Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Remote ischemic conditioning wikipedia , lookup
Heart failure wikipedia , lookup
Hypertrophic cardiomyopathy wikipedia , lookup
Cardiac surgery wikipedia , lookup
Myocardial infarction wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Ventricular fibrillation wikipedia , lookup
Quantium Medical Cardiac Output wikipedia , lookup
Arrhythmogenic right ventricular dysplasia wikipedia , lookup
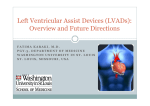
Left ventricular assist device management in patients chronically supported for advanced heart failure Jennifer Cowgera, Matthew A. Romanob, John Stulakb, Francis D. Paganib and Keith D. Aaronsona a Division of Cardiovascular Medicine and bSection of Cardiac Surgery, University of Michigan Health System, Ann Arbor, Michigan, USA Correspondence to Jennifer Cowger, MD, MS, University of Michigan Cardiovascular Center, 1500 E. Medical Center Drive, SPC 5853, Ann Arbor, MI 48109-5853, USA Tel: +1 734 936 5265; e-mail: [email protected] Current Opinion in Cardiology 2011, 26:149–154 Purpose of review This review summarizes management strategies to reduce morbidity and mortality in heart failure patients supported chronically with implantable left ventricular assist devices (LVADs). Recent findings As the population of patients supported with long-term LVADs has grown, patient selection, operative technique, and patient management strategies have been refined, leading to improved outcomes. This review summarizes recent findings on LVAD candidate selection, and discusses outpatient strategies to optimize device performance and heart failure management. It also reviews important device complications that warrant close outpatient monitoring. Summary Managing patients on chronic LVAD support requires regular patient follow-up, multidisciplinary care teams, and frequent laboratory and echocardiographic surveillance to ensure optimal outcomes. Keywords end-stage heart failure, left ventricular assist device, patient management Curr Opin Cardiol 26:149–154 ß 2011 Wolters Kluwer Health | Lippincott Williams & Wilkins 0268-4705 Introduction In 1963, Dr Domingo Liotta at Baylor University College of Medicine implanted the first left ventricular assist device (LVAD) for the management of postcardiotomy shock in a patient who had undergone double valve surgery [1]. After support on the Liotta-DeBakey LVAD for 10 days at a flow of 1200 ml/min, the patient recovered myocardial function. This pivotal experience foreshadowed a new era of heart failure management employing long-term mechanical circulatory support. With minimal improvements made over the last 20 years in posttransplant survival (50% at 10 years) [2] and the burdens and complications of the required posttransplant medical regimen, it is not unrealistic to envision a future where mechanical circulatory support is deemed preferable to transplant by many patients and physicians. Although still in its infancy in 2011, mechanical circulatory support has already rapidly evolved. LVAD manufacturers have improved device size, fluid dynamics, durability, and battery life. Patient selection, surgical technique, and postoperative patient management continue to be refined, reducing the frequency of device complications, patient morbidity and mortality. In the destination therapy population, for whom 1-year survival 0268-4705 ß 2011 Wolters Kluwer Health | Lippincott Williams & Wilkins in the medical arm of the REMATCH trial was 25%, survival of advanced heart failure destination therapy patients supported with a HeartMate XVE LVAD was improved to 52% [3]. In the continuous flow device arm of the HeartMate II Destination Therapy trial, destination therapy survival was further extended to 68% at 1 year [4]. While the greatest hazard for mortality with LVAD therapy will likely always be the early perioperative period, the cumulative hazard for death on LVAD support has not plateaued in any major trial or registry analysis to date. Thus, to ensure the best outcomes for our patients on chronic LVAD support, frequent outpatient follow-up and vigilant device, driveline, and heart failure management are obligatory. This review will discuss the important complications faced by patients on chronic LVAD support and means of reducing the risk for such complications. Early postoperative management The operative period imparts the greatest risk for death following LVAD implantation. In the second