Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Cardiac contractility modulation wikipedia , lookup
Electrocardiography wikipedia , lookup
Heart failure wikipedia , lookup
Myocardial infarction wikipedia , lookup
Mitral insufficiency wikipedia , lookup
Jatene procedure wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Aortic stenosis wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
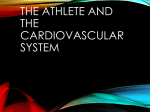
European Heart Journal – Cardiovascular Imaging (2013) 14, 1010–1020 doi:10.1093/ehjci/jes298 Comprehensive assessment of biventricular function and aortic stiffness in athletes with different forms of training by three-dimensional echocardiography and strain imaging† Antonio Vitarelli*, Lidia Capotosto, Giuseppe Placanica, Fiorella Caranci, Mario Pergolini, Francesco Zardo, Francesco Martino, Stefania De Chiara, and Massimo Vitarelli Sapienza University, Cardiac Dept., Via Lima 35, 00198 Rome, Italy Received 21 September 2012; accepted after revision 26 November 2012; online publish-ahead-of-print 8 January 2013 Previous studies have shown distinct models of cardiac adaptations to the training in master athletes and different effects of endurance and strength-training on cardiovascular function. We attempted to assess left-ventricular (LV) function, aortic (Ao) function, and right-ventricular (RV) function in athletes with different forms of training by using three-dimensional (3D) echocardiography, tissue Doppler imaging (TDI) and speckle-tracking imaging (STI). ..................................................................................................................................................................................... Methods We examined 35 male marathon runners (endurance-trained athletes, ETA), 35 powerlifting athletes (strengthand results trained athletes, STA), 35 martial arts athletes (mixed-trained athletes, MTA), and 35 sedentary untrained healthy men (controls, CTR). Two-dimensional and three-dimensional echocardiography were performed for the assessment of LV and RV systolic/diastolic function. LV and RV longitudinal strain (LS) and LV torsion (LVtor) were determined using STI (EchoPAC BT11, GE-Ultrasound). Maximum velocity of systolic wall expansion peaks (AoSvel) was determined using TDI. ETA experienced LV eccentric hypertrophy with increased 3D LV end-diastolic volume and mass and significant increase in peak systolic apical rotation and LVtor. In all groups of athletes, RV-LS was reduced at rest and improved after exercise. AoSvel was significantly increased in ETA and MTA and significantly decreased in STA compared with CTR. There were good correlations between LV remodelling and aortic stiffness values. Multivariate analysis showed aortic wall velocities to be independently related to LV mass index. ..................................................................................................................................................................................... Conclusion In strength-trained, endurance-trained, and mixed-trained athletes, ventricular and vascular response assessed by 3DE, TDI, and STI underlies different adaptations of LV, RV, and aortic indexes. ----------------------------------------------------------------------------------------------------------------------------------------------------------Keywords Echocardiography † Athlete’s heart † Tissue Doppler imaging † Speckle tracking imaging † Three-dimensional echocardiography † Ventricular function † Aortic function Introduction The haemodynamic load caused by long-term training involves both cardiac ventricular chambers, inducing an increase in ventricular diameters, wall thickness, and mass. These changes are usually described as ‘athlete’s heart’.1 – 3 Adaptations to exercise are dependent on the specific type of training performed. Previous † studies4 – 6 have shown distinct models of cardiac adaptations to the training in master athletes and different effects of endurance and strength-training on cardiovascular function. Further reports7 – 9 pointed out that the classification of left-ventricular hypertrophy in athletes as eccentric or concentric is not an absolute or dichotomous concept but has to be considered a relative Presented in part at Euroecho Meeting, Budapest, Hungary, 7–10 December 2011. *Corresponding author. Tel: +39 6 85301427; Fax: +39 6 8841926, Email: [email protected] Published on behalf of the European Society of Cardiology. All rights reserved. & The Author 2013. For permissions please email: [email protected] Downloaded from by guest on October 20, 2016 Aims 1011 Assessment of biventricular function and aortic stiffness in athletes Methods Population We examined 35 male marathon runners (endurance-trained athletes, ETA), 35 powerlifting athletes (strength-trained athletes, STA), and 35 martial arts athletes performing combined strength and endurance training (mixed-trained athletes, MTA). All of them were athletes participating in an organized team or individual sport in which regular competition was a component. Each athlete trained for .15 h/week and had participated in competition for .6 years. Thirty-five sedentary untrained healthy age-matched male adults were selected as a control group. Both groups were free of heart and systemic diseases and took no medications. Subjects with echocardiographic recordings of inadequate quality were excluded. Ethical approval was obtained. Echocardiography All patients underwent transthoracic echocardiography with a commercially available cardiovascular ultrasound system (Vivid E9, GE, Horten, Norway). Measurements of cardiac chambers and aortic diameters were made according to established criteria.23 Left-ventricular ejection fraction by modified biplane Simpson method and mass index were estimated.23 – 25 Peak early (E) and late (A) diastolic velocities, deceleration time, left-ventricular isovolumic relaxation time, and myocardial performance index were obtained using standard Doppler practices.26,27 Right-ventricular systolic pressure (RVSP) was determined by continuous wave Doppler echocardiography. Twodimensional measurements of aortic diameters were made at enddiastole in parasternal long-axis views at four levels: aortic annulus, sinuses of Valsalva, sinotubular junction, and proximal ascending aorta. Mitral and tricuspid annulus velocities (Sa, Ea, Aa) were measured by tissue Doppler imaging on the transthoracic four-chamber views. Three-dimensional echocardiography Transthoracic examination was carried out with the patient lying in the left lateral recumbent position. The echocardiographic system was equipped with dedicated software for dynamic three-dimensional acquisition. Standard parasternal, apical, and subcostal views were used. Three-dimensional images were saved in digital form on the hard disk of the ultrasound scanner and subsequently analysed using the EchoPAC view (BT11, GE Ultrasound). The left- and right- ventricular end-diastolic volumes (LVEDV, RVEDV) and