Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
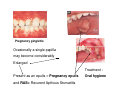
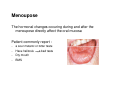
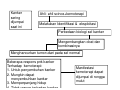
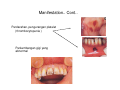
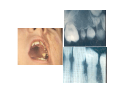
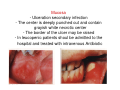
Endocrine abnormalities • In general changes in the oral mucosa dictated by endocrine abnormalities are not common • The most frequently cited changes are those due to the endocrine disturbances found in normal life especially: during preqnancy and at the menoupouse PREGNANCY The hormonal changes that occure chronic gingivitis proliferation of capillaries fragile papillae may bleed at the least injury secondary infection may occure may lead to halitosis Pregnancy gingivitis Ocasionally a single papilla may become considerably Enlarged Treatment : Present as an epulis = Pregnancy epulis and RAS= Recurent Apthous Stomatitis Oral hygiene Kehamilan Tanda dimulut Pregnancy ginggivitis - Pembesaran - Merah - Perdarahan Pregnancy epulis atau tumor - Menonjol - Hemorrhagic - Pada akhir kehamilan Evaluasi dan penanggulangan dental - Sesudah trimester pertama -------- dental prophylaxis - Selama trimester kedua -----perawatan gigi tertentu tidak dianjurkan ----- bacteremia - Selama akhir trimester kedua ------ perawatan yang tidak dapat ditunda ----- kontrol karies - Permulaan trimester ketiga ----- profilaksis ulangan - Bulan terakhir kehamilan ------ tidak dianjurkan - Radiography : hindari selama kehamilan - Dokter gigi harus konsultasi ke dokter sebelum pemberian obat - Obat-obatan yang harus dihindari : aspirin, lidocaine, penicillin, antianxiety ( diazepam ), nitrous oxide, tetracycline Menoupose The hormonal changes occuring during and after the menoupose directly affect the oral mucosa Patient commonly report : - a sour metallic or bitter taste Have halitosis a bad taste Dry mouth BMS MANIFESTASI KEMOTERAPI DI RONGGA MULUT Wilda Hafny Lubis drg MSi Kanker sering dijumpai saat ini Ahli- ahli scince+kemoterapi Melakukan Identifikasi & eksploitasi Perbedaan biologi sel kanker Mengembangkan obat dan kombinasinya Menghancurkan tumor>dari pada sel normal Beberapa respons pnk kanker Terhadap kemoterapi: 1. Untuk penyembuhan kanker 2. Mungkin dapat menyembuhkan kanker 3. Memperpanjang hidup 4. Tidak respon terhadap kanker Manifestasi kemoterapi dapat dijumpai di rongga mulut Kemoterapi • Perawatan kanker dengan menggunakan obat- obatan yang dapat menghancurkan sel kanker, menghentikan berlipat ganda Disebut obat anti kanker • Sel normal tumbuh dan mati secara terkontrol membelah • Sel kanker→ sel tidak normal >tidak terkontrol membentuk • • Kerusakan sel= efek samping, merusakkan sel normal juga Efek samping berpengaruh pada: • Pembentukan sel darah dalam sumsum tulang • Sel dalam saluran cerna (mouth, stomach, intestines) • Sistem reproduksi • Folikel rambut • Organ vital juga dapat terpengaruh eq. heart, lung, kidneys, nervous system Kemoterapi dapat mempengaruhi pada :…Cont. • Efek samping tergantung pada tipe dan dosis kemoterapi. • Recovery time tergantung pada kesehatan secara umum dan tipe kemoterapi yang diberikan Beberapa efek samping kemoterapi Anemia mengurangi kemampuan sel darah merah Sedikit sel darah merah yang membawa Oksigen Nafas pendek Lemah capek Nausea Vomiting Pain Obat KH dapat merusak syaraf Obat baru Rasa terbakar Reduce this Mati rasa Sakit mencucuk Pada kaki dan tangan Kehilangan rambut Dapat mengenai semua jenis rambut Akan tumbuh kembali setelah perawatan Manifestations in Oral Cavity : Mukositis and ulceration : mucosa gastrointestinal rentan terhadap efek toksik Infeksi oral: Leucopenia meningkatnya risiko infeksi , pengobatan setelah dilakukan kultur, mencegah infeksi sistemik atau septicaemia. Neurotosik, sakit yang dalam, terus menerus, bilateral dan seperti sakit gigi Xerostomia Perubahan pengecapan Manifestation.. Cont.. Perdarahan, pengurangan platelet ( thrombocytopenia ) Perkembangan gigi yang abnormal Tindakan pre kemoterapi: Pemeriksaan jaringan lunak, keras dan jaringan periodontal Pasien dengan kelainan haematologi ,mungkin menderita immunosuppression atau thrombocytopenia harus di konsul ke onkologi Hilangkan daerah infeksi dan iritasi seperti akar gigi , gigi tajam dll. Jadwal kemoterapi selanjutnya sebaiknya 7-10 hari setelah penyembuhan Informasi penting : Faktor pembekuan darah Kateter vena central Tempat kolonisasi bakteri Komplikasi haemaragik terjadi Platelet < 50 ribu/mm Perlu antibiotic prophylactic Neutrophil < High