annual report of the Interagency Registry for Mechanical Circulatory Support (INTERMACS), 3-month mortality for DOI:10.1097/HCO.0b013e3283438258 150 Heart failure Figure 1 Survival and hazard for death and survival by device strategy (a) Survival after primary LVAD Intermacs : June 2006 – March 2009 Primary LVAD: n = 1092, deaths = 191 0.20 Deaths/month % Survival 100 0.18 (hazard) Survival 80 0.16 0.14 0.12 60 0.10 Month % Survival 3 mo 88% 6 mo 83% 12 mo 74% 24 mo 55% 40 20 0.08 0.06 Hazard 0.04 0.02 0 Event: Death (censored at transplant or recovery) 0 3 6 9 12 15 18 21 0.00 24 Months after device implant (b) Device strategy at implant Intermacs : June 2006 – March 2009 Primary LVAD: n = 1092 % Survival 100 90 BTT = 496, deaths = 54 80 BTC = 458, deaths = 92 70 DT = 100, deaths = 39 60 50 40 Month 3 mo 6 mo 12 mo 30 20 10 0 BTT 91% 90% 84% BTC 85% 78% 72% DT 85% 72% 64% P < 0.0001 Event: Death (censored at transplant or explant recovery) 0 3 6 9 12 15 18 21 24 Months after device implant (a) Survival and hazard for death after left ventricular assist device (LVAD) implant in INTERMACS. Kaplan–Meier estimates for survival following LVAD implant in 1092 patients enrolled into INTERMACS are shown. All patients underwent implant of Food and Drug Administration-approved LVADs. At the bottom, the cumulative hazard for mortality (censoring for transplant or recovery) is also shown. (b) Survival by device strategy following LVAD implant in INTERMACS. Kaplan–Meier estimates of survival according to intended device strategy [bridge to transplant (BTT), destination therapy (DT), bridge to candidacy (BTC)] is shown for patients undergoing LVAD implant in INTERMACS. Reproduced with permission from [5 ]. the 1283 patients undergoing primary LVAD implant between 2006 and 2009 was 12% (Fig. 1a) [5]. Operative survival was lower in those with advanced age, preoperative cardiogenic shock (requiring vasopressors or preoperative temporary mechanical support), evidence of right ventricular dysfunction, and those for whom the intended device strategy was not bridge to transplant (i.e., destination therapy or bridge to candidacy) (Fig. 1b) [5]. In other studies, risks for death and morbidity in the LVAD perioperative period include requirements for preoperative ventilator support [6,7], high perioperative transfusion requirements and/or coagulopathy [6,8,9], and the development of renal failure following LVAD implant [10]. Thus, early LVAD survival relies on careful patient selection and vigilant perioperative management. Left ventricular assist device candidate selection Patient selection is paramount for success after LVAD support and this has been the subject of prior review [11,12]. The Lietz–Miller destination therapy risk score was developed from 222 individuals undergoing HeartMate XVE implant for destination therapy and may be useful for distinguishing destination therapy candidates at high risk for poor outcome on LVAD support [13]. The validity of this score in the bridge to transplant or ‘less ill’ population, as well as those on more contemporary devices, warrants investigation. Perioperative management Strategies to reduce right ventricular failure, bleeding, and infection risks are the focus of perioperative LVAD and patient management. The authors refer readers to a Left ventricular assist device management Cowger et al. 151 prior review on pre and early postoperative LVAD management strategies to reduce right ventricular failure risks [14]. In addition to a vigilant intraoperative hemostatic technique [9], preemptive preoperative assessment of bleeding and right ventricular failure risk is important [8,15]. When possible, glycoprotein (GP)2b3a inhibitors and vitamin K antagonists should be discontinued well in advance of surgery and international normalized ratios (INRs) should be normalized. Measures to reduce hepatic congestion (diuresis, inotropes, right ventricular afterload reduction) and improve nutritional status should be undertaken. At the time of LVAD initiation, optimization of speeds/flows should be done with transesophageal echocardiogram guidance to minimize septal shift and, thereby, right ventricular wall stress. Early postoperative inotrope administration with close monitoring of cardiopulmonary hemodynamics is often beneficial for right ventricular support and to assist with management of mobilized intraoperative fluids. Reducing complications: management of the outpatient on