Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
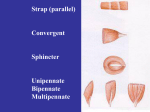
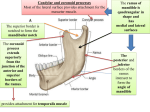
Edward Via Virginia College of Osteopathic Medicine Block 7 - 2013 Stuart F. Williams D.O. Additional Slides from David G Harden DO,FAAFP 1. 2. 3. 4. Define TMJ (Temporomandibular Dysfunction) Describe the role of the temporal bone in TMJ Define approaches to treatment of TMJ in Osteopathy in the Cranial field Define Counterstrain Points associated with TMJ MUSCLES Lateral Pterygoid Muscle Medial Pterygoid Muscle Tony, an otherwise healthy 22-year old male presents with left sided ear pain of 4 weeks’ duration after biting into an apple & feeling his jaw ‘pop’ Seen at the ER that night, as his jaw hurt immediately Told he had ‘TGM’ or something & was treated symptomatically • • • • • PMHx – none PSHx – none All – penicillin Meds – none Social – single, no children, lives in graduate dorm, binge ETOH & tobacco use; won’t admit nor deny marijuana use, but denies anything “heavier” Depression (opening of the mouth from rest) Elevation (closing of the mouth to rest) Protrusion (carrying the mandible forwards from rest) head anteriorly, disc posteriorly Retraction (carrying the mandible back to rest) Head and articular disc move anteriorly Head posteriorly, disc anteriorly Small amount of lateral movement (side-to-side movement from the rest position) bc of pterygoids • Smooth, normal motion is a blending: – – – – Muscular contraction on mandible Ligamentous tension Contraction, or lack thereof, by lateral pterygoid Gravitational and structural forces acting on cranium and mandible TMJ is a synovial joint, formed by the mandibular condyle in the fossa in the temporal bone Different from other synovial joints in that it: Formed from membrane (vs. endochrondron and therefore has no hyaline cartilage) Lined by fibrous tissue Joint cavity is divided into 2 by an intra-articular disc • • • This division by the disc means that there are actually two joints on each side: – One between the ramus of the mandible and the articular disc – Another between the disc and the temporal bone fossa During low-load opening activities (talking, gentle chewing) the motion is confined to the first During high opening activities (Eating/Yawning )the motion involves the second joint – this is usually when / where dysfunction occurs The stylomandibular ligament – purpose of the ligament is unknown Stylohyoid ligament provides attachment to the superior fibers of the middle pharyngeal constrictor and is closely related to the oral pharynx Lateral ligament helps strengthen the capsule Upper Head originates on the Greater Wing of the Sphenoid Lower Head of lateral pterygoid originates on the Lateral pterygoid plate Upper head attaches to disc Lower head attaches to mandible Together, they coordinate opening & closing of the mandible with the articular disc Also helps with protrusion and lateral deviation Temporalis – anterior fibers elevate, posterior retract Medial Pterygoid – elevates the mandible & helps with lateral & protrusive movements Digastric – depresses the mandible Mylohyoid – depresses mandible when hyoid fixed • • Masseter – elevates the mandible 3 points of attachment: – Superficial part from zygomatic process of the maxilla & from the anterior 2/3 of lower border of the zygomatic arch – Middle part from the deep surface of the anterior 2/3 of the zygomatic arch & from the lower border of the posterior one-third of the arch – Deep part arises from the deep surface of the zygomatic arch Really, really involved…more than we’ll go into depth here without more anatomy Note approximation of arterial and nervous supply in area of TMJ Pain & clicking with mandibular motion Tenderness to palpation over TM joint Lateral pterygoid draws disc and mandible anteriorly with opening when tight, prevents posterior motion of both Anteriorly displaced mandible – ↓ closing Posteriorly displaced mandible – ↓opening • Smooth, normal motion is a blending: Muscular contraction on mandible – Ligamentous tension – Contraction, or lack thereof, by lateral pterygoid – Gravitational and structural forces acting on cranium and mandible – Jaw Opening - 40-50 mm Side to Side (lateral motion) - 8 mm Gravity alone can cause 15mm of depression Due to pterygoids Protrusion - 6-8mm Retrusion- 3mm Hot bilateral masseter & medial pterygoid TPs with severe hypertonicity. 