Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
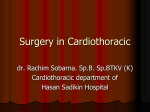
Le Infezioni in Medicina, n. 2, 174-177, 2015 174 Caso clinico / Case REPORT Salmonella paratyphi B mycotic aneurysm of the abdominal aorta in an HIV-infected patient: a case report Caso clinico di aneurisma micotico da Salmonella paratyphi B dell’aorta addominale in un paziente HIV positivo Nicolò Girometti1, Maddalena Giannella1, Stefano Brocchi2, Lorenzo Badia1, Leonardo Calza1, Pierluigi Viale1 Department of Medical Sciences and Surgery, Section of Infectious Diseases, University of Bologna, S. Orsola-Malpighi Hospital, Bologna, Italy; 2 Operative Unit of Radiology, University of Bologna, S. Orsola-Malpighi Hospital, Bologna, Italy 1 A ortic infection complicated by a mycotic aneurysm is a rare life-threatening event that progresses rapidly. Traditionally, antibiotic therapy is not sufficient and surgical repair is essential to prevent aneurysm [1]. Here is reported the story of a 49-year-old man with a poor control of his multi-resistant HIV infection diagnosed in 1990 after a short course of intravenous drug abuse, presented to the local HIV outpatient clinic with non-specific complaints consistent with urinary tract infection. Seven years prior to admission he was diagnosed for a Mycobacterium avium complex pancreatic infection with extensive abdominal lymphoadenopathy that required a 6 months treatment course of rifabutin, ethambuthol, and moxifloxacin. His last laboratory tests performed 10 days earlier revealed a CD4 blood-cell count of 107/mm3 accounting for a 4% of total lymphocytes and viral load of 1089135 copies/mL. The patient was on a maraviroc + boosted darunavir HAART regimen because of CCR-5 positivity and a viral history of multiple virological failures and development of resistances to all NRTIs, NNRTIs and PIs with the exception of darunavir. The patient admitted a poor compliance to the current HAART regimen because of personal issues during the past 4 months. Corresponding author Nicolò Girometti E-mail: [email protected] He reported a 7-day history of frequent urine passing, febrile chills and a dull left lumbar pain. At time of examination pain radiating to the left inferior abdomen quadrant, and left groin were present, abdomen was soft and not tender, while heart and lungs examination were normal. No joint pains or skin findings were observed. Mental status and neurological exam were normal. The patient was normotensive with a rhythmic pulse of 102 beats per minute and febrile (37.8°C) and he was admitted to the hospital with a presumptive diagnosis of urinary tract infection. Initial laboratory blood tests on that day showed increased white blood cells count (9760/mm3), a moderate anaemia (Hb 10.1 g/dL), elevated procalcitonin (0.4 ng/ml) and C-reactive protein (11.4 mg/dL). Transaminases were only slightly elevated and alkaline phosphatase was normal. Urine analyses were not significant for a urinary tract infection and an abdomen ultrasound was negative for hydronephrosis, renal stones or other kidney abnormalities. The patient was empirically started on piperacillin/tazobactam (13.5g/die) administered by continuous infusion after blood cultures were performed. 120 minutes later blood cultures analyzed by matrix-assisted laser, desorption/ ionization-time of flight (MALDI-TOF) mass spectrometry were positive for Salmonella paratyphi B. After 12 hours the patient was still febrile and feeling very unwell. An abdominal CT scan was performed and revealed an aortic aneurysm with a maximum transversal diameter of 5.1 cm and a Salmonella paratyphi B mycotic aneurysm of the abdominal aorta in an HIV-infected patient 175 total cranio-caudal length of 9.5 cm starting below the renal ostia and complicated by a posterior 1cm fissuration into a false lumen, which was narrowing the true lumen. Aortic walls were strictly wrapped by multiple retroperitoneal adenopathies (Figure 1). The patient was referred for emergency vascular surgery