateral longitudinal arch Peroneus longus: •Note the insertion into the lateral side of the base of the first metatarsal bone and the lateral side of the medial cuneiform. •Stabilizes the medial cuneiform and first metatarsal for toe off part of the gait cycle. Peroneus Brevis: •Sits medial to PL and attaches to the base of the fifth metatarsal •Plantar flexor and inverter of the foot Abductor digiti minimi: •Lies along the lateral border of the foot. from medial part of the cuboid. •It Muscles of the foot: Transverse arch Adductor Hallucis: •Two heads oblique head crosses the foot obliquely occupying the space under the first, second, third and fourth metatarsal bones •The •Originates from the bases of the above metatarsals and together with the lateral portion of flexor hallucis brevis inserts onto the lateral aspect of the base of the first phalanx of the greater toe. transverse head originates from the plantar metatarsophalangeal ligaments of the third, fourth and fifth toes inserting with the oblique head. •The Assessment: Assessment: Standing assessment: Standing assessment: • Good place to start as meaningful task or problem movement will involve weight bearing. • Cuboid, slide of 5th metatarsal base, next bone is cuboid. • Cuneiforms can be found by coming just off the navicular tuberosity anteriorly and in line with the cuboid. • Start posteriorly and look at position of calcaneus. Inverted, everted or neutrally aligned? • Neck of the talus centered or medially/ laterally deviated? • The second metatarsal articulates with the intermediate cuneiform and the third with the lateral cuneiform. • Navicular tuberosity down from neck of talus • 4th and 5th metatarsals articulate with the cuboid. • Medial cuneiform slide off 1st metatarsal ? rigid or some small joint play? • Does the 1st MTP weight bear evenly or is there excessive force or no force? • Same with the 5th? Assessment: Assessment: Jacks test: • How much 1st MTP joint extension is there? 65 degrees extension optimal for toe off • Knee alignment • Hip position 1 leg stand / step through: Foot: • Should pronate slightly on 1 leg stand or step through. • The calcaneus everts • The talus slightly internally rotate within the ankle mortise • The rest of the medial column should slightly oppose the direction of the talus into external rotation • Pelvis • The phalanges remain extended and relaxed • Thorax • Movement should look smooth with no rigidity • Abnormal movements include excessive pronation, medial column following talus, supination of foot, toe gripping, excessive weight bearing or minimal weight bearing through 1st ray • Look at timing with failed load transfer of hip, pelvis and thorax Assessment: 1 leg stand / step through: Toe off: • Foot should move into supinated position for maximum stability • The calcaneus should invert further challenge the foot: Balance pad excellent real time feedback for patient. Accentuates areas of failed load transfer. • The talus should glide into slight external rotation in the ankle mortise. • The rest of the lateral column should also externally rotate to lock the lateral column. • The 1st MT should internally rotate and plantar flex • Abnormal movements can include pronation, inability of the 1st metatarsal to remain plantar flexed and internally rotated. Assess with orthotics and shoes also to assess effectiveness of both. active movements passive movements Muscle length tests: •Ankle: plantarflexion and dorsiflexion looking for asymmetry •Rear foot: range of inversion and eversion at the sub talar joint •Midfoot: range of pronation/ supination •Toes: range of MTP planatarflexion and dorsiflexion especially 1st MTP extension (min 65 degrees) •Tibialis posterior (DF/EV) •Tibialis anterior (PF/EV) •Peroneus Longus (DF/INV) •FHL/FHB DF/1st MTP extension versus 1st MTP extension •FDL (Ankle DF and MTP extension) •Gastrocnemius/ •Palpate Soleus Dorsiflexion versus Dorsiflexion with knee flexion muscle bellies and compare with non restricted side to strengthen hypothesis. Muscle strength •Peronei: •Tibialis •Tibialis eversion and plantar flexed posterior: plantarflexion and inversion anterior: Dorsiflexion and eversion •Lumbricals: Keeping ends of toes straight point toes into ground without toe scrunching. Compare with good side. Key Points: Restriction of joint movement within the foot may be associated with one or more muscles (muscular compression rather than true joint fixation) Muscular dysfunction is not always apparent with standard muscle testing procedures. These tests sometimes don’t pick up subtle changes in muscle tension. Palpation of muscle tone with good side will tell you more. Use your hands to feel the foot during functional tasks. Everyone is different and everyone’s combinations of hypertonic muscles will be different. So assess good side as well. Forefoot disorders: Hallux Limitus Most forefoot disorders are: •Defined •Goal • An overload injury due to failed load transfer in the mid or rear foot or rest of the body • Training error of too much mileage to soon • New shoes or prolonged use of ill fitting shoes eg high heel Jimmy Choo’s with narrow toe box. as a restriction in dorsiflexion of less than 65 degrees first MTP joint. is to prevent Hallux Rigidus. Caused by •Failed load transfer of the kinetic chain leading to a loss of the MLA causing over use of the intrinsic hallux muscles, compression of the 1st MTP joint