20% population 3:1 (female : male) Etiologies: Malocclusion (tooth loss, improper alignment of dentures) Trauma Psychological / Emotional Neuromuscular “Poor Health” Internal Derangement Pillow too high Children: mm spasm after recent orthodontia Bruxism – grinding their teeth Dental malocclusion Jaw clenching Excessive gum chewing Trauma Lyme Disease JRA (other Connective Tissue Disease) Juvenile Rheumatoid arthritis If > 3-4 days duration Unilateral Otoscopy & pneumo-otoscopy wnl Up to 48% can have TMJ dysfunction! TMJ tenderness on palpation Restricted MOTION of jaw Unilateral “clicking” Aggravated by chewing or biting Ear Pain Etiologies (Preauricular referred pain secondary to TMJ) Nerve irritation Muscle spasm DJD (older pt) Other: jaw, ear, facial pain, H.A., masicatory muscle pain, fatigue, “tightness.” Traumatic Whiplash Bruxism (clenching or grinding teeth) http://peninsulaclarion.com/images/111801/knockout.jpg Cervical dysfunction Scoliosis Short leg http://www.whiplashandtmj.com/logo.jpg Cranial dysfunction http://www3.telus.net/hotdigitaldog/plumb%20bob.jpg • Total body structural exam – – • Postural imbalance perpetuates problem Higher incidence in dysautonomia Evaluation of the cranial mechanism vital – Myofascial trigger points & muscle imbalance • Masseter, pterygoids, temporalis, digastric – Skeletal arthrodial dysfunction • Sphenobasilar compression • Temporal bone restrictions – Ligamentous dysfunction • Sphenomandibular ligaments • Stylomandibular ligaments Anteriorly displaced mandible – can’t close well. Posteriorly displaced mandible – can’t open well. Monitor pt’s TMJ with flats of fingers over TMJ just anterior to the tragus while patient opens & closes jaw. Observe the mental area of the mandible for deviation while you simultaneously palpate the TMJs. Similar in concept to open/closed facets… Anteriorly displaced mandible – can’t close well. Posteriorly displaced mandible – can’t open well. Monitor pt’s TMJ with flats of fingers over TMJ just anterior to the tragus while patient opens & closes jaw. Observe the mental area of the mandible for deviation while you simultaneously palpate the TMJs. Similar in concept to open/closed facets… Anteriorly displaced mandible – can’t close well. (more common) Posteriorly displaced mandible – can’t open well. Common TMJ problem: anterior gliding motion of mandible is restricted Ex: L TMJ restriction R side works normally causes deviation of chin to L(restricted side) Multifaceted and multidisciplinary Proper DX may require Imaging Manual Treatment-OMT Medications Anti-inflammatory and antispasmodic Dental appliance or orthodontia Psychosocial Manipulative Treatment in TMJ Disorders Somatic dysfunction: Skeletal – Arthrodial - Myofascial Can be either direct or indirect Clues as to which to use: Acute Chronic Cause of injury/problem Pt tolerance Left TMJ Dysfunction Jaw Deviation to L Muscle Energy Restricted Jaw/Mouth Opening “Close mouth.” Two fingers under chin. “Open mouth against my fingers.” Hold 3-5 seconds. Repeat 3-5 times. Reevaluate motion of mandible to see if technique effective. 