long-term left ventricular assist device support Important complications following LVAD implant include infection, stroke, device thrombosis, gastrointestinal bleeding, and recurrent heart failure symptomatology with or without multisystem organ failure [16]. The University of Michigan (UofM) LVAD program’s strategy is to schedule monthly visits with LVAD patients until they are 6 months postoperative to allow laboratory, driveline line and volume status monitoring, LVAD speed optimization, and frequent patient and caregiver (re)education. After this point, return visits are extended to 2–3-month intervals unless complications arise. Heart failure management after left ventricular assist device implant Heart failure management after LVAD implant should include the application of standard American College of Cardiology/American Heart Association (ACC/AHA)recommended evidence-based medications for heart failure – angiotension inhibitors and receptor blockers (ARB), beta-blockers, and aldosterone antagonists [17]. In addition to offering a few patients the chance for myocardial recovery while on LVAD support, these medications work with the LVAD to reduce the activation of the renin–angiotensin–aldosterone system (RAAS) and sympathetic nervous system (SNS). The RAAS and SNS not only play critical roles in adverse myocardial remodeling that may impact long-term left ventricular and right ventricular performance; they also drive fluid retention and increase systemic afterload. Hydralazine and nitrate combination therapy can be added to the medical regimen of patients who are on maximal tolerated doses of the above medications, particularly in the setting of elevated pulmonary vascular resistance or systemic hypertension. Finally, studies have shown that ventricular arrhythmias occur at increased frequency following LVAD implant, especially in the early postoperative period when normal repolarization is disrupted by myocardial edema and inflammation [18,19,20]. In a prospective study of 61 patients with an implantable converter defibrillator (ICD) in place, 34% of patients supported for a mean of 365 days had an appropriate device intervention for a ventricular arrhythmia [19]. Thus, ICD prophylaxis should be strongly considered in patients undergoing LVAD support; it is standard practice at our center. Device management A discussion of device-specific speed/flow management for all LVAD models and manufacturers is beyond the scope of this paper. In general, care strategies aim to set device speeds/flows to optimize left ventricular preload and afterload while simultaneously avoiding perturbation of right ventricular wall stress. Continuous flow devices (especially centrifugal pumps) are very afterload sensitive and tight blood pressure control (goal mean arterial pressure 60– 90 mmHg) should be achieved to facilitate optimal device flows and reduce device power consumption. Echocardiography is a critical tool to guide LVAD speed/ flow optimization. Device settings should allow for decompression of the left ventricle (LV), leading to a reduction in left ventricular volumes and/or dimensions from preimplant measures. With appropriate LVAD flows/speeds, left ventricular afterload is reduced and, consequently, mitral regurgitation should be insignificant. The apical four chamber view is useful for visualization of the interventricular septum and the left ventricular inflow cannula. Leftward displacement of the septum induced by high LVAD inflows should be avoided due to the impact on right ventricular wall stress and potential for device-induced suction events. Doppler interrogation of the inflow cannula should be without turbulence. Elevated inflow velocities may suggest device thrombosis. Finally, there is growing evidence that aortic insufficiency tends to progress with the duration of LVAD support, potentially due to LVAD-induced shear-stress damage to the aortic root and the root side of the aortic valve [21,22]. While the clinical impact of aortic insufficiency on LVAD outcomes is not yet known, it could lead to ineffective LVAD output through blood recirculation. Thus, aortic insufficiency should be monitored in patients on LVAD support and device speeds may need to be adjusted accordingly if clinical heart failure is noted with aortic insufficiency progression. There is data to suggest that a fully opening aortic valve may have less of a 152 Heart failure propensity for developing regurgitation [21]. However, it is unclear at this time whether optimizing device speeds to ensure regular valve opening will prevent the development of aortic insufficiency. A regularly opening valve will reduce the likelihood of leaflet fusion, and maintenance of normal aortic valve operation is likely important for those in whom myocardial recovery is anticipated. The risk of development of aortic root thrombosis is also lessened in the setting of intermittent aortic valve opening. Infection Until a fully implantable technology is available, infection will remain the biggest obstacle to the success of truly long-term LVAD support. The hazard for sepsis is highest in the early postoperative period but never reaches zero, and infection is associated with a marked reduction in LVAD survival [16,23,24,25]. In the REMATCH trial, freedom from sepsis at 1 year in HeartMate XVE-supported patients was 58%, and 1-year survival in those with sepsis was 38% compared with 60% in those without. Device-related infections without septicemia are also prevalent and offer little better prognosis. In the 465 patients supported with pulsatile pumps in an INTERMACS (2006–2008) analysis, the infection rate at 12 months was 1.99 events per patient [24]. In the HeartMate II Destination Therapy trial, LVAD-related infections (pump, pump pocket, driveline) occurred at rates of 0.48 and 0.90 events/patient-year for HeartMate II and HeartMate XVE devices, respectively [4]. Case series have demonstrated that 60–70% of patients with a driveline infection require further surgical intervention, and 20–35% progress to pump infections requiring either urgent transplant or pump exchange [25,26]. Correlates of driveline infection include duration of LVAD support [26], known driveline trauma [26], and larger body mass index [27,28]. While studies have suggested that HeartMate XVE devices are associated with higher risk for driveline infection compared with the HeartMate II [4,28], a recent report suggests that patient characteristics and implant era may confound the interpretation of these prior nonadjusted analyses [29]. Further, the association between driveline infections and pump pocket infections is anticipated to be much less frequent with the HeartWare HVAD device, as this intrapericardially positioned device does not have an abdominal pump pocket. To reduce infectious complications, patient education on driveline care and infection warning signs is important. Education should encompass aseptic driveline cleansing techniques (which can rarely be performed by the patient alone) and appropriate driveline fixation using an abdominal binder and Velcro driveline ‘lead locks’. Our patients are instructed to wear their binder 24 h a day due to the risk for driveline disruption during sleep. Patients should be educated on avoiding activities that may lead to driveline displacement or bandage soiling. Antimicrobial prophylaxis administered in the perioperative period is targeted at culprit Gram-positive organisms (Staphylococcus species) as well as certain Gram-negative (Pseudomonas, Serratia) and fungal (Candida) pathogens. The duration of postoperative antimicrobial therapy and specific regimens administered are heterogeneous across LVAD institutions. Most will continue oral therapy until full driveline incorporation, which occurs between 3 and 6 months postoperative. At UofM, we use dual therapy (doxycycline and a fluoroquinolone) until the driveline is incorporated and then continue therapy with a single agent thereafter. For some destination therapy patients felt to be at high risk for infection, dual therapy may be continued indefinitely, but there is no evidence-based data to support either practice. Balancing bleeding risk with thrombosis and thrombotic complications Anticoagulation and antiplatelet therapy are required for most LVADs due to the potential for in-situ device thrombus formation and cardioembolic complications. For the HeartMate II device, rates of device thrombosis in the major trials were very low (0.02–0.03 events/ patient-year), with rates of ischemic stroke ranging from 0.06 to 0.13 events/patient-year [4,30]. No patient in the XVE arm of the HeartMate II Destination Therapy trial had a device thrombosis, and ischemic stroke rates were 0.10 events/patient-year [4]. In the outpatient setting, close monitoring of INRs, serum lactic acid dehydrogenase, serum free hemoglobin, bilirubin, and hematocrit levels is