Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
Cardiac contractility modulation wikipedia , lookup
Coronary artery disease wikipedia , lookup
Electrocardiography wikipedia , lookup
Cardiac surgery wikipedia , lookup
Myocardial infarction wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Mitral insufficiency wikipedia , lookup
Congenital heart defect wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
Lutembacher's syndrome wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
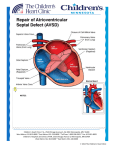
Atrioventricular
Septal Defects
Mary T. Donofrio MD, FAAP, FACC, FASE
Professor of Pediatrics
Director of the Fetal Heart Program
Director of the Critical Care Delivery Program
Children’s National Health System
Washington DC
Objectives
Discuss the etiology and associations for AVSD
Review the sonographic features of AVSD
Review cases of AVSD, including those with
associated cardiac anomalies to understand the
spectrum of the disease
Learn the clinical and anatomic features that
impact outcome in patients born with AVSD
Atrioventricular Septal Defect (AVSD)
Synonyms
• Atrioventricular canal defect (AVCD)
• Complete common atrioventricular canal defect (CCAVC)
• Endocardial cushion defect
Epidemiology
• 0.3-0.55/1000 live births
• 17% of prenatal CHD
Embryology
• Deficiency in the AV septum believed
to be caused by an abnormal or
inadequate fusion of the superior and
inferior endocardial cushions with the
mid portion of the atrial septum and
the muscular inlet portion of the
ventricular septum
AVSD: Subtypes
Complete
Normal
• Primum ASD, large inlet VSD
• Common AV valve annulus
Transitional
Complete
• Primum ASD, restrictive inlet VSD
• Common AV valve with fused
bridging leaflets and 2 distinct
valves
Incomplete/Partial
• Primum ASD, no VSD
• Separate tricuspid valve and cleft
mitral valve
Incomplete
Genetic Associations
Trisomy 21 (Multiple sources)
• 45% of children with trisomy 21 have CHD; of these, 35–40%
have AVSD
• 1/3 of all children with AVSDs also have trisomy 21
• Defect usually a “complete” AVSD
Noonan’s Syndrome (Marino B, 1999)
• Increased risk of AVSD
• Defect usually a "partial" AVSD
TBX2 (Harrelson Z, 2004)
• Transcription factor, involved in development of outflows and
AV canal
• Mice homozygous null (-/-) died due to insufficient formation
of the endocardial cushion and left ventricle
Genetic Associations / Extracardiac Anomalies
Study of 301 fetuses
• 218 had known karyotype
86 (39%) had trisomy 21
21 (10% )had other abnormalities
• Isolated AVSD more likely to have abnormal karyotype
(62.5%) vs. complex AVSD
• Karyotype association
Normal in most with heterotaxy (50/52)
Abnormal in most with normal atrial situs (105/165)
• Extracardiac abnormality identified in 40/301 (13%)
Huggon IC, JACC 2000
Genetic Associations / Extracardiac Anomalies
Study of 246 fetuses
• 7 (3%) had an isolated AVSD
with no other cardiac/extracardiac
abnormalities
• 16 (7%) had an isolated
cardiac defect (complex AVSD)
without extracardiac abnormalities
•
•
•
•
129 (52%) with chromosome abnormality
72 (29%) with heterotaxy
17 (7%) syndromic
5 (2%) with an extracardiac abnormalities
Berg C, Ultraschall in Med 2009
AVSD
AVSD: ASD and VSD Subtypes
AVSD: The Common Valve
RSL
SBL
LLL
IBL
RLL
AVSD: Valve Anatomy
AVSD: Fetal/Postnatal AVV Regurgitation
49 fetuses, assessment of AVVR
AVVR Grade
• 0= none
• 1= insignificant
• 2= hemodynamically important
Results
•
•
•
•
69% - no change
8% - decreased
22% - increased
Only 5 (10%) progressed to 2
Fetal AVVR predictive of postnatal
Heterotaxy, trisomy 21 not at
increased risk
Davey B, Ped Cardiol 2013
AVSD: AV Connection
Normal
RA
RV
RA
LA
Common
AV inlet
RV
LV
Balanced
LA
RA
LV
RV
Atretic AV inlet
LA
LV
Unbalanced
RA
RV
LA
LV
RA
RV
LA
LV
Unbalanced
AVSD
AVSD: Mild Unbalance, Right Side Dominant