performed 12 hours later. The aneurysmatic aorta was resected between the area below the renal arteries and the proximal part of the iliac arteries and a homograft with a cryopreserved aorta from donor was performed after a wide debridement of all infected tissue. The false lumen was filled with purulent material and wall samples were sent for both histological examination and microbiological culture analysis, which were positive for Salmonella paratyphi B. The strain was found to be sensitive to all the routine anti- Figure 1 - (A) Axial CT projection shows a large fluid collection with rim enhancement, surrounding the aorta which presents the saccular dilatation (maximum transversal diameter of 5.1 cm and a total cranio-caudal length of 9.5 cm starting below the renal ostia) complicated by a posterior fissuration into a false lumen. (B) A coronal view of the aneurysm (C), a volume-rendered 3-dimensional reconstruction and (D) a sagittal view of the mycotic aneurism showing the multiple colliquated lymph nodes surrounding the aorta and the saccular aneurysm. biotics tested for and continuous iv. piperacillin/ tazobactam antibiotic therapy was continued in combination with antihypertensive agents and narcotic analgesics. Repeat C reactive protein levels dropped from 31 mg/dL to 9 mg/dL by day 4; and the patient remained afebrile since post-operative day 1. Unfortunately, despite the improving clinical condition, the patient died on post-operative day 7 following haemorrhagic shock associated with graft rupture. nDISCUSSION Non-typhoid Salmonella species (NTS), including Salmonella paratyphi B, consist of a vast group of anaerobic, rod-shaped Gram negative bacteria, responsible for a large number of widely distributed foodborne diseases [2]. Salmonella paratyphi B infection causes paratyphoid fever, a disease characterized by acute onset of fever, abdominal pain, diarrhoea, nausea and sometimes vomit [2, 3]. However, 5% of patients also develop bacteraemia after the bacterial translocation over the gastrointestinal tract [4]. Some Salmonella serotypes show a predisposition to develop bacteraemia over others, and is much more frequent in the elderly population and in immunocompromised patients, including HIV-infected patients [1, 4]. Limited data suggest 30-day mortality rates as high as 60% in developing countries [5]. NTS can be responsible for as much as 8% of bacteraemia in HIV patients and are found in 15-35% of bacterial aortitis [1, 6-8]. NTS sepsis is more severe in HIV-positive patients with mortality related to severe sepsis in this group ranging around 30-55% [9, 10]. NTS may have predilection to attack the damaged vascular endothelium, favouring the development of a mycotic aneurysm [7]. The infra-renal segment of the abdominal aorta is the most frequent location for infected aneurysms, which can be evaluated by contrast-enhanced CT (CECT) that reveals aortic wall thickening, periaortic fluid or soft-tissue accumulation and rapidly progressing saccular aneurysms [1, 8, 11-14]. CECT also allows a multiplanar view with 3-dimensional reconstructions and excellent spatial resolutions, evaluating the aortic wall changes, luminal changes and disease extent to help find the best surgical approach [15]. Our patient was diagnosed with an advanced infectious aortitis complicated by an initial fissura- 176 N. Girometti, et al. tion of a mycotic aneurysm (see Figure 1), consistent with risk factors reported in the literature [16]. Infected aneurysms are usually irreversible and appear very frequently as complication of aortitis, holding a 40-45% mortality rate even when treated with both antibiotic therapy and surgery, although it has been demonstrated a beneficial impact on survival when prompt diagnosis and treatment are provided [1, 17, 18]. While an initial medical approach with adequate antibiotic therapy alone is reported to perform poorly with an average 96% mortality, early open surgery seems to grant the best outcome, albeit post-operatory