ventricular endsystolic volumes (LVESV, RVESV) were measured from each threedimensional echocardiographic data set. Left- and right-ventricular ejection fractions (LVEF and RVEF) were determined. The process of volume determination was done two times for each patient. Papillary muscles were not included in the volume estimation. Speckle-tracking imaging The general principles that underlie the STI modalities have been previously described.17 After tracing endocardial border at an endsystolic frame, the operator could validate the tracking quality and adjust the endocardial border or modify the width of the region of interest. Aortic valve opening and closure were selected on pulsedwave Doppler tracings recorded from the LV outflow tract. Frame rate ranged from 60 to 100 frame/s, and three cardiac cycles were stored in cineloop format for offline analysis. Longitudinal LV strain was defined as the average of negative longitudinal strains of six segments of the septal and lateral walls in the apical four-chamber view (Figure 1A). Average radial and circumferential strain of six mid-LV segments was determined in the mid-short-axis view. The assessment of LV rotation by 2D speckle-tracking strain imaging required the acquisition of the LV short-axis at the basal and apical level. The basal level was defined as that which showed the mitral valve tip and the apical level as that which was just proximal to the level with LV cavity obliteration at end-systole. The time rotation curves were displayed along the cardiac cycle. Counterclockwise rotation was conventionally marked as positive value and clockwise rotation as negative value when viewed from the LV apex. Peak apical and basal rotation and peak LV torsion were obtained. Left-ventricular torsion or twist (LVtor) was defined as the net difference (in degrees) of apical and basal rotation at isochronal time points. Normalized torsion was torsion divided by LV ventricular diastolic longitudinal length between apex and mitral plane. Peak diastolic untwisting velocity and time-to-peak untwisting velocity were measured. Twisting rate (TR) was defined28 as (peak LVtor – LVtorEarlySystole)/(time difference between these two events). Untwisting rate (UTR) was defined as (peak LVtor – LVtorMVO)/(time difference between these two events), where MVO is mitral valve opening. The analysis of strain and rotation parameters was performed offline using customized computer software (EchoPAC BT11, GE Ultrasound). To assess regional and global RV systolic function in the longitudinal direction, we adopted a six-segment RV model (basal RV lateral wall, mid-RV lateral wall, apical RV wall, apical septum, mid septum, and basal septum). Peak systolic strain was recorded for the six RV myocardial segments and the entire RV myocardium. Global strain and strain rate were calculated by averaging local strains along the entire right ventricle using machine software. Aortic function To assess aortic distensibility, echocardiographic tracings were obtained using a two-dimensional guided M-mode evaluation of systolic and diastolic aortic diameter, 3 cm above the aortic valve. Downloaded from by guest on October 20, 2016 concept, and a combined training of endurance and power can produce an extreme volume and pressure load. Moreover, in competitive athletes, left-ventricular hypertrophy can mimic pathological conditions (systemic arterial hypertension or hypertrophic cardiomyopathy) and this distinction may have important implications, particularly in adults who practice regular physical activity.10 Although standard Doppler echocardiography has been widely used to distinguish athlete’s heart by pathological LV hypertrophy,11,12 there are scanty data in the literature on the relationship between ventricular function and arterial function in athletes. Even the new echocardiographic techniques13 – 22 applied to the study of wall motion and ventricular volumes such as tissue Doppler imaging (TDI), speckletracking imaging (STI), and three-dimensional echocardiography (3DE), which were used to analyse LV function in different types of physiological and pathological hypertrophy, have produced limited data on left- and right-ventricular volumes and aortic stiffness. Accordingly, we attempted to assess systemic ventricular –vascular function and right-ventricular function in athletes with different forms of training by using TDI, STI, and 3DE in order to assess (1) biventricular volumetry and function at rest and after stress; (2) aortic stiffness and its relationship with left-ventricular remodelling, and (3) advantages of these new technologies compared with standard ones. 1012 A. Vitarelli et al. Downloaded from by guest on October 20, 2016 Figure 1 Application of echocardiographic techniques in an athlete. (A). Speckle-tracking imaging (STI) and LV longitudinal strain. (B). Ascending aortic wall TDI velocity profile: aortic wall peak systolic radial strain is derived from velocity data. AAo ¼ wall late diastolic velocity; EAo ¼ wall early diastolic velocity; SAo ¼ wall systolic velocity. The elastic properties of the aorta were indexed by calculation29 – 31 of aortic distensibility (D), stiffness index (SI), and pressure– strain elastic modulus (Ep) as D ¼ 2(As – Ad)/[Ad (Ps 2 Pd)], SI ¼ ln(Ps / Pd) / (As – Ad)/Ad, and Ep ¼ (Ps – Pd)/[(As 2 Ad)/ Ad], respectively, where As, aortic diameter at end-systole; Ad, aortic diameter at end-diastole; Ps, systolic blood pressure; Pd, diastolic blood pressure; and ln, natural logarithm. Aortic wall TDI velocities have been obtained as previously described.32 By marking a region of interest on the 2D image in the anterior aspect of the ascending aorta at the same point as in M-mode measurements, velocities throughout the cardiac cycle for this area can be determined (Figure 1B). Offline analysis of the velocity data sets was performed using dedicated software (EchoPAC BT11, GE Ultrasound). Tissue Doppler imaging tracing displayed accelerated 1013 Assessment of biventricular function and aortic stiffness in athletes Statistics 3D volumetry in athletes and controls Data are presented as mean value + SD. Linear correlations, univariate and multivariate analysis were used for comparisons. Variables were compared between groups by Student’s t-test. Differences were considered statistically significant when the P-value was , 0.05. To analyse intraobserver variability, measurements of 2D strain parameters were made at multiple sites in different patients on two different occasions. For interobserver variability, a second investigator randomly made measurements at the above different sites without knowledge of other echocardiographic parameters. The intraobserver and interobserver variabilities were determined as the difference between the two sets of observations divided by the mean of the observations and expressed as a percentage. ETA and MTA experienced LV eccentric hypertrophy, characterized by increased LV end-diastolic volume and mass (Figure 2). Three-dimensional LVEDV, LVESV, RVEDV, and RVESV were enlarged in athletes compared with controls (Table 3). A close association between 3D LV and RV end-diastolic volume in the three groups of athletes was found (r ¼ 0.72, P , 0.001). On multiple linear regression analysis, the body surface area, type and duration of training, and LV end-diastolic volume were the only independent determinants of RV end-diastolic volume (F ¼ 73.2, P , 0.005). Exercise stress-echo TDI –STI parameters in athletes and controls Results Intraobserver variability was 4.6 + 2.8% for 3D-LVEDV, 5.3 + 4.9% for 3D-LVESV, 4.8 + 3.6% for 3D-RVEDV, 5.7 + 5.8% for Table 1 LV diastolic function measurements such as mitral Ea and tricuspid Ea were increased in athletes compared with the control group (Table 3). Age, anthropometric, and clinical characteristics of the study population Controls (n 5 35) ETA (n 5 35) STA (n 5 35) MTA (n 5 35) P-value ............................................................................................................................................................................... Age Body surface area (cm2) 28.3 + 11.4 1.89 + 0.23 28.7 + 10.7 1.91 + 0.15 30.3 + 9.4 1.98 + 0.18 29.4 + 9.8 1.93 + 0.13 NS NS Body mass index (kg/m2) 22.4 + 2.4 22.7 + 2.6 23.4 + 3.1 22.9 + 2.5 0.05* Training experience (years) HR (bpm) / 69.5 + 9.1 9.6 + 2.9 54.1 + 5.6 9.1 + 3.2 65.8 + 8.6 9.7 + 3.1 60.1 + 7.4 NS ,0.005† SBP (mmHg) 120.6 + 7.2 121.9 + 6.8 129.1 + 7.4 123.2 + 7.1 0.03‡ DBP (mmHg) Double product (SBP x HR) 75.2 + 5.7 7335 + 1253 71.3 + 5.4 6731 + 1249 76.3 + 4.8 8247 + 1459 70.9 + 4.6 7121 + 1231 NS 0.01‡ RVSP 21.6 + 6.2 28.4 + 7.3 23.4 + 6.5 27.6 + 7.6 0.05§ DBP, diastolic blood pressure; ETA, endurance-trained athletes; HR, heart rate; MTA, mixed-trained athletes; NS, not significant; RVSP, right-ventricular systolic pressure; SBP, systolic blood pressure; STA, strength-trained athletes. *STA vs. controls. † ETA vs. controls. ‡ STA vs. ETA, MTA, and controls. § ETA and MTA vs. controls. Downloaded from by guest on October 20, 2016 Exercise stress-echo test was undertaken by bicycle ergometry in the supine position, with initial workload set at 25 W and 25 W increments every 2 min. Heart rate and rhythm were continuously recorded by 12-lead ECG, and blood pressure was measured manually during the last 30 s of each stage by sphygmomanometry. The following functional and echocardiographic indexes were assessed at peak effort: maximal HR, maximal systolic blood pressure (SBP), maximal workload (number of Watts achieved by bicycle test), rate– pressure product (maximal HR x maximal SBP), LVEF, annular early diastolic velocity (Ea), left-ventricular longitudinal strain (LV LS), left-ventricular torsion (LVtor), aortic wall systolic velocity (AoSvel), RVEF, rightventricular longitudinal strain (RV LS). 3D-RVESV, 7.9 + 3.3% for STI longitudinal strain, 9.7 + 5.4% for STI strain rate, and 4.7 + 3.2% for AoSvel. Interobserver variability was 5.1 + 3.3% for 3D-LVEDV, 6.2 + 5.6% for 3D-LVESV, 5.4 + 3.1% for 3D-RVEDV, 8.2 + 5.6% for 3D-RVESV, 9.6 + 4.1% for STI longitudinal strain, 15.8 + 6.4% for STI strain rate, and 5.9 + 4.2% for AoSvel. With regard to the data obtained with exercise, intraobserver variability was 8.1 + 3.8% for 3D-LVEDV, 10.9 + 5.8% for 3D-LVESV, 8.6 + 4.4% for 3D-RVEDV, 11.3 + 6.1% for 3D-RVESV, 11.7 + 3.6% for STI longitudinal strain, 16.3 + 4.6% for STI strain rate, and 6.2 + 4.2% for AoSvel. Interobserver variability was 9.3 + 5.2% for 3D-LVEDV, 13.8 + 6.5% for 3D-LVESV, 9.9 + 4.5% for 3D-RVEDV, 14.9 + 7.8% for 3D-RVESV, 13.3 + 4.9% for STI longitudinal strain, 18.8 + 6.7% for STI strain rate, and 7.7 + 5.8% for AoSvel. The overall feasibility of speckle-tracking echocardiography at rest and peak stress was 94% and overall feasibility of 3D echocardiography was 87%. The baseline age, anthropometric, and clinical characteristics are given in Table 1. Mmode/2D findings are given in Table 2. expansion of the aortic wall followed by a slow deceleration, a plateau, and then a rapid deceleration into diastole. This trace represents the mean of the instantaneous velocity spectrum. Systolic maximum wall expansion velocity (AoSvel, cm/s), wall contraction early diastolic velocity (AoEvel, cm/s), and wall peak systolic radial strain (AoS, %) were derived. 1014 A. Vitarelli et al. Table 2 M-mode/2D findings in athletes and controls Controls (n 5 35) mean + SD ETA (n 5 35) mean + SD STA (n 5 35) mean + SD MTA (n 5 35) mean + SD P-value LVED (mm) LVES (mm) 48.2 + 4.3 29.3 + 2.6 55.7 + 4.9* 31.2 + 3.4 49.1 + 4.3 28.5 + 2.8 51.3 + 3.8† 29.7 + 3.1 0.01*, 0.05† NS IVST (mm) 9.5 + 1.6 10.5 + 1.7 12.4 + 1.4 10.6 + 1.5 0.01‡ PWT (mm) RWT 8.7 + 1.8 0.42 + 0.07 10.3 + 1.5 0.40 + 0.09 12.3 + 1.2 0.46 + 0.06 10.4 + 1.7 0.41 + 0.08 0.05‡ 0.01‡ LVM (g) 129 + 23 189 + 25 159 + 26 182 + 29 ,0.05§ 115 + 18 179 + 22 143 + 20 164 + 24 ,0.05*,† 65 + 5 64 + 7 65 + 5 67 + 4 Parameters ............................................................................................................................................................................... LV M-mode 2D LVEDV (mL) LVEF NS Aorta M-mode 29.1 + 3.5 29.7 + 3.3 30.8 + 3.4 29.5 + 3.1 NS 25.6 + 3.2 3.44 + 1.12 26.3 + 3.7 3.83 + 0.82 27.5 + 3.6 6.14 + 1.85 26.4 + 3.2 4.09 + 0.82 NS 0.02‡ AoEM (kPa) 31.1 + 2.1 30.3 + 2.3 45.5 + 5.1 30.7 + 2.4 0.03‡ 72.6 + 15.2 81.4 + 14.2 48.1 + 14.2 79.7 + 14.4 0.05‡ Ao-An (mm) 23.4 + 3.1 23.6 + 3.2 24.9 + 3.3 23.8 + 3.1 0.05|| Ao-SV (mm) Ao-ST (mm) 33.1 + 3.5 28.2 + 3.6 32.7 + 3.4 29.2 + 3.4 37.6 + 3.8 32.3 + 3.3 34.1 + 3.3 28.6 + 3.5 0.05|| 0.05|| AAo (mm) 32.4 + 3.1 32.9 + 3.2 34.5 + 3.1 32.6 + 3.3 0.05|| 22.6 + 2.3 26.9 + 2.6 23.3 + 2.4 25.3 + 2.1 0.05*, 0.03† 15 + 5 24+4 16 + 5 21 + 5 0.05*, 0.03† 2 AoD (m /Newton) 2D RV M-mode RVED (mm) 2D RVEDA (mm2) 2 RVESA (mm ) RVFAC (%) 8+3 10 + 2 9+4 9+3 NS 42 + 8 41 + 6 38 + 5 40 + 7 NS AAo, ascending aorta; Ao-An, aortic annulus; AoD, aortic distensibility; AoED, aortic end-diastolic diameter; AoEM, aortic elastic modulus; AoES, aortic end-systolic diameter; AoSI, aortic stiffness index; Ao-ST, aortic sinotubular junction; Ao-SV, aortic sinuses of Valsalva; LVED, left-ventricular end-diastolic diameter; LVES, left-ventricular end-systolic diameter; LVM, left-ventricular mass; IVST, interventricular septal thickness; NS, not significant; PWT, posterior wall thickness; RVED, right-ventricular end-diastolic diameter; RVEDA, right-ventricular end-diastolic area; RVESA, right-ventricular end-systolic area; RVFAC, right-ventricular fractional area change; RWT, right wall thickness; LVEDV, left-ventricular end-diastolic volume; LVEF, left-ventricular ejection fraction. *ETA vs. controls. † MTA vs. controls. ‡ STA vs. controls. § ETA, STA, MTA vs. controls. || STA vs. ETA, MTA, and controls. LV longitudinal strain increased from base to apex in all groups of athletes. There was a significant increase in peak systolic apical rotation and peak LVtor in ETA and MTA (Figure 2, Table 