Survey
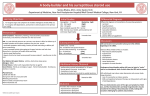
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
by William Llewellyn (Liverpool John Moores University, 2014) “If I had an hour to solve a problem, I'd spend 55 minutes thinking about the problem, and 5 minutes thinking about solutions.” ― Albert Einstein All AAS are based on TESTOSTERONE Anabolic: muscle, bone, red blood cell production Androgenic: masculinization, fertility, libido Estrogenic: anabolic, metabolic effects 1931 – testosterone synthesized 1934 – first steroid for hypogonadism (Proviron, Schering Germany) 1935, 1936 – testosterone esters, Methyltestosterone 1940’s – AAS in common medical use 1950’s – “Research Decade” Manipulate anabolic/androgenic/estrogenic effects alter bioavailability Injection Testosterone Esters Nandrolone Esters Methenolone Boldenone Trenbolone Oral Methandrostenolone Oxymetholone Oxandrolone Stanozolol Mesterolone Hypogonadism Osteoporosis Anemia Anti-Wasting Tissue Healing/Injuries and Burns Breast Cancer Cardiovascular Cholesterol (reduced HDL/LDL ratio) Ventricular hypertrophy Blood pressure Increased prothrombin time Reproductive Infertility Sexual dysfunction Hypogonadism/testicular atrophy (men) Menstrual irregularities (women) Liver Toxicity (Orals) Liver dysfunction Liver cancer Cosmetic Acne Hair loss (androgenetic alopecia) Gynecomastia Water or fat retention Psychological Depression Aggression Virilization (women) Body/facial hair growth Clitoral enlargement Vocal change Not Supported Suicide “Roid Rage” other cancers Ability to build muscle becomes widely known AAS use spreads throughout sports/bodybuilding Hospitals flooded with toxicity cases Major sporting events Competitors dying on the field Turning point for AAS prohibition Doping scandals Media speculation Public “Fix steroid problem!!!” Drug Enforcement Agency (DEA) Department of Health and Human Services American Medical Association (AMA) Various Experts All opposed U.S. steroid criminalization “The other potential loss of credibility is we are telling people that they are going to be dropping over dead and the athletes are looking at the longtime user and not seeing people dropping like flies. Now, increased death, probability of death, or morbidity could be taking place, but people are apparently not dropping like flies.” - Dr. Charles Yesalis AAS are Acutely Very Safe Drugs No overdose No physical addiction Non-toxic, primarily Exceedingly rare to have a life-threatening reaction Most short-term side effects are cosmetic or temporary Health Risk Primary With Long-Term Abuse Increased risk of CVD/heart attack/stroke Hypogonadism 24 AAS related deaths in 16 years (1996-2012) Department of Forensic Medicine (DOFM) All men, mean age early 30’s Accidental drug toxicity 54.2% (13) Combined accidental drug toxicity/CVD 8.3% (2) Suicide 16.7% (4) Homicide 12.5% (3) Accident 4.2% (1) Undetermined 4.2% (1) J Forensic Sci, 2014. doi: 10.1111/1556-4029.12424 In only ONE CASE was AAS found alone Opioids 37.5% Psychostimulants 66.7% Benzodiazepines 45.8% (9) (16) (11) Steroid Deaths = OTHER DRUGS Cardiac pathology was diagnosed in 47.8% of Cases More than 20 years, fighting AAS abuse with prohibition policies Prevent diversion of pharmaceuticals Prohibit physicians from prescribing (non-medical) Ban the importation of AAS Criminalize use/possession . 1. Drastically Cut Supply of Pharmaceuticals Portion of Market 10% . Legitimate Illegitimate 90% Raw material trade, mainly from China. UK major hub. Converting powder into product Converting powder into product 12 AAS Samples from 3 Internet Dealers None matched the label. Underdosed, overdosed, substitute ingredients. Contaminants included: Arsenic Tin Lead Prednisone (corticosteroid) Betamethasone (corticosteroid) Diethylstilbestrol (synthetic estrogen) Benzyl chloride (alkylating agent, precursor chemical) FurFural (industral processing) 24 samples sent in for analysis 6 samples (25%) contained bacteria. Other contaminants included: BHT (food preservative) Bis (2-ethyl hexyl) phthalate (plasticizer) Paraffin (kerosene) Amines & Carboline (organic/synthesis) Fatty Acids Underground ANABOLICS, 2010 35 year old bodybuilder carrying assortment of supplements, steroids, other drugs, two unlabeled vials admitted to the hospital. Symptoms of liver dysfunction. Progressed to signs of heavy metals poisoning. 33x safe level of arsenic present. Patient died. Analysis of vials yielded an unlabeled bottle with very high arsenic level, no AAS. J Clin Endocrinol Metab. 2013 Dec;98(12):4613-8 2. Prohibition prevents prescribing (nonmedical) No physician oversight or advice Minimal focus on health markers/blood testing . Higher Doses Longer Cycles (bridging, cruising) Spot Injections More Injections 3. Prohibition = Market Free-For-All Much higher concentrations Unapproved AAS Blends/multi-component AAS (“pre-stacked”) 4. Effect of Prohibition Unknown 2014 meta-analysis puts usage rate at: 3.3 % global lifetime prevalence rate 6.4 % for men 1.5 % for women . Prohibition has decimated AAS supply Placed users at high risk of drug mislabeling, contamination, infection Diminished access to medical advice/blood work Unknown effect on AAS prevalence, though usage rates are higher today than pre-prohibition Is this a recipe for reduced public harm? “No problem can be solved from the same level of consciousness that created it.” ― Albert Einstein 1. Quantify Risk of AAS Misuse Researchers and clinicians need to work together to collect and analyze data Short-term risks Long-term risks Athletes vs. Bodybuilders 2. Quantify Black Market Risk Heavy metals Bacterial/microbial contamination Dosage/drug mislabeling Other substance contamination 3. Evaluate New Equipment Syringe filters Sterile vials Can remove all bacteria from a solution Limitations: Cannot remove other drugs, pyrogens, or heavy metals. 4. Address Abuse vs. Self Medication Many men 35+ suffer from hypogonadism (low testosterone) Clinical symptoms: loss of libido, reduced energy, loss of muscle mass, increased adiposity, osteoporosis, and depression. HRT shows consistent improvements in CVD, diabetes, metabolic syndrome, and cancer risk. Some needle exchange users should be referred for medical treatment. 5. Allocation of Resources AAS users should not take away resources from narcotic interventions AAS = separate issue = new resources 6. Staffing: Weightlifter/Former AAS User Beyond standard BBV interventions Connect with users; better acceptance of drug-related advice 7. Rethink Policies Ease restriction on imports Recovery agenda? Allow personal-use. Never criminalize. Allow physicians to Rx and monitor Liposuction deaths: 1 every 5,000 procedures