important. INTERMACS defines clinically significant hemolysis as a serum free hemoglobin more than 40 mg/dl more than 72 h after device implant with other clinical signs [31]. Whether other thresholds or other markers of hemolysis are more sensitive/specific for predicting adverse events is unknown. The low thrombotic event rates discussed above come at increased risks for bleeding complications, even in patients on HeartMate XVE support for whom warfarin is not required. In addition to pharmacologic-induced bleeding diathesis, LVAD support has been shown to impact hemostasis. Acquired von Willebrand syndrome with a reduction in von Willebrand factor (vWF) high molecular weight multimers has been well characterized and tends to onset early (as soon as 24 h) after LVAD support, resolving upon device explant [32,33,34]. Other LVAD-induced changes in the coagulation system include a reduction in factors XI and XII and an increase in markers of fibrinolysis [35]. In the major trials, bleeding requiring blood product transfusion occurred Left ventricular assist device management Cowger et al. 153 in 42–81% of patients and bleeding requiring surgery occurred in 15–30% of LVAD patients [3,4,30]. Hemorrhagic stroke rates range from 0.05 to 0.11 events/patientyear [3,4,30]. Of growing concern are complications from gastrointestinal bleeding. Similarly to Heyde’s syndrome in aortic stenosis, patients on LVAD support can develop gastrointestinal arteriovenous malformations with high propensity for bleeding due to acquired vWF deficiency. Cohort studies show a cumulative incidence of gastrointestinal bleeding ranging from 32% (mean patient follow-up 371 days) to 40% (follow-up unknown) with a mean time to first bleed of 112 and 87 days, respectively [32,36]. Angiodysplastic bleeds can occur anywhere in the gastrointestinal tract, tend to be recurrent, and carry associated burdens of blood transfusion and allosensitization risk. Compared with pulsatile flow devices, the risk for angiodysplasia development appears to be higher in patients supported with continuous flow LVADs, but further studies are underway [36,37]. Unfortunately, there is no known intervention to prevent or reduce gastrointestinal bleeding risk. Patient and family education Because patient device management is integral to LVAD success, one of the most important components of outpatient management is education. In addition to the extensive inpatient education provided after LVAD implant, re-education in the outpatient arena is key. Patients and caregivers should receive frequent reviews on (1) device alarms; (2) proper battery management: changing batteries, carrying back up batteries, purchasing an electric generator for emergency use; (3) aseptic driveline care and occlusive bandaging; (4) driveline fixation: proper positioning and sizing of the abdominal binder, proper fixation of leads to avoid fracture, high-risk activities that may increase driveline infection risk; (5) controller fixation; (6) signs and symptoms of gastrointestinal bleeding. intervention, 24–7 access to physicians or physician extenders who specialize in LVAD care is essential for patients and outside practitioners. Acknowledgements Disclosures for Drs Aaronson and Pagani – Both doctors have relationships with HeartWare (unpaid) and Terumo as members of Clinical Steering Committees. Dr Aaronson’s interactions with HeartWare and Thoratec are regulated by Conflict Management Plans on file with the University of Michigan’s Conflict of Interest Board. The other doctors have nothing to disclose. References and recommended reading Papers of particular interest, published within the annual period of review, have been highlighted as: of special interest of outstanding interest Additional references related to this topic can also be found in the Current World Literature section in this issue (p. 173). 1 Rodriquez L, Pereyra D, Trotta G. Biography of Professor Domingo S. Liotta, MD. http://www.fdliotta.org/curriculum.htm. [Accessed 14 October 2010] 2 Stehlik J, Edwards LB, Kucheryavaya AY, et al. The Registry of the International Society for Heart and Lung Transplantation: twenty-seventh official adult heart transplant report – 2010. J Heart Lung Transplant 2010; 29:1089–1103. 