3). Global RV STI longitudinal strain was significantly lower than control group in all athletes and was especially reduced in basal segments (Table 3). Right-ventricular systolic pressure (RVSP) was obtained by tricuspid regurgitation in 79/105 athletes (Table 1). In these athletes, there was a close relation between RVSP and RV LS (r ¼ 20.76, P , 0.001). TDI-derived indexes of Ao function and correlation with LV function Aortic diameters at all levels were significantly larger in STA than in ETA, MTA, and controls (Table 2). Aortic wall velocities and strain were significantly decreased in STA (P , 0.001) and significantly increased in MTA (P , 0.05) and ETA (P ¼ 0.003) compared with controls (Figure 2, Table 3). By univariate analysis there was a good correlation between LV remodelling and aortic function Downloaded from by guest on October 20, 2016 AoES (mm) AoED (mm) AoSI 1015 Assessment of biventricular function and aortic stiffness in athletes parameters (Figure 3). Multivariate analysis showed aortic wall velocities and strain to be independently related to the body surface area, type and duration of training, and LV mass index (F ¼ 74.1, P , 0.001). Bicycle ergometric test During maximal physical effort (Table 4), ETA and MTA showed a better functional capacity compared with STA, with greater maximal workload achieved with lower maximal heart rate and systolic blood pressure. The baseline increase in peak systolic apical rotation translated into a highly significant increase in peak systolic LV torsion after exercise. Right-ventricular strain was reduced at rest (Table 3) and improved after exercise (Table 4). Decreased AoSvel values persisted in STA during maximal physical effort (Table 4). Discussion To our knowledge, a study assessing comprehensively biventricular function and aortic distensibility in athletes with different forms of training with the use of 3DE and strain imaging has not been reported. Novel findings of this study in athletes were the assessment of 3D RV –LV volumes, the assessment of behaviour of RV –LV deformation and torsion parameters and assessment of TDI aortic wall properties. In athletes subjected to purer endurance-type training, we found eccentric hypertrophy characterized by increased LV end-diastolic volume and mass as well as LV torsion. Aortic wall velocities and strain were significantly increased in endurance athletes and significantly reduced in power- trained athletes compared with controls. The martial arts athletes performing combined strength and endurance training presented a significant increase in left-ventricular end-diastolic volume and torsion and aortic wall velocities and strain but with lower significance values when compared with endurance athletes. All athletes had increased LV longitudinal strain and decreased RV longitudinal strain. A good correlation was shown between left- and rightventricular volumes and between LV function and aortic parameters. LV and RV volumes Marathon athletes, involved in a high dynamic component of aerobic training, developed an increase in the size of left- and right-ventricular chambers, with a proportional increase in LV thickness and volume caused by volume overload, thus showing eccentric LV hypertrophy. On the other hand, power athletes, involved in exercises with predominantly anaerobic component, showed an increase in LV wall thickness and relative wall thickness, with a geometric pattern of concentric hypertrophy due to the high systolic systemic blood pressure caused by this type of exercise. Recent studies7 – 9 considered that the classification of leftventricular hypertrophy in athletes as eccentric or concentric is not an absolute or dichotomous concept but rather a relative concept. It should also be noted that genetic factors as well as the somatotype could play a significant role for the cardiac dimensions in addition to the body dimensions.33 In our study, athletes of martial arts with mixed training developed an intermediate pattern of adaptation with increased cardiac volumes albeit to a lesser extent than marathon runners. The use of 3DE helped to Downloaded from by guest on October 20, 2016 Figure 2 Three-dimensional left-ventricular end-diastolic volume index (3D-LVEDVI) (A), LV mass index (LVMI) (B), LV torsion (LVtor) (C), and aortic wall velocity (AoSvel, D) in controls (CTR), endurance-trained athletes (ETA), strength-trained athletes (STA), and martial arts athletes (MTA). *P , 0.005, †P ¼ 0.01, ‡P ¼ 0.02, §P ¼ 0.05, ||P ¼ 0.01, #P ¼ 0.02, **P , 0.005 (all P-values vs. CTR). 1016 A. Vitarelli et al. Table 3 3D, TDI, and STI values in athletes and controls Controls (n 5 35) mean + SD Parameters ETA (n 5 35) mean + SD STA (n 5 35) mean + SD MTA (n 5 35) mean + SD 193 + 26 103 + 11 154 + 23 82 + 13 179 + 27 95 + 10 P-value ............................................................................................................................................................................... LV 3D 3D-LVEDV (mL) 3D-LVEDVI (mL/m2) 126 + 21 64 + 14 ,0.005*, 0.03† ,0.005*, 0.01† 63 + 7 64 + 6 64 + 5 65 + 7 124 + 25 69 + 17 178 + 30 107 + 15 149 + 22 93 + 11 167 + 28 104 + 12 0.03*, 0.05† 0.02*, 0.05† 12.2 + 2.3 5.5 + 1.4 20.3 + 4.2 2.7 + 0.9 14.7 + 2.6 2.4 + 0.7 18.8 + 4.4 2.3 + 0.8 0.01*, 0.04† 0.04*, 0.03† Global LS (%) Global RS (%) 220.3 + 2.6 48.9 + 9.7 221.7 + 2.6 46.9 + 9.4 222.5 + 2.4 49.6 + 8.5 221.6 + 2.2 47.5 + 8.7 ,0.05‡ NS Global CS (%) 224.7 + 3.4 222.9 + 3.3 224.1 + 2.7 222.6 + 3.6 NS 14.6 + 4.3 10.1 + 3.6 21.5 + 5.2 14.2 + 4.3 15.8 + 4.5 10.8 + 3.7 20.8 + 5.4 13.8 + 3.9 26.7 + 2.3 27.7 + 2.2 26.8 + 1.9 27.6 + 2.4 1.8 + 0.4 2.5 + 0.5 1.9 + 0.8 2.4 + 0.6 3D-LVEF LVM (g) LVMI (g/m2) NS TDI MV Ea (cm/s) MV E/Ea STI 0.01* 0.05* NS 0.03* 78.9 + 15 93.9 + 21 83.1 + 16 92.2 + 22 NS 16.5 + 7.1 20.3 + 8.3 17.5 + 5.3 19.4 + 6.7 NS 61.7 + 24 94.2 + 29 64.2 + 23 80.6 + 31 0.03* AoSvel (cm/s) AoEvel (cm/s) 6.2 + 0.4 7.2 + 0.8 7.2 + 0.6 7.5 + 0.8 4.7 + 0.3 4.3 + 0.6 6.8 + 0.5 7.7 + 0.4 0.04*, ,0.005† 0.04† AoS (%) 8.5 + 1.4 9.9 + 1.6 5.5 + 1.3 9.6 + 1.3 0.02*, ,0.005† 77 + 19 115 + 12 96 + 12 112 + 17 0.01*, 0.03† 40 + 8 56 + 7 63 + 10 55 + 4 54 + 10 52 + 7 59 + 12 54 + 6 0.01*, 0.02† NS 11.6 + 2.4 4.6 + 1.1 19.6 + 4.7 3.4 + 0.7 15.5 + 3.2 2.4 + 0.6 18.9 + 4.3 2.9 + 1.1 0.02*, ,0.05† 0.04*, 0.01† RV Global LS (%) RV FW Basal LS (%) 228.2 + 3.8 225.7 + 2.9 226.7 + 2.9 221.2 + 2.3 227.4 + 3.4 222.3 + 2.2 226.3 + 3.2 221.5 + 2.4 0.03*, ,0.05† 0.01*, 0.04† RV FW Apical LS (%) 229.8 + 4.2 229.3 + 4.8 229.8 + 4.3 228.9 + 4.6 NS Normalized time to peak UTV (%) UTR (degrees/s) Aorta RV 3D 3D-RVEDV (mL) 2 3D-RVEDVI (mL/m ) 3D-RVEF TDI TV Ea (cm/s) TV E/Ea STI AoEvel, aortic wall early diastolic velocity; AoS, aortic wall peak radial strain; AoSvel, aortic wall systolic velocity; CS, circumferential strain; E, mitral inflow early diastolic velocity; Ea, annular early diastolic velocity; EF, ejection fraction; FW, free wall; LS, longitudinal strain; LV, left ventricle; LVM, left-ventricular