mortality ranges from 11% to 45% depending on the extent of vascular damage, surgical technique, and time to treat [1, 8, 17, 19, 20]. Open-surgery treatment may not be suitable in patients with high operative risk and repair of thoracic aortic aneurysms by endoluminal stent-grafting is an emerging alternative to surgical intervention, including treatment of mycotic aneurysm [8, 18, 21]. For those patients with non-critical conditions, length of antimicrobial treatment before surgery is controversial and ranges from 1 week to 4 months [20]. Microbiological management of intraoperatory samples is also a very important stage of management, because pathologic confirmation of the diagnosis and susceptibility testing are essential to confirm adequate antimicrobial therapy. Despite the unfortunate ending, our case report underlines the importance to include cardiovascular infections in the differential diagnosis every time a septic patient with an uncontrolled HIV viral load and a lymphocyte CD4+ cell-count below 200/mm3. In these situations, Salmonella species infection can be a possible cause for disease and aorta must be investigated along other sites. MALDI-TOF can be a very useful resource, offering the fastest way to detect the pathogen from blood cultures and prompting appropriate follow-up radiographic examinations [22]. No financial support was received for this study All authors: No reported conflicts of interest. Keywords: HIV, Salmonella paratyphi, aortic aneurysm. SummaRY An HIV-infected 49-year-old man was admitted with polyuria, fever, chills and a dull left lumbar pain. Laboratory tests showed increased C-reactive protein while urine analysis and abdomen ultrasound scan were negative. Blood cultures revealed a Salmonella paratyphi B, identified through MALDI-TOF mass spectrometry. Targeted antibiotic therapy with intravenous piperacillin/tazobactam was started and a multi-phase contrast-enhanced abdomen CT-scan was performed at 24 hours from admission showing a saccular aneurysm of the abdominal aorta with a 1 cm penetrating aortic ulcer on posterior wall. The patient underwent emergency vascular surgery at 34 hours from admission for debridement and homo-graft placement of sub-renal aorta, and surgical samples were sent for microbiological analysis. Unfortunately, the patient died on post-surgical day 7 after haemorrhagic shock due to laceration of his graft. Salmonella paratyphi infection can be responsible for sepsis in severely immunosuppressed patients with poorly controlled HIV, requiring careful work-up for cardiovascular involvement. RIASSUNTO Di seguito descriviamo il caso di un paziente HIV-positivo di 49 anni, con uno scarso controllo della malattia di base, che si presenta con febbre, poliuria e dolore lombare. In seguito alle prime indagini diagnostiche si riscontra un quadro settico per cui si imposta terapia antibiotica empirica con piperacillina/tazobactam e.v. che viene successivamente confermata alla luce della identificazione MALDI-TOF su emocolture di Salmonella paratyphi. Per il persistere di dolore addominale il paziente veniva sottoposto a TC addome multifase che identificava la presenza di aneurisma dell’aorta addominale con iniziale ulcerazione della parete vascolare posteriore. Pertanto, a 34 ore dal ricovero, veniva sottoposto ad intervento di resezione dell’aneurisma a livello sotto-renale e trapianto aortico da donatore. Nel post-intervento si assisteva al netto miglioramento degli indici di flogosi e allo sfebbramento del paziente, che decedeva però in settima giornata post-operatoria in seguito a shock emorragico da rottura del graft. L’infezione da Salmonella paratyphi può provocare sepsi in pazienti gravemente immunocompromessi e con malattia da HIV scarsamente controllata, e richiede un controllo completo minuzioso per il coinvolgimento cardiovascolare. Salmonella paratyphi B mycotic aneurysm of the abdominal aorta in an HIV-infected patient 177 nREFERENCES [1] Fernandez Guerrero M.L., Aguado J.M., Arribas A., Lumbreras C., de Gorgolas M. The spectrum of cardiovascular infections due to Salmonella enterica: A review of clinical features and factors determining outcome. Medicine (Baltimore). 