3 Rose EA, Gelijns AC, Moskowitz AJ, et al. Long-term mechanical left ventricular assistance for end-stage heart failure. N Engl J Med 2001; 345:1435–1443. Slaughter MS, Rogers JG, Milano CA, et al. Advanced heart failure treated with continuous-flow left ventricular assist device. N Engl J Med 2009; 361:2241–2251. This is the landmark study comparing outcomes with the Heartmate II vs. the XVE LVAD in patients supported for destination therapy. 4 Kirklin JK, Naftel DC, Kormos RL, et al. Second INTERMACS annual report: more than 1,000 primary left ventricular assist device implants. J Heart Lung Transplant 2010; 29:1–10. This report summarizes morbidity and mortality for patients enrolled to date into INTERMACS, a Food and Drug Administration-mandated database of currently approved mechanical support outcomes. It is one of the largest LVAD database analyses to date. 5 6 Rao V, Oz MC, Flannery MA, et al. Revised screening scale to predict survival after insertion of a left ventricular assist device. J Thorac Cardiovasc Surg 2003; 125:855–862. 7 Oz MC, Goldstein DJ, Pepino P, et al. Screening scale predicts patients successfully receiving long-term implantable left ventricular assist devices. Circulation 1995; 92:II169–II173. Matthews JC, Pagani FD, Haft JW, et al. Model for end-stage liver disease score predicts left ventricular assist device operative transfusion requirements, morbidity, and mortality. Circulation 2010; 121:214–220. Cohort study examining postoperative bleeding risk and associated morbidity and mortality in LVAD candidates. 8 9 Conclusion LVAD therapy offers patients with advanced heart failure improved survival and quality of life. To ensure that greatest benefits are gained from LVAD support for the longest duration necessary, careful heart failure, driveline, and device management are key. A multidisciplinary approach to patient care that includes cardiac surgeons, heart failure specialists, infectious disease consultants, and social work are vital to the success of an LVAD program and patient outcomes. Clinic visits should be frequent and should include patient and caregiver education with frequent attempts at re-education. Due to the complexity of LVAD management and the present ‘novelty’ of the Goldstein DJ, Beauford RB. Left ventricular assist devices and bleeding: adding insult to injury. Ann Thorac Surg 2003; 75:S42–S47. 10 Morgan J. Impact of acute renal failure on survival after HM II LVAD implanta tion. J Heart Lung Transplant 2010; 29:S178. This study demonstrates very poor outcome in patients with renal failure after LVAD implant. 11 Lund LH, Matthews J, Aaronson K. Patient selection for left ventricular assist devices. Eur J Heart Fail 2010; 12:434–443. Summary of current data on LVAD candidate risk stratification. 12 Miller LW, Lietz K. Candidate selection for long-term left ventricular assist device therapy for refractory heart failure. J Heart Lung Transplant 2006; 25:756–764. 13 Lietz K, Long JW, Kfoury AG, et al. Outcomes of left ventricular assist device implantation as destination therapy in the post-REMATCH era: implications for patient selection. Circulation 2007; 116:497–505. 14 Romano MA, Cowger J, Aaronson KD, et al. Diagnosis and management of right-sided heart failure in subjects supported with left ventricular assist devices. Curr Treat Options Cardiovasc Med 2010; 12:420–430. Review article discussing preoperative diagnosis and postoperative management of right ventricular failure. 154 Heart failure 15 Matthews JC, Koelling TM, Pagani FD, et al. The right ventricular failure risk score a preoperative tool for assessing the risk of right ventricular failure in left ventricular assist device candidates. J Am Coll Cardiol 2008; 51:2163–2172. 26 Zierer A, Melby SJ, Voeller RK, et al. Late-onset driveline infections: the Achilles’ heel of prolonged left ventricular assist device support. Ann Thorac Surg 2007; 84:515–520. 16 Pagani FD, Miller LW, Russell SD, et al. Extended mechanical circulatory support with a continuous-flow rotary left ventricular assist device. J Am Coll Cardiol 2009; 54:312–321. This report provides longer-term follow-up of quality of life, infection risk, and survival of patients supported with a HeartMate II LVAD for the bridge to transplant indication enrolled into the HeartMate II bridge to transplant trial. 27 Raymond AL, Kfoury AG, Bishop CJ, et al. Obesity and left ventricular assist device driveline exit site infection. ASAIO J 2010; 56:57–60. 17 Jessup M, Abraham WT, Casey DE, et al. 2009 focused update: ACCF/AHA Guidelines for the Diagnosis and Management of Heart Failure in Adults: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines: developed in collaboration with the International Society for Heart and Lung Transplantation. Circulation 2009; 119:1977–2016. 