mass; LVMI, left-ventricular mass index; LVtor, left-ventricular torsion; MV, mitral valve; NS, not significant; RS, radial strain; RV, right ventricle; time to peak UTV, time to peak untwisting velocity (expressed as percentage of duration of diastole); UTR, untwisting rate; UTV, untwisting diastolic velocity; TV, tricuspid valve; 3D-LVEDV, three-dimensional left-ventricular end-diastolic volume; 3D-LVEDVI, three-dimensional left-ventricular end-diastolic volume index; 3D-LVEF, three-dimensional left-ventricular ejection fraction; 3D-RVEDV, three-dimensional right-ventricular end-diastolic volume; RVEDVI, three-dimensional right-ventricular end-diastolic volume index; 3D-RVEF, three-dimensional right-ventricular ejection fraction. *ETA and MTA vs. controls. † STA vs. controls. ‡ ETA, MTA, and STA vs. controls. Downloaded from by guest on October 20, 2016 Peak LVtor (degrees) Peak apical rotation (degrees) Peak basal rotation (degrees) Normalized peak LVtor (degrees/cm) Peak UTV (degrees/s) 1017 Assessment of biventricular function and aortic stiffness in athletes the ventricular septum, also causes deformation of RV walls as well as RV pressure and relaxation rate changes. LV and RV wall velocities and strain assess left- and right-ventricular volumes and better characterize different cardiovascular adaptations. This is in keeping with previous reports21 that showed that 3DE offers more detailed information on LV remodelling compared with 2DE since it takes into account differences in the length and shape of the LV chamber and provides data on LV geometry, function, and synchronicity of contraction, differently from patients with hypertrophic or dilated cardiomyopathy that do not show LV harmonic remodelling. Our results have also highlighted a close association between LV and RV end-diastolic volumes in the three groups of athletes. Multivariate analysis has provided additional information about this association with adjustment for several confounding factors. These independent associations point to a mutual dependency between the two ventricles in the trained heart. Overload alterations may be highly obvious in athletes that represent a model of extreme physiological haemodynamic load with a large increase in training-induced LV stroke volume. Ventricular interaction is the expression of the close anatomical association between the two ventricles, which are surrounded by common muscle fibres, share a septal wall, and are enclosed within the pericardium. Leftventricular volumetric expansion, changing the location and size of Downloaded from by guest on October 20, 2016 Figure 3 (A) Relation in all the athletes between threedimensional left-ventricular end-diastolic volume index (3D-LVEDVI) and aortic wall velocity (AoSvel) determined by TDI. (B) Relation in all the athletes between LV mass index (LVMI) and AoSvel. Tissue Doppler findings showed higher early diastolic myocardial velocity and Ea/Aa ratio in LV and RV lateral walls in ETA and MTA compared with controls confirming previous reports.14 – 16 These observed differences in biventricular diastolic behaviour suggest a supernormal diastolic function of athlete’s heart. Since peak velocity and Ea/Aa ratio are the expression of abnormal atrioventricular pressure gradient and passive diastolic properties of ventricular walls, their increase in ETA and MTA suggests a training-induced improvement of left- and right-ventricular compliance. LV longitudinal strain increased significantly from base to apex in all groups of athletes. Previous studies have used STI to characterize both athlete’s heart and pathological hypertrophy.17,18 Both global LS (cutoff point , 219%) and E/Ea ratio (cutoff point ≤ 6.16) appeared to be accurate to discriminate between controls and hypertensive patients, with E/Ea ratio being more sensitive and GLS more specific.34 It is known that the ‘physiological’ hypertrophy in athletes shows increased ventricular mass and normal organization of cardiac structure with no increase in collagen content, whereas hypertrophic cardiomyopathy is associated with structural myofibrillar changes, collagen accumulation, and potential systolic and diastolic dysfunction. In our athletes, longitudinal strain was higher compared with controls, whereas radial and circumferential strains were not significantly different. This is consistent with previous studies that compared various types of LV systolic deformation and found that the behaviour of longitudinal systolic function of subendocardial fibres allowed to distinguish trained athletes and patients with systemic hypertension.35 Left-ventricular torsion, a key determinant in LV function in cardiac diseases, has recently been analysed in the setting of exercise.18,36 In addition to the systolic twist, the subsequent early diastolic untwisting is an important marker of LV filling. Differently from patients with pathological LV hypertrophy who do not experience torsion/untwisting augmentation during exercise, LV torsion and untwisting rate have been shown to increase during laboratory-based submaximal exercise in healthy persons.18 In athletes, some discordant data have been reported and both increased or decreased torsion after training have been described depending on study population, study design, and measurement technique.36 We found a different behaviour of LV torsion after exercise in endurance and strength athletes since in marathon and martial arts athletes we found a baseline increase in peak systolic apical rotation that translated into a highly significant increase in peak systolic LV torsion after exercise. The same increase was not shown in power athletes. The underlying mechanisms responsible for this heterogeneous response of LV torsion are not well understood. Left-ventricular torsion results from a complex arrangement of wall myocardial fibres and its progressive increase during effort could reflect a higher contribution of subepicardial vs. subendocardial layers blunted by local ischaemia. Another explanation could be based on the regular decrease in LV enddiastolic diameters observed with exercise intensity that could enhance subepicardial layers. The current uncertainty regarding 1018 Table 4 A. Vitarelli et al. Changes of functional and echocardiographic parameters during maximal physical effort ETA (n 5 35) STA (n 5 35) MTA (n 5 35) CTR (n 5 35) 165.9 + 15. 4 180.2 + 13.7 168.8 + 12. 9 177.4 + 14. 