Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
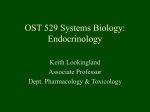
case study [chemistry | immunology] Principal Laboratory Findings The Case of the Newborn with Ambiguous Genitalia Test Qing H. Meng, MD, PhD, Stephen Hill, PhD, FCACB, Gillian Luxton, MD, FCACB Department of Pathology and Molecular Medicine, McMaster University, Ontario, Canada Hematology WBC count RBC count Hemoglobin Hematocrit MCV Differential: DOI: 10.1309/FU9PBRKA5AHFV191 Patient 1-day-old baby. Chief Complaint Neonate was noted to have ambiguous genitalia. Family History The father is healthy. The mother (para 1, gravida 2) had a Cesarean section for her first baby girl 3 years ago at 40 weeks gestation due to failure to progress following three days of labor. The girl has been fine. The mother had no history of diabetes or hypertension. Drug History The mother did not take any medication during her most recent pregnancy. She had no history of drug abuse or contact with any toxic chemicals. Physical Examination The baby weighed 3,925 grams with APGAR scores of 9 at both 1 minute and 5 minutes after birth. Ambiguous genitalia (clitoromegaly and partial fusion of the labioscrotal folds) were observed. Cardiovascular and respiratory systems were normal. Principal Laboratory Findings [T1] 532 Questions: 1. What is(are) this patient’s most striking laboratory result(s)? 2. How do you explain this patient’s most striking laboratory test results? 3. What is the most likely diagnosis relevant to this patient? 4. Which additional laboratory test(s) are appropriate to order on this patient and why? 5. What is the etiology of this patient’s condition? 6. How is this patient’s condition typically diagnosed? 7. How should this patient be treated? Chemistry Glucose BUN Sodium Potassium Chloride Bicarbonate Anion gap TSH Free T4 Cortisol (0800 h) 17-OH-progesterone DHEA-S “Normal” Reference Range 14.8 4.16 11.1 39.9 78.3 9.0 4.1 1.3 5.5-15.5 x 103/µL 3.25-5.50 x 106/µL 10.5-14.0 g/dL 40-60% 70-95 fL 1.5-7.0 x 103/µL 2.0-8.0 x 103/µL 0.0-1.1 x 103/µL 79 5 130 5.8 100 18 12 1.8 2.6 1.0 34,500 822 50-80 mg/dL 4-12 mg/dL 135-145 mEq/L 3.5-5.5 mEq/L 95-105 mEq/L 22-30 mEq/L 5-14 mEq/L 0.5-5.5 µU/mL 0.8-2.7 ng/dL 5-23 mg/dL 20-140 ng/dL 26-444 µg/dL WBC, white blood cell; RBC, red blood cell; MCV, mean corpuscular volume; BUN, blood urea nitrogen; TSH, thyroid stimulating hormone; T4, thyroxine; DHEA-S, dehydroepiandrosterone-sulfate Possible Answers: 1. The most striking laboratory results are markedly elevated 17-OH-progesterone, and dehydroepiandrosterone-sulfate (DHEA-S) concentrations; elevated potassium; reduced sodium, cortisol, and urea levels; low osmolality; and a normal anion gap. 2. The reduced cortisol level and accumulation of its precursor, 17-OH-progesterone, suggest 21-hydroxylase deficiency, which is the most commonly seen enzyme deficiency in newborns with congenital adrenal hyperplasia (CAH). The accumulation of 17-OH progesterone may lead to the increased formation of dehydroepiandrosterone (DHEA) and its metabolite, DHEA-S, by an alternate pathway. The increased DHEA and DHEA-S concentrations lead to the peripheral synthesis in the liver of androstenedione and testosterone, which, together, are responsible for ambiguous genitalia, hirsutism, and virilization in females. Lack of the 21-hydroxylase enzyme blocks the pathways for both cortisol and aldosterone production, the principal glucocorticoids and mineralocorticoids produced by the adrenal cortex. Aldosterone causes increased sodium ion reabsorption and potassium and hydrogen ion excretion (Na+ ↔ K+ and Na+ ↔ H+ exchange) by the distal convoluted tubules and collecting duct of the kidney. Aldosterone is essential for the homeostasis of plasma water, sodium, and potassium ion concentrations. Aldosterone deficiency leads to hypovolemia, hyponatremia, hyperkalemia, and metabolic acidosis. In early or mild aldosterone and cortisol deficiency, these biochemical changes may not be evident. Severe cortisol deficiency may cause hypoglycemia. laboratorymedicine> july 2003> number 7> volume 34 © Downloaded from http://labmed.oxfordjournals.org/ by guest on October 18, 2016 Medical History Neonate delivered by Cesarean section under spinal anesthesia at 39 weeks of gestation. After delivery, the baby was assigned as a male by the obstetrician. neutrophils lymphocytes monocytes T1 Patient’s Result 4. Serum aldosterone, plasma renin activity, serum testosterone, plasma ACTH, and urinary pregnanetriol levels. Low serum aldosterone concentration is expected in patients with CAH, while plasma renin may be increased or decreased depending on the type of enzyme deficiency present and the degree of mineralocorticoid deficiency. In addition, serum testosterone concentration is increased due to the decreased cortisol and aldosterone levels in such patients and shunting of cortisol