Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
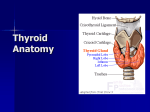
ISSN :2250-0359 Volume 5 Issue 3.5 2015 Anatomy of thyroid gland Surgeon’s perspective Balasubramanian Thiagarajan Stanley Medical College Abstract: Thyroid surgery can give rise to complications if performed without adequate knowledge of anatomy. With adequate knowledge of its anatomy, its variations and optimal operative technique complications can be reduced. Structures that should be protected at all costs include the recurrent laryngeal nerves, external branches of superior laryngeal nerves and parathyroid glands. Safe surgery involves meticulous hemostasis, and performing the dissection in a meticulous and step wise pattern. Thyroid gland if pulled medially will help in lateral dissection, securing middle thyroid vein (which may cause troublesome bleed in some patients as it is a branch from internal jugular vein). This also protects the recurrent laryngeal nerve from damage. Capsular dissection helps in protecting the recurrent laryngeal nerve and also protects the blood supply of parathyroid glands. An Initiative of drtbalu’s Otolaryngology online Introduction: Thyroid gland was first described by Vesalius in 1543. He called it “Glandulare laryngis” since he erroneously assumed that this gland lubricated the larynx. The word thyroid originated from the Greek word “Thyreos” meaning shield. This word was first coined by Thomas Wharton in 1656. History of thyroid surgeries make a good reading. Thyroid surgeries have been described in the 1st century AD. Celsus the Roman encyclopedia of Medicine described the operation as a dangerous procedure. Albucasis 11th century (surgeon from Corodoba Spain) explained extirpation of the thyroid gland using setons (threads) passing through the mass causing it to necrose. During the 18th century thyroid surgeries were performed only for life threatening conditions. Mortality rate those days was more than 20% which added to its disrepute. In 1850 the French Academy of Medicine totally banned thyroid surgeries because of its high degree of mortality 1. The first documented partial thyroidectomy was performed by Pierre Joseph Dasault in 1791. He used vertical midline neck incision to remove one lobe of thyroid gland. He ligated superior and inferior thyroid arteries and dislodged the gland from trachea according to his description. Thyroid surgery became safer due to the advent of Ether anesthesia in 1846, introduction of antisepsis in 1867, and development of better artery clamps 1870 which enabled unhurried dissection of the gland thereby increasing the safety of the procedure. Burned seaweed ash was used to treat goiter because of its iodine content in 1811. Modern thyroid surgery was pioneered by Theodar Kocher who is considered to be a father of thyroid surgery. He reported a series of 146 thyroidectomies spanning between 1850 – 1877 with a mortality rate of 21%. He had impressive statistics. By the year 1912 he had performed more than 2000 thyroid surgeries 2. He was awarded the Nobel Prize for his contributions towards the understanding of physiology of thyroid gland. Towards the beginning of 20th century Thomas Dunhill Peel described near total thyroidectomy as a treatment for thyrotoxicosis. He documented about 200 thyroidectomies performed by him as a treatment for exophthalmic goiter. He even claimed a mortality rate of less than 3% which was not believed by surgeons those days. Developments that pioneered safe thyroid surgery: Introduction of General anesthesia – by J.C. Warren in 1846 3 Discovery of antisepsis by Lister in 1867 3 Asepsis superseded antisepsis by usage of sterile instruments and dressings. . An Initiative of The drtbalu’s Otolaryngology online Buchner introduced boiling of surgical instruments, and surgeon’s hand washing and cleansing was introduced at Bergman’s clinic by Schimmelbuch. Anatomy of thyroid gland an overview: Thyroid gland is a butterfly shaped endocrine gland situated in the anterior neck. It lies deep to the platysma, sternothyroid and Sternohyoid muscles. Commonly this gland extends from the 6th cervical vertebrae to the 1st thoracic vertebrae (C6 – T 1). It has two lobes interconnected by a thin sleeve of thyroid tissue known as the isthmus. This thin sleeve of thyroid tissue overlies the 2nd, 3rd and 4th tracheal rings. Isthmus hence needs to be sectioned or retracted out of the way when performing tracheostomy, because the stoma will have to be created between the 3rd and 4th tracheal rings. Commonly the isthmus measures 2 cm in width, 2 cms in height and 2-6 mm in thickness 4. Normal thyroid gland weighs about 15-25 g in adults. Superior pole of the gland