2 0.04*, ,0.05† Maximal SBP (mmHg) Rate– pressure product (bpm × mmHg × 1023) 173.49 + 24.7 30.8 + 3.1 195.11 + 24.1 34.6 + 2.2 175.82 + 23.1 31.8 + 3.3 165.16 + 22.2 28.4 + 3.5 0.03*, 0.04† 0.03*, ,0.05† Maximal workload achieved (W) 207.42 + 33.9 173.31 + 30.8 197.18 + 36.5 157.13 + 35.3 0.02*, 0.03† 68 + 8 22.2 + 3.7 67 + 5 16.1 + 3.3 67 + 9 21.6 + 3.8 66 + 4 15.2 + 2.9 224.2 + 3.3 225.1 + 2.7 226.5 + 2.4 224.9 + 2.5 23.8 + 4.7 7.4 + 0.5 16.9 + 4.6 5.3 + 06 23.6 + 4.9 6.9 + 0.7 17.2 + 4.5 6.7 + 0.5 Bicycle ergometer P-value ............................................................................................................................................................................... Maximal HR (bpm) 3D-LVEF MV Ea (cm/s) LV Global LS (%) Peak LVtor (degrees) AoSvel (cm/s) 3D-RVEF TV Ea (cm/s) RV Global LS (%) 60 + 9 22.1 + 3.5 228.9 + 2.9 58 + 6 18.1 + 4.3 229.7 + 2.6 59 + 8 21.7 + 3.8 229.3 + 2.7 59 + 7 14.8 + 4.4 230.2 + 2.5 NS ,0.05‡ NS ,0.05‡ ,0.05§ NS ,0.05‡ NS AoSvel, aortic wall systolic velocity; CTR, controls; Ea, annular early diastolic velocity; EF, ejection fraction; HR, heart rate; LS, longitudinal strain; LV, left ventricle; LVtor, left-ventricular torsion; MV, mitral valve; NS, not significant; RV, right ventricle; SBP, systolic blood pressure; TV, tricuspid valve. *ETA vs. STA. † MTA vs. STA. ‡ ETA and MTA vs. CTR. § STA vs. CTR. For two-dimensional parameters, the greatest limitation was the effective frame rate which compromised frame-to-frame tracking of the fast contracting myocardium while for Doppler indices cardiac translation due to respiration increased the noise-to-signal ratio due to several artefacts. Although the superior temporal resolution of Doppler modalities is an advantage for exercise measures allowing these techniques to be more sensitive to dynamic changes, it has been shown39 they have a greater variability in quantification of myocardial values at all levels of exercise compared with two-dimensional methods. As regards 3D echocardiography, the resolution of the images was not as high as that obtained with conventional scanners, due to the lower frame rates that limited its feasibility. Another strong limitation to feasibility and reproducibility was high heart rates reached at the peak of the stress test. However, in this study as in previous reports,40 quantifications of left-ventricular volumes were reproducible also when heart rate was high or resting images of sub-optimal quality. Ao wall velocities and strain Elastic properties of the aorta29 are important factors supporting LV function. The functions of the aorta are not only those of a blood conduit for tissues, but also an important modulator of the entire cardiovascular system, which hinder cardiac intermittent pulsatile flow to provide a constant flow in the capillary bed. By virtue of its elastic properties, the aorta influences left-ventricular function and coronary flow. Previous studies5 have shown an increase in the elastic properties of these endurance athletes and several cardiovascular adaptations in power athletes related to intermittent elevations of blood pressure during exercise in muscle strength. It was also suggested that in these athletes, the transient increase in cardiac output associated with high elevation of systemic blood pressure may cause a chronic increase in wall tension responsible for aortic dilation and regurgitation. In a Downloaded from by guest on October 20, 2016 the significance of high resting LV torsion suggests that using these parameters to differentiate physiological and pathological LV remodelling is not feasible at the present time. The examination of LV torsion ‘reserve’ during exercise in athletes may provide further insight in the future. RV function assessment in athletes is important due to the possible overlap between athlete’s heart and ARVD especially in the presence of ventricular arrhythmias. Long-lasting RV volume overload could be the mechanism contributing to the development of RV structural changes leading to functional abnormalities. A number of studies using 2D echocardiography have demonstrated transient RV systolic dysfunction in response to high-intensity sports activity such as marathon running.22,37,38 It has been suggested37 that the adaptation to volume and pressure stress might spatially differ within the RV as a result of differences in wall stress between the apical and the inflow tract and that the basal portion of the RV might be more vulnerable and prone to preferential dilatation and reduced strain, or both. Our results are partially in concordance with these findings. The greater regional heterogeneity in RV strain compared with controls was more pronounced in endurance vs. power athletes and this seems to be related to increased pulmonary artery pressure as well as to ventricular dilatation. However, there was an improvement of RV strain after exercise with a behaviour similar to control subjects. One can speculate that these ‘normal’ responses would differ from those seen in patients with RV disease (such as ARVD or pulmonary hypertension) but it remains to be demonstrated that RV dysfunction is accentuated with exercise using these new echocardiographic techniques. The quantification of strain and strain rate as well as 3D ejection fraction during exercise has proved to be difficult in the present study as in previous reports.39 – 41 However, offline STI analysis was feasible in most subjects after strenuous levels of exercise. 1019 Assessment of biventricular function and aortic stiffness in athletes Limitations Some limitations should be pointed out. First, technical limitations of strain Doppler echocardiography should be considered. A technical limitation is that speckle-tracking echocardiography is dependent both on frame rate and image resolution. In addition, the endocardial border tracing must be manually optimized. We found frame rates in the range of 60 –100 Hz suitable for speckletracking analysis, that is a lower value than frame rate available with Doppler strain. However, STI may overcome some TDI limitations by assessing myocardial thickening in a manner less affected by passive translational motion or tethering. Also we have not directly estimated the exact distance between the two short-axis levels, which could have affected LV torsion measurements, nor have we selected reproducible anatomic landmarks for measuring apical rotation although we defined the apical level just proximal to the level with LV luminal obliteration at the end-systolic period.46 Furthermore, only one vessel bed (ascending aorta) was examined to assess aortic stiffness, whereas in different points the arterial wall distensibility may be different. Last, the accuracy of 3D volume and EF is related to the effects of endocardial trabeculae that play an important role in the intermodality discordances in LV volume measurements,2 and could certainly be expected to affect RV measurements even more, since the RV is more heavily trabeculated. Moreover, the accuracy of 3D volume and EF is less certain in significantly dilated right ventricles since limited data are available in the literature. Conclusions The combined application of 3DE, TDI, and STI has shown that ventricular and vascular response underlie different adaptations of ventricular volumes and arterial stiffness in strength-, endurance-, and mixed-trained athletes. Future studies in this direction with a larger sample size and longitudinal study design will certainly increase our knowledge of cardiovascular adaptation of the athletes. Conflict of interest: none declared. References 1. Maron BJ. Structural features of the athlete heart as defined by echocardiography. J Am Coll Cardiol 1986;7:190 – 203. 