and its passive restraints •Hypermobile 1st ray from previous trauma to the passive system or genetics. Clinical features •Pain around the first metatarsophalangeal joint. •Aggravated by walking and especially toe off and narrow toe box Hallux valgus Hallux Limitus •Genetic disorder characterized by a varus deviation of the 1st metatarsal and valgus deviation of the first phalange Examination findings •Often bony extotosis and associated overlying chronic thickening of the bursa and occasionally acute bursitis. •Hallux limitus •The location of maximum tenderness is the first •Windlass mechanism is disrupted and sesamoids pulled laterally disrupting flexor pull metatarsophalangeal joint, especially dorsally and there may be bone spurs present. •Caused by •X-ray may reveal degenerative OA. •Tightness and trigger points in FHL, FHB, Abductor and •Genetics, narrow toe box and high heel. •Poorly fitting shoes such as a very narrow toe box especially with heels •Hypermobile foot and excessive pronation increases pressure on the medial border of the adductor hallucis. hallux and medial capsular structures Sesamoid injuries Hallux Limitus Clinical features •Often asymptomatic •Pain can develop medially over time again with prolonged use of inappropriate shoes or acutely with a new pair of shoes with narrow toe box. •Medial sesamoid slightly larger and more commonly injured sesamoid due to taking more load during gait cycle •The sesamoids role is to protect the tendon of flexor hallucis longus, absorb most of the weightbearing on the medial aspect of the forefoot and increase the mechanical advantage of the intrinsic muscles of the hallux. Likened to the patella of the knee. •Portions of the adductor and abductor hallucis also insert on the sesamoids. •In Examination findings •Obvious •With deformity or without acute bursitis •Adductor halluces trigger points in either head 30% of people bipartite or two part sesamoid may be present. ? alterations in the pull of hallux tendons with bipartite sesamoid. Common to see this in patients presenting with sesamoid pain. Caused by •Common •Injuries in endurance athletes or athletes who play change of direction sports. include stress fractures, traumatic fracture , inflammation or osteonecrosis around the sesamoid. Sesamoid injuries Sesamoid injuries Clinical features Investigations •The •Get axial view x-ray to exclude a fracture •Get MRI so you know exactly what you are dealing with. MRI can detect whether you are pain associated with sesamoid disorders variable from generalized joint pain to affected sesamoid or whole sesamoid complex. •Pain with weight bearing through the forefoot particularly at toe off when the hallux is at full extension. •Present walking on lateral border of foot to avoid weight bearing through the 1st MTP joint. •Occasionally describe clicking under the 1st MTP joint. Metatarsophalangeal joint synovitis (metatarsalgia) managing a stress fracture, a bipartite sesamoid sprain or inflammation. Examination findings •Tenderness to palpation of sesamoid involved and visible swelling •Trigger points in FHB, FHL, ABDUCTOR or adductor halluces •Loss of 1st MTP extension with or without pain or clicking •FLT ankle or midfoot common Metatarsophalangeal joint synovitis (metatarsalgia) Metatarsalgia generic term for dysfunction to the second, third, fourth or fifth metatarsophalangeal joints or metatarsal heads. Examination findings Caused by •A drop in the transverse arch distally, •callous formation over the effected met heads, •Tenderness over the MTP joint or Met head •Passive extension of the toes will hurt or be restricted when comparing to the other side. •Flexor digitorum brevis and longus if unopposed by the lumbricals, will cause extension at •Often related to extremes in foot type such as pes planus or cavus (high arch) •Hyper mobile foot type •Failed load transfer throughout kinetic chain •It can be caused by overactivity of FDL and FDB seen with Toe gripping/ clawing •It can also be caused by tight toe extensors Clinical features Pain is usually associated with weight bearing especially mid stance and toe off. the MTP joints so clinically may find excessive FDB and FDL tone and an inability to activate the lumbricals •Normally always has tight EDL, EDB or dorsal interossei check all. Metatarsophalangeal joint synovitis (metatarsalgia) Examination findings •The lumbricals originate from the toe flexor tendons and insert onto the dorsal extensor tendons. It assists in flexion of the MTP joints and extension of the interphalangeal joints. •Imbalance between the two will extend the MTP joints and aggravate the forefoot. •Interossei dorsal and plantar ab and adduct the metatarsals however they have connections with the ligaments however have a slip with peroneus longus. Dysfunction in peroneus longus may irritate or create dysfunction forcing the metatarsals plantarly. •Hallux limitus common causing increased loading of MTP joints Morton’s neuroma •Not really a true neuroma. Due to the same problems as for metatarsalgia you can get swelling and scar tissue build up around the interdigital nerves between the metatarsals. Pain can radiate into the toes with pins and needles or numbness. •And again is aggravated by narrow shoes and forefoot running. •Entrapment site of nerve is intermetatarsal ligament and bursa •Caused again by 1st MT dysfunction causing increased loading of MTP joints, 2,3,4