risk of infection and septicaemia Perawatan Dental / Oral yang harus diperhatikan • • • • • • • • Teknik menyikat gigi Makanan yang tajam Berkumur dengan alkohol Penggunaan propilaksis Pencegahan demineralisasi Pasien sering muntah Tidak boleh pakai gigi palsu Pertahankan oral hygiene • Sebelum memulai kemoterapi kanker , pada penderita dilakukan evaluasi untuk mengenali dan menyingkirkan sumbersumber infeksi oral yang dapat memperburuk rangkaian perawatan kemoterapi EFFECT OF RADIOTHERAPY Oral complications of head and neck radiation 1. Mucositis - Generalized mucosal erythema ( after initiation of treatment) -Desquamation and ulceration - Extreamly pain, eating nearly impossible - Sites : buccal, labial and lingual mucosae - Healing rapidly follows the cessation of radiation - Mucosal atrophy permanent - Candidiasis 2.Xerostomia - Bacterial colonization of the teeth - Difficulty of swallowing and managing food - Plaque formation and debris accumulation 3. Caries radiation - Rampant caries Caused by : xerostomia, accelerated decalcification of irrradiated teeth, reduced oral hygiene The three major risk factors in the development of osteoradionecrosis * Anatomic site of the trauma -----mandible develop necrosis 5 times more frequently * Dose of radiation * Dental status of patient ----- patients with teeth are more likely than edentulous patients Osteoradionecrosis and extraction Risk of development of osteoradionecrosis to timing of extraction : - High risk : extractions during radiation therapy - Elevated risk : extractions just prior to radiation therapy - Lowest risk : !2 mo or more after radiation therapy Extraction strategy Pre radiation extraction of actively infected teeth Extraction done 12 mo or more after radiation therapy are lesser risk Oral complications of cancer cemotheraphy Factors affecting frequency of development of oral problems 1. Patient related variables - The younger patient ------ more likely affect - The type of malignancy----- lymphoma, leukemia : higest frequency - Patient with poor oral hygiene and pre existing odontogenic and periodontal infection -------high risk Dentist should be work with oncologist to optimize the 2. Therapy related variables * Type of drug - Antimetabolite ( methotrexate ) ------ mucositis - Alkylating agent ( 5 fluorouracil------ mucositis - Adriamycin ----- minor salivary gland * Dose of drug administration * The timing of drug administration Oral Complications Direct Stomatotoxicity 1. Mucositis - Diffuse ulcerative condition - Generally on nonkeratinized oral mucosa - Extrem pain - Erythema and ulceration of some or all mucosal surfaces : typically ginggiva, dorsal surface of the tongue - Ulcerative area may appears grayish white with central areas of necrosis - Self limiting and tends to heal spontaneously in about 14 days 2. Xerostomia Adriamycin ---- xerostomia 3. Neurotoxicity Alkaloid ----- neurotoxicity ----- odontogenic pain Symptoms usually disappear with discontinueance drugs Indirect Stomatotoxicity Infection 1. Bacterial infection - Tooth pain, deep caries, sensitivity to percussion 2. Soft tissue infection * Ginggiva - Marginal, papillary and attached ginggiva in patients pre existing periodontal diseases - Infectious lesions : localized necrotic area of ginggiva ( similar to ANUG) - Tends to spread laterally, apically, large area of ginggiva and mucosa - Pain, bad taste - Underlying bone may be exposed - Bleeding Mucosa - Ulceration secondary infection - The center is deeply punched out and contain grayish white necrotic center - The border of the ulcer may be raised - In leucopenic patients shoul be admitted to the hospital and treated with intravenous Antibiotic Salivary gland infection - Parotid gland --- most frequently affected - Complain of pain of sudden onset - Unilateral - The parotid gland may be enlarged and erythemtous - Pus may be milked from the parotid duct - Fever - Dry mouth Myelosuppressed patients with salivary gland infection require hospitalization Management : cooperation of the dentist, oncologist and infectious disease specialist 2. Fungal infection In the myelosuppressed host Oral Candidiasis - Raised, white, curdy looking areas - White necrotic areas may be scraped off, revealing a raw, bleeding base - Oral candida infectious may spread to the oesophagus or lungs ------ dysphagia, febrile 3. Viral infection - Herpes simplex virus infections---- commissura of the lips - Herpes zoster infection - Recurrent herpes infection Oral bleeding cause by thrombocytopenia