2. La Gerche A, Taylor AJ, Prior DL. Athlete’s heart: the potential for multimodality imaging to address the critical remaining questions. JACC Cardiovasc Imaging 2009; 2:350–63. 3. Bhella PS, Levine BD. The heart of a champion. J Am Coll Cardiol 2010;55:1626 –8. 4. Morganroth J, Maron BJ, Henry WL, Epstein SE. Comparative left ventricular dimensions in trained athletes. Ann Intern Med 1975;82:521 –4. 5. Otsuki T, Maeda S, Iemitsu M, Saito Y, Tanimura Y, Ajisaka R et al. Vascular endothelium-derived factors and arterial stiffness in strength- and endurancetrained men. Am J Physiol Heart Circ Physiol 2007;292:H786–91. 6. D’Andrea A, Caso P, Scarafile R, Salerno G, De Corato G, Mita C et al. Biventricular myocardial adaptation to different training protocols in competitive master athletes. Int J Cardiol 2007;115:342–9. 7. Fagard RH. Athlete’s heart: a meta-analysis of the echocardiographic experience. Int J Sports Med 1996;17(Suppl. 3):S140 –4. 8. Pluim BM, Zwinderman AH, van der Laarse A, van der Wall EE. The athlete’s heart. A meta-analysis of cardiac structure and function. Circulation 2000; 101:336–44. 9. Naylor LH, George K, O’Driscoll G, Green DJ. The athlete’s heart: a contemporary appraisal of the ‘Morganroth hypothesis’. Sports Med 2008;38:69 –90. 10. Maron BJ, Pelliccia A. The heart of trained athletes: cardiac remodeling and the risks of sports, including sudden death. Circulation 2006;114:1633 – 44. Downloaded from by guest on October 20, 2016 recent study,42 the aortic root diameter was significantly higher in power athletes than in endurance athletes matched for age and sex. However, a significant dilation of the ascending aorta and the presence of aortic regurgitation proved uncommon. Other studies43 have applied standard echocardiographic techniques to the assessment of elastic properties and diameters in top-level athletes and shown that aortic root diameters and stiffness were significantly greater in strength-trained athletes, while aortic distensibility was higher in endurance athletes compared with age- and sex-matched healthy controls. We have studied aortic wall distensibility as well as wall velocity and strain with tissue Doppler techniques. The aortic wall velocities and strain were significantly increased in endurance and martial arts athletes and significantly reduced in power athletes compared with controls. In power athletes, the decreased values persisted during maximal physical effort. These data can be interpreted as a result of a physiological ventricular–vascular coupling. The increase in aortic distensibility in marathon runners and athletes in martial arts can cause an improvement in LV diastolic function as a factor of physiological adaptation. In power athletes, the greater aortic stiffness has a potential correlation with the ventricular wall stress. In response to increased afterload or increased blood pressure, LV hypertrophy reflects a compensatory mechanism to decrease wall stress and these changes may be a cardiovascular adaptation of the isometric exercise in harmony with a normalization of systolic and diastolic function. It has been speculated that changes in wall thickness and lumen diameter may reflect adaptations consistent with the Law of Laplace and normalization of wall stress.44 The mechanism underlying the differences in arterial stiffness between endurance- and strength-trained athletes is not completely clear. It is possible that changes in vasoactive substances production, such as endothelin-1 (ET-1) and nitric oxide (NO), caused by exercise training could promote differential changes in arterial stiffness. Further investigation is required to assess the balance between training-induced changes in vasodilator and vasoconstrictor function and arterial remodelling. The advantages of the use of these new methodologies in patients with cardiovascular diseases and in athletes have been highlighted for each technique in previous studies.14,17,21,22,32,45 Three-dimensional echocardiography has been compared with MRI in the assessment of LV and RV volumes and LVEF/RVEF, demonstrating excellent intraobserver and interobserver reliability and a higher correlation compared with standard techniques.21,22,45 Other reports14,17 have pointed out the reliability of TDI and STI techniques to detect subclinical ventricular dysfunction and differentiate physiological from pathological hypertrophy since peculiar aspects of ventricular deformation and torsion cannot be assessed by using conventional echocardiographic techniques. With regard to vascular function, we have previously shown that TDI values in the ascending aorta had a higher discriminating power in differentiating hypertensive patients from controls.32 Our present data in athletes show that TDI values in the ascending aorta, while using a faster methodology to be applied, have a higher significancy in differentiating athletes from controls compared with stiffness index and distensibility assessed by M-mode echocardiography. 1020 28. Park SJ, Miyazaki C, Bruce CJ, Ommen S, Miller FA, Oh JK. Left ventricular torsion by two-dimensional speckle tracking echocardiography in patients with diastolic dysfunction and normal ejection fraction. J Am Soc Echocardiogr 2008;21:1129 –37. 29. Stefanadis C, Stratos C, Boudoulas H, Kourouklis C, Toutouzas P. Distensibility of the ascending aorta: comparison of invasive and non-invasive techniques in healthy men and in men with coronary artery disease. Eur Heart J 1990;11:990 –6. 30. Schmidt-Trucksass A, Grathwohl D, Schmid A, Boragk R, Upmeier C, Keul J et al. Assessment of carotid wall motion and stiffness with tissue Doppler imaging. Ultrasound Med Biol 1998;24:639–46. 31. Mottram PM, Haluska BA, Leano R, Carlier S, Case C, Marwick TH. Relation of arterial stiffness to diastolic dysfunction in hypertensive heart disease. Heart 2005;91:1551 –6. 32. Vitarelli A, Giordano M, Germanò G, Pergolini M, Cicconetti P, Tomei F et al. Assessment of ascending aorta wall stiffness in hypertensive patients by tissue Doppler imaging and strain Doppler echocardiography. Heart 2010;96:1469 –74. 33. Urhausen A, Monz T, Kindermann W. Echocardiographic criteria of physiological left ventricular hypertrophy in combined strength- and endurance-trained athletes. Int J Card Imaging 1997;13:43 –52. 34. Galderisi M, Lomoriello VS, Santoro A, Esposito R, Olibet M, Raia R et al. Differences of myocardial systolic deformation and correlates of diastolic function in competitive rowers and young hypertensives: a speckle-tracking echocardiography study. J Am Soc Echocardiogr 2010;23:1190 –8. 35. Butz T, van Buuren F, Mellwig KP, Langer C, Plehn G, Meissner A et al. Twodimensional strain analysis of the global and regional myocardial function for the differentiation of pathologic and physiologic left ventricular hypertrophy: a study in athletes and in patients with hypertrophic cardiomyopathy. Int J Cardiovasc Imaging 2011;27:91 –100. 