50 YOF c/o debilitating headaches(h.a.), neck pain, and R arm and hand pain. HA prompted spinal taps and a dx of aseptic meningitis. HA are described as “everywhere,” and “nasty” all the time. Recent cervical MRI revealed mild to moderate central stenosis & moderate L foraminal stenosis from a herniated disc at C5-6. Patient has seen multiple times by several other physicians with minimal relief. She says, “Dr. _____, you are my last hope.” PMH: SLE with significant arthritis & synovitis. General: Anxious appearing female c/o h.a. of “13” on a 10 scale. Neuro: Alert & Oriented X 3. CN 2-12 grossly intact. Funduscopic benign DTRs +2 in UE & LE except +1 brachioradialis HENT: Normocephalic, TMs clear & mobile, Pharyx with minimal ant pillar injection, no exudate. No enlarged ant or post nodes. Multiple TPs found in the trapezius (rarely palpated) Other TPs found: Levator scapulae (h.a.) Right teres minor (shoulder pain) Right subscapularis (shoulder pain) Bilateral supraspinatus (shoulder pain) LAC 5 (neck pain) RPC3 (neck) LPC1 (neck) Multiple TPs were tx & relieved! On d/c, pt stated pain was 0/10! No h.a.! Will f/u patient for reassessment of cervical pain secondary to DJD & SLE. Patient referred from dentist with “closed and locked” jaw. Unable to open mouth > 10mm (normal is 40mm). No deviation of mandible noted. Severe local muscle pain at end range esp in masseter region. C/O pain in R TMJ, ear, and supraorbital. Began 2 days after a dental procedure where she had to hold her mouth open for an extended period of time. Neuro: Oriented X 3 CN 2-12 grossly intact DTRs + 2 Eyes: PERRLA, Funduscopic benign HENT: TMs clear & mobile. Pharynx noninjected. Neck supple withour adenopathy Upper cervical, sphenobasilar & occipitomastoid areas unremarkable. Hot bilateral masseter & medial pterygoid TPs with severe hypertonicity. Counterstrain to bilateral TPs. On reevaluation, both bellies of masseter and medial pterygoid were soft and much less tender. Patient could open mouth to 40mm without difficulty. Placed on soft diet for 3 days. F/U: Patient continued to improve and was able to open mouth without difficulty. TP Location Tx Masseter Superficial and deep fibers of the masseter muscle. Press posterior toward anterior border of ascending ramus of mandible. Push slightly open jaw towards the TP from opposite side Medial pterygoid Posterior surface of ascending ramus of mandible approximately 2 cm above the angle of the mandible (press anteriorly). Pull with fingers of opposite hand slightly open jaw laterally away from the TP, deviating mandible to the opposite side. Lateral pterygoid 1 cm anterior to neck of the condyle (press medial and sl posterior). Lower edge of greater wing of sphenoid (press medial). With open jaw, use fingers of opposite hand to pull jaw laterally away from TP, deviating mandible to the opposite side. Temporalis anywhere in the fan-shaped fibers of the muscle (press medially With opposite hand push relaxed jaw toward the TP. • • • • • Stand opposite the TMJ to be treated Gloved caudad thumb is placed inside patient’s mouth on surface of last molar tooth Cephalad thumb & index fingers stabilize greater wings of the sphenoid Slight pressure on gloved thumb moving mandible in a caudal direction Balance and hold until release is felt Stabilize temporal bone while the gloved hand applies gentle caudal & anterior traction on the mandible Hold until a release is felt Stabilize temporal bone with a five-fingered hold Middle finger in external auditory meatus Index finger & thumb grasp zygomatic arch Ring and little fingers on the mastoid process Ext Rotation with Flexion Thumb down & out Ring up & in Int Rotation with Extension Index up & in 5th down & out Short Leg Syndrome: Can be a factor in TMJ dysfunction. Tony’s jaw still hurts, but he can now close it more easily and with less pain. You also notice less deviation. You instruct him to apply heat for 15-20 mins, 3x/day (you expect him to do this once daily, maybe), and continue prn pain meds He’ll follow up in 2 weeks & avoid any further bar bets…oh yeah, and he says you’re “Pretty cool – for a doc.”