Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
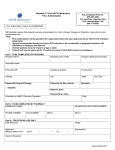
PacifiCare Non Formulary Medication Prior Authorization Form DATE: _______ TIME: _______ MOD: III Patients Name: ________________________________ Physician Name: _______________________________ Specialty: _______________________________ Address: _______________________________ _______________________________ Phone #: (______)________________________ Member #: ________________________________ Phone #: (______)_________________________ Date of Birth: ________________________________ Male Female FAX #: (______)________________________ Strength: Requested Medication: Directions For Use: DIAGNOSIS: Date Patient Started this Medication: NAME OF SPECIFIC DRUGS TRIED AND FAILED: Reason For Non-Formulary Request. ( Patient chart notes will be requested if further documentation is necessary ) Date: Requesting Physician Signature: Office Use Only Approved Denied Date Received : Date Received : Date Reviewed: Date Reviewed: Approval Dates: to Reason Denied: Signature: PC #: 1 2 3 4 5 Physician notified _______:_______ am/pm Carrier/Acct: _______________________________ Employer Group: ___________________________ 1) To Prescriber- Complete and return to: Signature: Office Use Only Plan Code: ____________________________ Facility ID: ____________________________ Prescription Solutions 3515 Harbor Blvd. Costa Mesa, CA 92626 Phone # : 1-800-711-4555 Fax # : 1-800-527-0531 2) Obtain Member’s Pharmacy Name and Phone number. 3) Instruct member to call prescriber in three (3) working days of request to check approval. If this request is for an acute medication, please call 1-800-711-4555. 4) Prescription Solutions will contact prescriber with decision or request for additional information. 5) Once approval is received, prescriber calls in prescription to member’s pharmacy 6) Authorization will be granted for up to twelve (12) months unless otherwise noted. Request for Missing/Additional Information Form Request for Missing/Additional Information Your request for Prior Authorization for the patient listed above is incomplete and cannot be processed as a Prior Authorization request until additional information has been provided. In order to ensure rapid patient care and to expedite appropriate medication consistent with the member’s benefit, we need the following pertinent information. Patient name Directions for Use Member # Diagnosis Date Birth Name of specific drugs tried and failed Requested Medication Reason for non-formulary request Requesting physician signature/contact name Additional drug specific information. Complete questions on the following page related to the item number indicated below. 1 2 3 4 5 6 As part of your contract with PacifiCare, it is important to provide complete clinical information when requesting prior authorization for non-formulary drugs. Please record the requested information in the space provided on the top half of this form, and/or the drug specific information on the next page and then fax back the request to: 800-527-0531. Or, to expedite the resolution of the requested medication, call 800-711-4555. Note: If complete information is not returned within 48 hours, a denial will be issued. Once complete information is received, a decision will be rendered. Request for Drug Specific Information 1OSTEOPOROSIS 1. DRUGS: Evista Fosamax Miacalcin 2. 3. Member Name: Member ID #: Bone Mineral Density/Scan (DEXA or QCT) Date:______ Result: Standard deviation below young adult mean: ____________ Is patient currently on ERT? Yes____ No____ gm/cc Does patient have a contraindication for ERT? Yes____ No____ If yes, What is the cause ? ________________________________ _________________________ 4. Does patient have a history of vertebral compression fractures? Yes____ No____ 2 DRUGS: Aricept Cognex 5. Does patient have a history of hip or distal radius fractures resulting from minimal trauma? Yes___ No___ 6. Is the patient receiving concurrent chronic or expected oral steroid use? Yes No If yes, What dose and for how long? _________________________________________________ ALZHEIMERS 1. Current Mini-Mental Status Exam (MMSE) Score:_______ Date: 2. If score is 10 or 11, in which of the following categories does the patient exhibit independence? Transferring Continence Feeding Bathing Dressing Going to toilet 3 HYPERLIPIDEMIA 1. DRUGS: Lescol Lipitor Mevacor Pravachol Zocor 2. Lipid Panel information: Baseline date:_________________ Current date: TC TC TG TG LDL LDL HDL HDL Goal of therapy i.e. LDL < 100 ________________ Current drug and dose Does patient have any of the following CHD or CAD risk factors? HDL Cholesterol < 35 Diabetes Hypertension Smoking Female w/ premature menopause and not on ERT 4 PPI’S DRUGS: Aciphex Prevacid Prilosec Female > 55 years old Male > 45 years old 1. Is this initial therapy? Yes____ No____. If no, how long has the patient been on the drug? ______________ 2. For continuation of therapy, What are the clinical reasons? 3. Has step down therapy been tried? Yes____ No ____ If no, list reasons why 4. Has PPI been prescribed by GI consult for long term therapy? Yes____ No ____ 5. Patient has diagnosis of Zollinger-Ellison Syndrome Esophagitis Stomach Cancer Grades III / IV Esophagitis Esophageal Stricture Gastropathy Other malignancies Barrett’s NSAID