AVSD: Unbalanced, Right Side Dominant
AVSD: Unbalanced, Left Side Dominant
AVSD: Associated Cardiac Anomalies
Segmental
301 fetusesAnatomy Assessment
••
•
•
Atria: Visceral/atrial situs
Atria
Normal 67%
Ventricles
Left isomerism 20% / Right isomerism 12%
Great
arteries
Inverted
2%
• Ventricles: AV connection (balanced vs unbalanced)
Normal 69%
Right dominant 20%/ Left dominant 11%
• Great arteries
Normal 73%
Discordant 2%
DORV 24%
Single outlet <1%
(Pulmonary obstruction 13%)
Huggon IC, JACC 2000
Associated Cardiac Anomalies
246 fetuses
Additional cardiac
abnormality present in
109 (44%)
• Additional defects
positively correlated with
heterotaxy syndromes
(p < 0.01)
• Additional defects
negatively correlated with
aneuploidies, including
trisomy 21 (p < 0.01)
Berg C, Ultraschall in Med 2009
Associated Cardiac Anomalies
Berg C, Ultraschall in Med 2009
AVSD: Coarctation
AVSD: Tetralogy of Fallot
AVSD: Unbalanced, DORV with PA
AVSD and Heterotaxy
71 fetuses (48 LAI, 23 RAI)
Taketazo M, Am J Cardiol 2006
AVSD and Heterotaxy
81 patients with heterotaxy/ 43 prenatal dx (53%)
Ann Thor Surg 2006
Cohen M, Ann Thor Surg 2006
AVSD: Heterotaxy/ Right Isomerism
•
•
•
•
•
•
•
Levocardia, right stomach
Bilateral RA appendages
Ventricular inversion
Unbalanced AVSD, small LV
IVC to LA/ SVC to RA
DORV/PA {A,L,L}
TAPVR to ascending vein
L
R
AVSD: Heterotaxy/ Left Isomerism
•
•
•
•
•
•
Dextrocardia, left stomach
Bilateral LA appendages
Ventricular inversion
Unbalanced AVSD, small LV
DORV/PS {A,L,L}
Interrupted IVC with
azygous to SVC
L
R
Heterotaxy: Complete Heart Block
a
v
a
a
v
a
a
v
Heterotaxy: Pleural Effusion/ Early Hydrops
• Dextrocardia,
rightward stomach
• AVSD, unbalanced left
dominant
• DORV/PA {A,L,L}
• TAPVR
• SVC to RA, Bil IVC
AVSD: Surgery
AVSD: Outcome
301 fetuses, 178 terminated
N= 123 overall with intent to continue
• Live birth- 82%
• 3 year survival- 38%
Huggon IC, JACC 2000
N= 43 with isolated AVSD and intent
to continue
• Live birth- 81%
• 3 year survival- 55%
AVSD: Outcome
Improved outcome
• No hydrops
• No extracardiac defect (trend)
Huggon IC, JACC 2000
AVSD: Outcome
246 fetuses
Survival:
• Overall survival- 20%
58.5% terminated
7% died in-utero/neonatal
period
8% died in infancy
• Survival excluding lethal
malformations- 65%
• Trisomy 21 had better
survival and more likely to
have 2V repair
Berg C, Ultraschall in Med 2009
AVSD: Outcome
106 fetuses
• 88 with outcome data
Overall survival = 47%
Survival in those with
intent to continue (n=60)
= 69%
Presence of chromosomal
abnormality did not affect
mortality (p = 0.34)
Beaton AZ, JASE 2013
AVSD: Outcome
Situs Solitus vs. Heterotaxy
AVSD: Outcome
Decreased survival
• Heterotaxy
• Unbalanced AVSD
AVSD: Outcome
Mortality data
• Most deaths after SV type surgery
AVSD: Outcome
Balanced AVSD with complex CHD associated with SV repair
• 4/7 had SV repair vs. none in the isolated AVSD group
Unbalanced AVSD associated with SV repair 12/17(71% )
• 2V repair performed more often with restrictive VSD 5/7 (71%)
AVSD: Outcome
In-Utero Progression
• Unbalanced AVSD (16)
• 12 had no change in LAVV/RAVV ratio through gestation
AVSD: Outcome
SV repair more likely
• Unbalanced AVV
• In the presence of additional complex heart disease
2V repair
• May be more likely if the VSD is restrictive even with
unbalanced AVV
Poor outcome is associated with
•
•
•
•
Heterotaxy
Unbalanced ventricles
Need for SV repair
Not associated with trisomy 21
Conclusions
AVSD is associated with significant mortality, even
after accounting for termination of pregnancy
Isolated AVSD have the best chance of good
outcome even in the presence of trisomy 21
Associated defects including heterotaxy,
unbalanced AVV, and additional complex disease
increases the risk
Detailed and accurate prenatal imaging is
imperative for effective parental counseling and
postnatal surgical planning