precursors toward adrenal androgen production. Moreover, cortisol deficiency leads to an elevated ACTH concentration, which increases further the levels of cortisol and aldosterone precursor substances and results in bilateral adrenal hyperplasia (BAH). Measurement of urinary pregnanetriol (a metabolite of 17-OH-progesterone) concentration is also useful in the diagnosis of CAH. Genetic testing for mutations in the gene for the 21-hydroxylase enzyme is rarely necessary for the diagnosis of classical forms of adrenal hyperplasia, but is essential in the prenatal diagnosis of adrenal hyperpla- © sia. Subtle forms of adrenal hyperplasia associated with nonclassical forms of 21-hydroxylase deficiency and 3-beta-hydroxysteroid dehydrogenase deficiency often require a Cortrosyn (synthetic ACTH) stimulation test to demonstrate the abnormal accumulation of precursor steroids. 5. Several enzyme deficiencies can cause CAH [F1] and principal among these are: 21-hyroxylase, 11-beta-hydroxylase, 3-beta-hydroxysteroid dehydrogenase, 17-alpha-hydroxylase, 17,20-cholesterol-desmolase, and corticosterone 18-methyloxidase type II. Deficiency of the 21-hydroxylase enzyme accounts for more than 90% of CAH cases.1 In this type of CAH, there is increased production of progesterone, 17-OHprogesterone, DHEA, and androstenedione. Moreover, urinary concentrations of the metabolites of these substances (eg, 17-ketosteroids and pregnanetriol) are increased, while serum cortisol levels are decreased. The clinical symptoms of CAH are exacerbated by the stress (and demand for cortisol) of increased physical activity. The gene (CYP21) for the 21hydroxylase enzyme is located on chromosome 6p21, adjacent to the human leukocyte antigen (HLA) genes. This gene is about 30 kilobases (kb) away from a pseudogene (CYP21P), which is 98% homologous in structure with the CYP21 gene; therefore, the minor differences between these genes are sufficient to render the pseudogene inactive in the production of functional 21-hydoxylase enzyme. Deficiency of the 11-beta-hydroxylase enzyme causes 3% to 5% of all cases of CAH and is associated with a characteristic elevation of serum 11-deoxycortisol and deoxycorticosterone concentrations. In addition, urinary levels of 17-OH-corticosteroids are also usually high. Because of the mineralocorticoid activity of deoxycorticosterone, patients with 11-beta-hydroxylase enzyme deficiency exhibit salt retention, decreased plasma renin activity, and hypertension with hypokalemic alkalosis. The 11-beta-hydroxylase gene (CYP11B1) resides on chromosome 8q21. A neighboring gene (CYP11B2) codes for aldosterone synthetase, which catalyzes the conversion of corticosterone to aldosterone in the zona glomerulosa of the adrenal cortex. Mutations and deletions in the CYP11B2 gene result in diminished aldosterone synthesis. Therefore individuals with a mutated CYP11B2 gene develop hyponatremia, hyperkalemia, and dehydration. Deficiency of the 3-beta-hydroxysteroid dehydrogenase enzyme is indicated by an abnormal ratio of 17-hydroxypregnenolone to 17-hydroxyprogesterone and dehydroepiandrosterone to androstenedione concentration. The gene for 3-beta-hydroxysteroid dehydrogenase resides on chromosome 1p13. Deficiency of the 17-alpha-hydroxylase, 17,20-lyase, and 17,20-cholesterol-desmolase enzymes result in virilization of affected female infants and undervirilization of affected male infants. A single gene (CYP17) mutation causes the deficiency in the activity of these enzymes. Moreover, steroidogenic acute regulatory protein (StAR) appears to be involved in the transport of cholesterol across the mitochondrial membrane where it can be acted upon by the CYP450 system in laboratorymedicine> july 2003> number 7> volume 34 Downloaded from http://labmed.oxfordjournals.org/ by guest on October 18, 2016 3. Most likely diagnosis: Congenital adrenal hyperplasia. Congenital adrenal hyperplasia is an inherited autosomal recessive disorder that occurs with a population frequency of 1:1,000. It is classified in 2 forms based on different clinical presentations: classical and non-classical. The non-classical form of CAH due to partial 21-hydroxylase deficiency is the most common of all autosomal recessive diseases. The classical form of CAH due to hydroxylase deficiency occurs as a result of the imbalance in the production of cortisol, aldosterone, and androgens.1 Too little cortisol during physical stress can lead to low blood pressure and even death. The lack of aldosterone production results in salt wasting. Excess androgen production causes abnormal physical development. The non-classical form of CAH is a milder version of the classical form of this disease. Patients with nonclassical CAH are not deficient in cortisol and aldosterone; however, they do produce excess androgens. Salt wasting forms of adrenal hyperplasia are accompanied by low serum aldosterone