lies lateral to inferior constrictor muscle and posterior to sternothyroid muscle. The inferior pole of thyroid gland extends up to the level of 5th or 6th tracheal rings. Postero laterally the gland overlaps the carotid sheath and its contents. While attempting to remove large thyroid masses this relationship should be borne in mind, to prevent damage to structures within the carotid sheath. Image showing the lobes and isthmus of thyroid gland Beneath the deep cervical fascia, the thyroid gland is surrounded by a true inner capsule. This capsule is thin and is closely adherent to the gland. Projections rising from the capsule penetrates the thyroid gland dividing it into lobes and lobules. A pyramidal lobe may be present in about 50% of patients. It can arise from either lobe / isthmus and is directed upwards usually to the left. Levator glandulae thyroideae is a thin strip of muscle if present could be seen extending from the isthmus / lateral lobe to the hyoid bone or thyroid cartilage. This muscle could be innervated by a branch from ansa cervicalis or superior laryngeal nerve. Presence of levator glandulae thyroideae is often associated with the presence of pyramidal lobe. An Initiative of drtbalu’s Otolaryngology online Knowledge about levator glandulae thyroideae is important during neck surgeries. This structure could represent the persisting distal end of thyroglossal duct. Anterior cervical region should hence be clearly examined during total thyroidectomy in order not to leave behind residual thyroid tissue. Lobes of thyroid gland: Figure showing thyroid lobe along with pyramidal lobe Levator glandulae thyroideae is fibrous / fibromuscular band of tissue stretching from the pyramidal lobe / upper border of isthmus of thyroid gland commonly on the left side. Superiorly it gets attached to the body of hyoid bone 5. Mori after performing meticulous dissection of thyroid tissue classified levator glandulae thyroideae into 5 types according to its attachments. Hypopyramidalis Thyreopyramidalis Thyreoglandularis Hyoglandularis Tracheoglandularis Each lateral lobes of thyroid gland are medially bound by trachea and oesophagus. Trachea lies anterior to the oesophagus. Carotid sheath lies postero lateral to thyroid lobe. Sternomastoid muscle and other strap muscles (Sternohyoid, sternothyroid, and superior belly of omohyoid) lie anterolateral to the thyroid lobe. Thyroid capsule: Thyroid gland is ensheathed by true capsule. This capsule is tightly adherent to the gland, in fact penetrates the gland. Posteriorly thyroid gland is anchored by the presence of condensed middle layer of deep cervical fascia (known as Berrys ligament / ligament of gruber). This ligament connects the lobes of thyroid gland to cricoid cartilage and first two tracheal rings. Recurrent laryngeal nerve often passes through this ligament to reach the larynx. This ligament also contains the terminal branches of inferior thyroid artery. Care must be taken while dissecting in the area of Berry’s ligament in order to avoid damage to the recurrent laryngeal nerve 6. It is advisable to dissect this area under magnification to prevent damage to recurrent laryngeal nerve. An Initiative of The drtbalu’s Otolaryngology online Studies reveal that this ligament may contain residual thyroid tissue and hence needs to be removed in total thyroidectomy. Blood supply: Blood supply to thyroid gland is derived from a pair of arteries: i.e. Superior and Inferior thyroid arteries. Superior thyroid artery the first branch of external carotid artery along with superior thyroid vein supplies the upper pole of the thyroid gland. Close to the upper pole this artery lies superficial to the external laryngeal branch of superior laryngeal nerve which courses to supply the cricothyroid muscle. Rarely in 10% of cases superior thyroid artery may arise directly from common carotid artery 7. Superior thyroid artery passes deep to infrahyoid muscles, and on reaching the superior pole of thyroid gland, divides into anterior and posterior branches to supply superior portion of thyroid gland. Before these branches are given off superior thyroid artery gives off superior laryngeal artery which passes across the thyrohyoid membrane along with superior laryngeal nerve enters the larynx. It also gives off another branch i.e. cricothyroid artery near the lower border of thyroid cartilage. This artery lies on the cricothyroid membrane. Inferior thyroid artery is larger than that of superior thyroid artery. It is a branch of thyrocervical trunk, which is a branch of subclavian artery. This artery courses along the anterior scalene muscle, turning medially behind the common carotid artery descending on