83, 123-138, 2004. [2] Shane A.L., Roels T.H., Goldoft M., Herikstad H., Angulo F.J. Foodborne disease in our global village: A multinational investigation of an outbreak of Salmonella serotype Enteritidis phage type 4 infection in Puerto Vallarta, Mexico. Int. J. Infect. Dis. 6, 98-102, 2002. [3] Bhan M.K., Bahl R., Bhatnagar S. Typhoid and paratyphoid fever. Lancet. 366, 749-762, 2005. Dhanoa A., Fatt Q.K. Non-typhoidal Salmonella bacteraemia: Epidemiology, clinical characteristics and its association with severe immunosuppression. Ann. Clin. Microb. 8, 15, 2009. [4] Gordon M.A., Banda H.T., Gondwe M. Non-typhoidal salmonella bacteraemia among HIV-infected Malawian adults: high mortality and frequent recrudescence. AIDS 16, 1633-1641, 2002. [5] Meremo A., Mshana S.E., Kidenya B.R., et al. High prevalence of non-typhoid salmonella bacteraemia among febrile HIV adult patients admitted at a tertiary Hospital, North-Western Tanzania. Int. Arch. Med. 5, 28, 2012. [6] Bnennson S., Raveh D., Schlesinger Y. The risk of vascular infection in adult patients with nontyphi Salmonella bacteremia. Am. J. Med. 110, 60-63, 2001. [7] Leon L.R.Jr., Mills J.L.Sr. Diagnosis and management of aortic mycotic aneurysms. Vasc. Endovasc. Surg. 44, 1, 5-13, 2010. [8] Mrus J.M., Braune L.A., Yi M.S., Linde-Zwirble W.T., Johnston J.A. Impact of HIV/AIDS on care and outcomes of severe sepsis. Crit. Care 9, 623-630, 2005. [9] Silva Jr. J.M., De Sousa dos Santos S. Sepsis in AIDS patients: clinical, etiological and inflammatory characteristics. J. Int. AIDS Soc. 16, 17344, 2013. [10] Hsu R.B., Lin F.Y., Chen R.J., Hsueh P.R., Wang S.S. Antimicrobial drug resistance in Salmonella-infected aortic aneurysms. Ann. Thorac. Surg. 80, 530-536, 2005. [11] Restrepo C., Ocazionez D., Suri R., Vargas D. Aorti- tis: Imaging Spectrum of the Infectious and Inflammatory Conditions of the Aorta. RadioGraphics. 31, 435-451, 2011. [12] Kam M.H., Toh L.K., Tom S.G., Wong D., Chia K.H. A case report of endovascular stenting in Salmonella mycotic aneurysm: a successful procedure in an immunocompromised patient. Ann. Acad. Med. Singapore. 36, 1028-1031, 2007. [13] Lee M.H., Chan P., Chiou H.J., Cheung W.K. Diagnostic imaging of Salmonella-related mycotic aneurysm of aorta by CT. Clin. Imaging 20, 26-30, 1996. [14] Katabathina V.S., Restrepo C.S. Infectious and noninfectious aortitis: cross-sectional imaging findings. Semin Ultras CT MRI. 33, 207-221, 2012. [15] Hsu R.B., Chang C.I., Wu I.H., Lin F.Y. Selective medical treatment of infected aneurysms of the aorta in high risk patients. J. Vasc. Surg. 49, 66-70, 2009. [16] Soravia-Dunand V.A., Loo V.G., Salit I.E. Aortitis due to Salmonella: report of 10 cases and comprehensive review of the literature. Clin. Infect. Dis. 29, 4, 862868, 1999. [17] Taylor L.M., Deitz D.M., McConnell D.B., Porter J.M. Treatment of infected abdominal aneurysms by extraanatomic bypass, aneurysm excision, and drainage. Am. J. Surg. 155, 655–658, 1988. [18] Leo´n L.R., Ihnat D.M., Mills J.L. Chapter 41-vascular complications: primary arterial infections. In Comprehensive Vascular and Endovascular Surgery (Hallett J.J., Mills J.L., Earnshaw [19] J.J., Reekers J.A, Eds.). 2008, 714-726. Elsevier, Philadelphia, PA. [20] Hsu R.B., Chen R.J., Wang S.S., Chu S.H. Infected aortic aneurysms: clinical outcome and risk factor analysis. J. Vasc. Surg. 40, 1, 30-35, 2004. [21] Kan C.D., Lee H.L., Yang Y.J. Outcome after endovascular stent graft treatment for mycotic aortic aneurysm: a systematic review. J. Vasc. Surg. 46, 5, 906-912, 2007. [22] Klein S., Zimmermann S., Köhler C., Mischnik A., Alle W., Bode K.A. Integration of matrix-assisted laser desorption/ionization time-of-flight mass spectrometry in blood culture diagnostics: a fast and effective approach. J. Med. Microbiol. 61, 323-331, 2012.