36. Weiner RB, Hutter AM Jr, Wang F, Kim J, Weyman AE, Wood MJ et al. The impact of endurance exercise training on left ventricular torsion. JACC Cardiovasc Imaging 2010;3:1001 – 9. 37. Teske AJ, Prakken NH, De Boeck BW, Velthuis BK, Martens EP, Doevendans PA et al. Echocardiographic tissue deformation imaging of right ventricular systolic function in endurance athletes. Eur Heart J 2009;30:969 –77. 38. Poh KK, Ton-Nu TT, Neilan TG, Tournoux FB, Picard MH, Wood MJ. Myocardial adaptation and efficiency in response to intensive physical training in elite speedskaters. Int J Cardiol 2008;126:346 –51. 39. La Gerche A, Burns AT, D’Hooge J, Macisaac AI, Heidbuchel H, Prior DL. Exercise strain rate imaging demonstrates normal right ventricular contractile reserve and clarifies ambiguous resting measures in endurance athletes. J Am Soc Echocardiogr 2012;25:253 –62. 40. Pratali L, Molinaro S, Corciu AI, Pasanisi EM, Scalese M, Sicari R. Feasibility of realtime three-dimensional stress echocardiography: pharmacological and semisupine exercise. Cardiovasc Ultrasound 2010;8:10 –8. 41. Schattke S, Wagner M, Hättasch R, Schroeckh S, Durmus T, Schimke I et al. Single beat 3D echocardiography for the assessment of right ventricular dimension and function after endurance exercise: Intraindividual comparison with magnetic resonance imaging. Cardiovasc Ultrasound 2012;10:6–15. 42. Babaee Bigi MA, Aslani A. Aortic root size and prevalence of aortic regurgitation in elite strength trained athletes. Am J Cardiol 2007;100:528 – 30. 43. D’Andrea A, Cocchia R, Riegler L, Salerno G, Scarafile R, Citro R et al. Aortic stiffness and distensibility in top-level athletes. J Am Soc Echocardiogr 2012; 25:561 – 7. 44. Green DJ, Spence A, Rowley N, Thijssen DH, Naylor LH. Vascular adaptation in athletes: is there an ‘athlete’s artery’? Exp Physiol 2012;97:295 –304. 45. Vitarelli A, Sardella G, Di Roma A, Capotosto L, De Curtis G, D’Orazio S et al. Assessment of right ventricular function by three-dimensional echocardiography and myocardial strain imaging in adult atrial septal defect before and after percutaneous closure. Int J Cardiovasc Imag 2012;28:1905 –16. 46. Kim HK, Sohn DW, Lee SE, Choi SY, Park JS, Kim YJ et al. Assessment of left ventricular rotation and torsion with two-dimensional speckle tracking echocardiography. J Am Soc Echocardiogr 2007;20:45– 53. Downloaded from by guest on October 20, 2016 11. Fagard R, Van Den Broeke C, Bielen E, Vanhees L, Amery A. Assessment of stiffness of the hypertrophied left ventricle of bicyclists using left ventricular inflow Doppler velocimetry. J Am Coll Cardiol 1987;9:1250 –4. 12. Lewis JF, Spirito P, Pelliccia A, Maron BJ. Usefulness of Doppler echocardiographic assessment of diastolic filling in distinguishing ‘‘athlete’s heart’’ from hypertrophic cardiomyopathy. Br Heart J 1992;68:296 – 300. 13. Palka P, Lange A, Fleming AD, Donnelly JE, Dutka DP, Starkey IR et al. Differences in myocardial velocity gradient measured throughout the cardiac cycle in patients with hypertrophic cardiomyopathy, athletes and patients with left ventricular hypertrophy due to hypertension. J Am Coll Cardiol 1997;30:760 –8. 14. Vinereanu D, Florescu N, Schulthorpe N, Tweddel AC, Stephens MR, Fraser AG. Differentiation between pathologic and physiologic left ventricular hypertrophy by tissue Doppler assessment of long-axis function in patients with hypertrophic cardiomyopathy or systemic hypertension and in athletes. Am J Cardiol 2001; 88:53 –8. 15. D’Andrea A, Caso P, Galderisi M, Di Maggio D, Cicala S, D’Andrea L et al. Assessment of myocardial response to physical exercise in endurance competitive athletes by pulsed Doppler tissue imaging. Am J Cardiol 2001;87:1226 –30. 16. Butz T, van Buuren F, Mellwig KP, Langer C, Oldenburg O, Treusch KA et al. Systolic and early diastolic left ventricular velocities assessed by tissue Doppler imaging in 100 top-level handball players. Eur J Cardiovasc Prev Rehabil 2010; 17:342–8. 17. Richand V, Lafitte S, Reant P, Serri K, Lafitte M, Brette S et al. An ultrasound speckle tracking (two-dimensional strain) analysis of myocardial deformation in professional soccer players compared with healthy subjects and hypertrophic cardiomyopathy. Am J Cardiol 2007;100:128 –32. 18. Doucende G, Schuster I, Rupp T, Startun A, Dauzat M, Obert P et al. Kinetics of left ventricular strains and torsion during incremental exercise in healthy subjects: the key role of torsional mechanics for systolic-diastolic coupling. Circ Cardiovasc Imaging 2010;3:586 –94. 19. Simsek Z, Gundogdu F, Alpaydin S, Gerek Z, Ercis S, Sen I et al. Analysis of athletes’ heart by tissue Doppler and strain/strain rate imaging. Int J Cardiovasc Imaging 2011;27:105 –11. 20. Mor-Avi V, Jenkins C, Kühl HP, Nesser HJ, Marwick T, Franke A et al. Real-time 3-dimensional echocardiographic quantification of left ventricular volumes: multicenter study for validation with magnetic resonance imaging and investigation of sources of error. JACC Cardiovasc Imaging 2008;1:413 – 23. 21. Caselli S, Di Paolo FM, Pisicchio C, Di Pietro R, Quattrini FM, Di Giacinto B et al. Three-dimensional echocardiographic characterization of left ventricular remodeling in Olympic athletes. Am J Cardiol 2011;108:141 –7. 22. Oomah SR, Mousavi N, Bhullar N, Kumar K, Walker JR, Lytwyn M et al. The role of three-dimensional echocardiography in the assessment of right ventricular dysfunction after a half marathon: comparison with cardiac magnetic resonance imaging. J Am Soc Echocardiogr 2011;24:207 –13. 23. Lang RM, Bierig M, Devereux RB, Flachskampf FA, Foster E, Pellikka PA et al. Recommendations for chamber quantification: a report from the American Society of Echocardiography’s Guidelines and Standards Committee and the Chamber Quantification Writing Group, developed in conjunction with the European Association of Echocardiography, a branch of the European Society of Cardiology. J Am Soc Echocardiogr 2005;18:1440 –63. 24. Devereux RB, Alonso DR, Lutas EM, Gottlieb GJ, Campo E, Sachs I et al. Echocardiographic assessment of left ventricular hypertrophy: comparison to necropsy findings. Am J Cardiol 1986;57:450 –8. 25. Quinones MA, Otto CM, Stoddard M, Waggoner A, Zoghbi WA. Recommendations for quantification of Doppler echocardiography: a report from the Doppler quantification task force of the nomenclature and standards committee of the American Society of Echocardiography. J Am Soc Echocardiogr 2002;15:167–84. 26. Nagueh SF, Appleton CP, Gillebert TC, Marino PN, Oh JK, Smiseth OA et al. Recommendations for the evaluation of left ventricular diastolic function by echocardiography. J Am Soc Echocardiogr 2009;22:107–33. 27. Nagueh SF, Bhatt R, Vivo RP, Krim SR, Sarvari SI, Russell K et al. Echocardiographic evaluation of hemodynamics in patients with decompensated systolic heart failure. Circ Cardiovasc Imaging 2011;4:220 –7. A. Vitarelli et al.