the posterior aspect of lateral lobes of thyroid before entering the inferior thyroid pole. In its course behind the common carotid artery this vessel exhibits a variable relationship with that of the sympathetic chain. This vessel may be absent in 5% of patients. Another inconsistent artery is arteria thyroideae ima. This vessel could replace inferior thyroid artery. This vessel could arise from: Innominate artery Subclavian artery Right common carotid artery Internal mammary artery Aortic arch This artery is more common in the right side. Since it is closely related to the anterior wall of trachea it may cause troublesome bleeding during tracheostomy. Within the capsule of thyroid gland there is a dense network of interconnecting blood vessels. These vessels form extensive capillary plexus around the follicles. Veins draining these plexuses give rise to inferior, middle and superior thyroid veins. These veins in turn join either the internal jugular or innominate vein. It is precisely these veins that cause bleeding during thyroidectomy or tracheostomy procedures. Lymphatics draining the thyroid gland usually follow the veins. Those travelling along with superior and middle thyroid veins drain into upper and middle deep cervical nodes respectively. An Initiative of drtbalu’s Otolaryngology online Lymphatics following inferior thyroid vessels drain into lower deep cervical chain of nodes, supraclavicular, pretracheal and prelaryngeal nodes. Thyroid gland is purely innervated by sympathetic nervous system from superior, middle and inferior cervical ganglia. Parathyroid glands: Parathyroid glands which secrete parathormone are typically 4 in number i.e. two superior and two inferior. 10% of patients may have supernumerary parathyroid glands. Each parathyroid gland weighs 35-40 mg measuring about 3-8 mm in all three dimensions. These glands can vary in color between yellow to reddish brown. Inferior parathyroid gland is found within 1 cm inferior, lateral or posterior to the inferior pole of thyroid gland in at least 50% of cases. Usually inferior parathyroid gland lies anterior to a plane drawn along the course of recurrent laryngeal nerve 8. Commonly inferior parathyroid glands could also be seen within the capsule of thyroid gland. Superior parathyroid gland can be found in the posterior aspect of thyroid lobe just 1 cm above the crossing of inferior thyroid artery and recurrent laryngeal nerve. Superior parathyroid gland could be commonly seen located in the posterolateral aspect of superior pole of thyroid gland at the cricothryoid cartilage junction. Vascular anatomy of parathyroid glands: Parathyroid glands are highly vascular structures. The inferior parathyroid gland is supplied by inferior thyroid artery. In 10% of patients’ inferior thyroid artery could be absent (particularly on the left side). In such cases a branch from superior thyroid artery supplies inferior parathyroid glands also. Whereas superior parathyroid glands are supplied by superior thyroid artery. The location of inferior parathyroid shows the greatest degree of variation because inferior parathyroid glands migrate with the thymus which descends from the angle of mandible to the pericardium. Damage to recurrent laryngeal / superior laryngeal nerves during thyroid surgeries leave behind a troublesome morbidity. Care should be taken to ensure that these two important structures are not damaged during surgery. Superior laryngeal nerve: This nerve originates at the inferior ganglion of vagus nerve (nodose ganglion) close to the jugular foramen. The average length of superior laryngeal nerve is about 2 cm in males and 1.5 cms in females. It courses posterior and medial to the internal carotid artery and descends antero inferiorly to reach the larynx. At the level of greater cornu of hyoid bone it divides into a large internal laryngeal and a smaller external laryngeal branch. The internal laryngeal nerve passes between thyrohyoid muscle and the thyrohyoid membrane. It pierces the thyrohyoid membrane along with superior laryngeal artery and vein to supply sensation to the interior of larynx. It supplies sensation to supraglottis and pyriform sinus. After entering into the larynx this nerve divides into three branches i.e. superior, middle and inferior. An Initiative of drtbalu’s Otolaryngology online The superior division divides into two / three branches supplying sensations to the lingual surface of epiglottis, lateral aspect of glosso epiglottic fold. The middle division innervates the aryepiglottic fold, vocal folds, vestibular folds and the posterior aspect of arytenoid. The inferior division is the largest of the branches of superior laryngeal nerve. It lies