18 Harding JD, Piacentino V 3rd, Rothman S, et al. Prolonged repolarization after ventricular assist device support is associated with arrhythmias in humans with congestive heart failure. J Card Fail 2005; 11:227–232. 19 Oswald H, Schultz-Wildelau C, Gardiwal A, et al. Implantable defibrillator therapy for ventricular tachyarrhythmia in left ventricular assist device patients. Eur J Heart Fail 2010; 12:593–599. This study characterizes the burden of dysrhythmias in LVAD-supported patients. 20 Ziv O, Dizon J, Thosani A, et al. Effects of left ventricular assist device therapy on ventricular arrhythmias. J Am Coll Cardiol 2005; 45:1428–1434. 21 Cowger J, Pagani FD, Haft JW, et al. The development of aortic insufficiency in LVAD supported patients. Circ Heart Fail 2010; 3:668–674. This cohort study characterizes the progression of aortic insufficiency in LVADsupported patients and potential mechanisms behind its development. 22 Pak SW, Uriel N, Takayama H, et al. Prevalence of de novo aortic insufficiency during long-term support with left ventricular assist devices. J Heart Lung Transplant 2010; 29:1172–1176. Cohort study examining the progression of aortic insufficiency in LVAD-supported patients. 23 Holman WL, Park SJ, Long JW, et al. Infection in permanent circulatory support: experience from the REMATCH trial. J Heart Lung Transplant 2004; 23:1359–1365. 24 Holman WL, Kirklin JK, Naftel DC, et al. Infection after implantation of pulsatile mechanical circulatory support devices. J Thorac Cardiovasc Surg 2010; 139:1632.e2–1636.e2. This study reviews the incidence of device infections and correlates of infection development in patients supported with pulsatile devices. 25 Topkara VK, Kondareddy S, Malik F, et al. Infectious complications in patients with left ventricular assist device: etiology and outcomes in the continuousflow era. Ann Thorac Surg 2010; 90:1270–1277. 28 Martin SI, Wellington L, Stevenson KB, et al. Effect of body mass index and device type on infection in left ventricular assist device support beyond 30 days. Interact Cardiovasc Thorac Surg 2010; 11:20–23. 29 Schaffer JM, Allen JG, Weiss ES, et al. Infectious complications after pulsatile flow and continuous-flow left ventricular assist device implantation. J Heart Lung Transplant 2010. [Epub ahead of print] This study reviews the incidence of device infections and suggests that era of device may play a major role in infection risk. 30 Miller LW, Pagani FD, Russell SD, et al. Use of a continuous-flow device in patients awaiting heart transplantation. N Engl J Med 2007; 357:885–896. 31 INTERMACS – Interagency Registry for Mechanically Assisted Circulatory Support Manual of Operations Adverse Event Definitions. 2007; version 2.2. http://www.uab.edu/ctsresearch/intermacs/Appendices_092107.htm. [Accessed 20 October 2010] 32 Uriel N, Pak SW, Jorde UP, et al. Acquired von Willebrand syndrome after continuous-flow mechanical device support contributes to a high prevalence of bleeding during long-term support and at the time of transplantation. J Am Coll Cardiol 2010; 56:1207–1213. Key paper discussing the deficiency of vWF multimers in LVAD-supported patients and risks of bleeding. 33 Heilmann C, Geisen U, Beyersdorf F, et al. Acquired von Willebrand syndrome in patients with ventricular assist device or total artificial heart. Thromb Haemost 2010; 103:962–967. Another key paper discussing the deficiency of vWF multimers in LVAD-supported patients and risks of bleeding. 34 Geisen U, Heilmann C, Beyersdorf F, et al. Nonsurgical bleeding in patients with ventricular assist devices could be explained by acquired von Willebrand disease. Eur J Cardiothorac Surg 2008; 33:679–684. 35 Hampton CR, Verrier ED. Systemic consequences of ventricular assist devices: alterations of coagulation, immune function, inflammation, and the neuroendocrine system. Artif Organs 2002; 26:902–908. 36 Stern DR, Kazam J, Edwards P, et al. Increased incidence of gastrointestinal bleeding following implantation of the HeartMate II LVAD. J Card Surg 2010; 25:352–356. Cohort study examining bleeding risk in LVAD-supported patients. 37 Miller LW. The development of the von Willebrand Syndrome with the use of continuous flow left ventricular assist devices: a cause-and-effect relationship. J Am Coll Cardiol 2010; 56:1214–1215.