concentrations, hyponatremia, hyperkalemia, elevated plasma renin activity, hypovolemia, and hypotension. In contrast, hypertensive forms of adrenal hyperplasia (eg, 11-beta-hydroxylase deficiency and 17-alpha-hydroxylase deficiency) are associated with suppressed plasma renin activity and often hypokalemia. The diagnosis of CAH depends upon the demonstration of inadequate production of cortisol and/or aldosterone in the presence of accumulation of excess concentrations of precursor hormones. For example, the distinguishing characteristic of 21-hydroxylase deficiency is a very high (usually exceeding 1,000 ng/dL) serum 17-OH-progesterone and urinary pregnanetriol (a metabolite of 17-OHprogesterone) concentrations in the presence of clinical features suggestive of the disease (eg, a female with ambiguous genitalia, evidence of salt wasting, clitoromegaly, precocious pubic hair development, excessive growth, premature phallic enlargement in the absence of testicular enlargement, hirsutism, oligomenorrhea, and/or female infertility). 533 Cholesterol ACTH 17 OH'ase 17,20 Lyase 17,20 DLase Pregnenolone 17-OH Pregnenolone DHEA Progesterone 17-OH Progesterone Androstenedione 3 βSDH 21 OH'ase Deoxycorticosterone 11-deoxycortisol Testosterone 11 OH'ase Cortricosterone Cortisol Estradiol 18 OH'ase Aldosterone the synthesis of pregnenolone which then is converted in various steroidogenic tissues into cortisol, aldosterone, or sex steroids. A deficiency of StAR results in a global steroid deficiency state. Lastly, deficiency of corticosterone 18-methyloxidase type II is characterized by aldosterone deficiency (low plasma aldosterone concentration) with chronic hyperkalemia and no abnormalities of sexual differentiation. 6. Prenatal diagnosis for 21-hydroxylase deficiency can be performed using DNA analysis on fetal cells obtained from amniotic fluid following amniocentesis or from chorionic villus samples (CVS).2 This technique will detect 95% of all abnormal genes for CAH. Neonatal screening for 21-hydroxylase deficiency is sufficiently specific and sensitive to detect almost all infants with classical CAH and some infants with non-classical CAH. Analysis of 17-OH-progesterone levels in dried blood spot samples obtained from newborns between 48 to 72 hours of age is the typical method for screening newborns for CAH. A positive screening result must be confirmed by quantitative analysis of 17-OH-progesterone concentration, using a sensitive and specific method, in a second serum/plasma sample, urine steroid analysis, or mutation analysis of the CYP21 gene. 534 7. Early (less than 9 weeks after last menstrual period) treatment of a pregnant woman carrying a CAH-affected fetus appears to be somewhat successful in preventing the virilization of a female fetus with 21-hydroxylase enzyme deficiency. However, more detailed guidelines for the use of this treatment are needed. Infants with ambiguous genitalia should be observed closely for any signs or symptoms of salt wasting while the diagnosis of CAH is being established. Such infants should undergo surgical evaluation in case corrective surgery is indicated.3 Moreover, newborns with dehydration, hyponatremia, hyperkalemia, or hypoglycemia must be treated immediately to correct these symptoms. Glucocorticoid and/or aldosterone replacement therapy may be necessary depending upon what enzyme deficiency is involved and whether cortisol and/or aldosterone synthesis is affected. A new therapy using the combination of a glucocorticoid, a mineralocorticoid, an aromatase inhibitor, and flutamide is currently under investigation.2 A clitoroplasty was done on this patient and her external genitalia progresses well. Our patient has been on corticosteroid therapy and followed regularly by pediatric endocrinologists by monitoring 17-hydroxyprogesterone, renin, and electrolytes. Keywords: congenital adrenal hyperplasia, 21-hydroxylase enzyme deficiency, cortisol, aldosterone, 17-hydroxyprogesterone 1. New MI, Carlson A, Obeid J, et al. Prenatal diagnosis for congenital adrenal hyperplasia in 532 pregnancies. J Clin Endocrinoal Metab. 2001;86:5651-5657. 2. Joint LWPES/ESPE CAH working group. Consensus statement on 21hydroxylase deficiency from The Lawson Wilkins Pediatric Endocrine Society and The European Society for Paediatric Endocrinology. J Clin Endocrinol Metab. 2002;87:4048-4053. 3. Lee PA. Genital surgery among females with congenital adrenal hyperplasia: Changes over the past five decades. J Pediatr Endocrinol Metab. 2002;15:14731477. laboratorymedicine> july 2003> number 7> volume 34 © Downloaded from http://labmed.oxfordjournals.org/ by guest on October 18, 2016 [F1] Pathway of adrenal steroid synthesis. 21 OH’ase, 21-hydroxylase; 11 OH’ase, 11β-hydroxylase; 18 OH’ase, 18-hydroxylase; 3βSDH, 3β-hydroxysteroid dehydrogenase; 17 OH’ase, 17αhydroxylase; 17,20 DLase, 17,20-cholesterol-desmolase.