along the medial aspect of pyriform fossa. It is this nerve which is blocked when pyriform fossa block is given for endolaryngeal surgical procedures. This branch supplies the interarytenoid muscle. This nerve gives out a branch that communicates with the recurrent laryngeal nerve (Galen's loop). The external laryngeal nerve at the level of superior horn of thyroid cartilage turns medially and runs posterior and parallel to the oblique line. This nerve lies deep to the superior thyroid artery. Its relationship with the superior pole of thyroid gland is highly variable. Type III nerve: In this type the external branch of superior laryngeal nerve crosses the superior thyroid artery under cover of the superior pole of thyroid gland. Kierner classified the superior laryngeal nerve into 4 types depending on the relationship of its external branch to the superior pole of thyroid gland. The following are the steps which should be taken during thyroid surgeries to minimize damage to external laryngeal nerve: Type I nerve: In this type the external branch of superior laryngeal nerve cross the superior thyroid artery about 1cm above the superior pole of thyroid gland. Type IV nerve: In this type the external branch of superior laryngeal nerve descends dorsal to the superior thyroid artery and crosses its branches just superior to the upper pole of thyroid gland. Awareness of these anatomical variations will help the surgeon in preserving this branch during head and neck surgeries. Incidence of superior laryngeal nerve injury during thyroid surgeries run close to 40% 9. The incidence is also probably underdiagnosed and under reported. Prevention of damage to external laryngeal nerve has not be emphasized. 1. Division of sternothyroid muscle 2. Careful dissection in the cricothyroid space (space that lies medial surface of thyroid gland and cricothyroid muscle. 3. Meticulous isolation and dissection of superior thyroid vessels Type II nerve: In this type the external branch of superior laryngeal nerve crosses the superior thyroid artery within 1 cm of the superior pole of thyroid gland. An Initiative of drtbalu’s Otolaryngology online Recurrent laryngeal nerves: Conclusion: Always asymmetric. Left recurrent laryngeal nerve arises from vagus in the chest. It crosses the arch of aorta to reach the neck. It ascends posterior to the thyroid gland to reach the tracheo oesophageal groove. On the right side recurrent laryngeal nerve arises from vagus in the chest and reaches the neck by crossing anterior to right subclavian artery. It loops around the right subclavian artery to reach the tracheo oesophageal groove posterior to thyroid gland. It enters the larynx behind the cricothyroid articulation and inferior cornua of thyroid. Left recurrent laryngeal nerve is more closely related to the trachea in its lower part when compared to that of the right nerve. At the lower pole of thyroid gland right nerve is slightly more anterior than the left. During the middle part of the course recurrent laryngeal nerve is found within the tracheo oesophageal groove commonly. Intraoperatively recurrent laryngeal nerves could be seen in the Simon triangle formed by the common carotid artery laterally, oesophagus medially and inferior thyroid artery superiorly. It can also be identified with certainty where it enters the larynx just behind the inferior cornua of thyroid cartilage. In order to prevent complications and unnecessary post-operative morbidity following thyroid surgery one must have through understanding of anatomy of thyroid glands and their adnexal structures. Surgeon should learn to avoid pitfalls by following a systematic approach to identify vulnerable structures. An Initiative of drtbalu’s Otolaryngology online References: 1. Greene, W.W.: Three cases of bronchocele successfully removed. Am. J. Med. Sci. 121:80, 1871 2. Kazi R A. Theodor E. Kocher (1841-1917): Nobel Surgeon of the Last Century. J Postgrad Med 2003;49:371-2 3. VoIn Brunnl Kurze Geschichte der Chir., pp. 27I, 279, 28I 4. Hoyes AD, Kershaw DR. Anatomy and development of the thyroid gland. Ear Nose Throat J 1985;64(10):318–32. Standring S. In: Gray’s Anatomy, 39th Edition, London: Elsevier Churchill Livingstone. 2006; 561. 5. https://sites.google.com/site/ drtbalusotolaryngology/Home/ laryngology/surgical-anatomy-of-thyroid 6. Hollinshead WH. Anatomy of the endocrine glands. Surg Clin North Am 1958;39: 1115–40. 7. Randolph G. Surgery of the thyroid and parathyroid glands. Philadelphia: WB Saunders; 2003. 8. Aluffi P, Policarpo M, Chevorac C, et al. Postthyroidectomy superior laryngeal nerve injury. Eur Arch Otorhinolaryngol 2001;258:451–4. An Initiative of drtbalu’s Otolaryngology online