Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
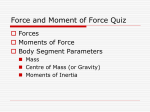
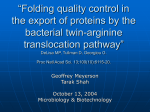
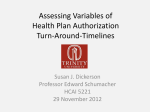
SIIM 2016 Scientific Session Posters & Demonstrations Thursday, June 30 Ι 5:30 pm – 7:30 pm Does Ready Access to Clinical Information Reduce Turn Around Time? Satre W.J. Stuelke, MD, MFA, Johns Hopkins School of Medicine; Michael Cohen; John Eng, MD; Kenneth Wang, MD, PhD (Presenter) Background Traditionally, the reason for study or clinical information given from the ordering provider for radiology examinations is not very useful for the radiologist to understand why the patient obtained a given exam. There is a wide-spread assumption that knowledge of the patient’s true clinical history, particularly from the History of Present Illness (HPI) leading to the exam order, is useful in accuracy of image interpretation and helpful in reducing turnaround time (TAT), but precious little has been published supporting these assumptions. Systems providing this information have been described in the literature (1,2) but no data has been given to support these assumptions. The few studies that have been published actually show that improved accuracy is questionable at best (3,4) but fail to address TAT. RAD Assistant (Figure 1) is a Java-based application that has been used for many years by radiologists at Johns Hopkins Hospital (JHH) to give ready access to all clinical notes found in the electronic medical record (EMR), pathology and lab results, and prior radiology reports. One need only click on a link to a history and physical note, for example, to have it immediately pop up in an adjacent window, complete with HPI, physical exam, and assessment/plan. Labs and pathology are equally immediately accessed. Figure 1 Case Presentation By finding a 96-hour time period, when the RAD Assistant server was down on a Monday through Thursday, we were able to compare TAT times for the radiology department both with RAD Assistant available, and unavailable, for use. TAT is defined by the period of time between completion of study (available for reading) to finalization of the report. We ran queries comparing TAT during RAD Assistant downtime, and queries for the same time period the week before, when it was up and running. We also surveyed the attendings, fellows, and residents on if they felt RAD Assistant improved their work experience and reduced their turnaround times or not. Outcome Queries were run to ascertain average TAT for the department as a whole including attendings, fellows, and residents. There are a total of 173 clinical attendings, fellows, and residents at JHH. Average TAT for the 96hour down time period (8681 studies) were compared to a 96-hour up time period (9282 studies) for the immediately preceding week. For the department as a whole, TAT was 18.3% faster during the time period that RAD Assistant was available. Queries were also run to ascertain average TAT for attendings working alone, without preliminary reports from residents or fellows, which showed a 21.2% faster turnaround time when RAD Assistant was available. Further, to measure the more nebulous aspects of having RAD Assistant as part of the radiologist’s normal workflow, a survey was sent out to gauge perception of the effect of RAD Assistant on TAT and how radiologists felt when it wasn’t available. Results from that survey showed that 90% felt that RAD Assistant did reduce turnaround time (Figure 2), 96% felt frustrated when RAD Assistant was down (Figure 3). Interestingly, when RAD Assistant was down, only 30% of users manually looked up all the information they normally would have when RAD Assistant was up (Figure 4). Figure 2 Figure 3 Figure 4 Discussion This study assumes that RAD Assistant use is the major variable of all those affecting turnaround time during the study period. Of course, there are many variables affecting turnaround time including the number of radiologists available, their level of training, the number of studies performed, other computer problems, other down systems, etc. In attempt to minimize confounding variables, we chose an identical time period when RAD Assistant was running the week before which gave a large number of studies and a similar number of available reading radiologists. Another anecdotal benefit from having instant access to relevant clinical data is that it increases confidence in the accuracy of reads. Also, a more complete and accurate reason for study given by the clinician is thought to reduce TAT. While access to our same data set might reveal interesting results, these questions were not the focus of this study. Conclusion The point of this study was to determine if the widespread assumption, often stated in the literature but never really proven, that instant access to relevant clinical information actually reduces TAT. While a tightly controlled study to eliminate confounding variables would be challenging, our study compared two similar 96-hour periods of time during the week when the department was fully staffed to read a large volume of studies. The only readily identifiable and constant difference between these two times was whether instant access to clinical notes and data were available. When it was available, TAT was 24% faster for attendings alone, and 15% faster for attendings working with residents/fellows. At a future date, more information related to accuracy, confidence, and provided clinical information may be available from the same large dataset used for this study. References 1. Mates J, Branstetter BF, Morgan MB, Lionetti DM, Chang PJ. “Wet Reads” in the Age of PACS: Technical and Workflow Considerations for a Preliminary Report System. Journal of Digital Imaging. 2007;20(3):296-306. doi:10.1007/s10278-006-1049-y. 2. McEnery KW, Suitor CT, Hildebrand S, Downs RL. Radiologist's clinical information review workstation interfaced with digital dictation system. J Digit Imaging. 2000 May;13(2 Suppl 1):45-8. 3. Carney PA, Cook AJ, Miglioretti DL, et al. USE OF CLINICAL HISTORY AFFECTS ACCURACY OF INTERPRETIVE PERFORMANCE OF SCREENING MAMMOGRAPHY. Journal of Clinical Epidemiology. 2012;65(2):219-230. doi:10.1016/j.jclinepi.2011.06.010. 4. Good BC, Cooperstein LA, DeMarino GB, Miketic LM, Gennari RC, Rockette HE, Gur D. Does knowledge of the clinical history affect the accuracy of chest radiograph interpretation? AJR Am J Roentgenol. 1990 Apr;154(4):709-12. Keywords History, Relevant Clinical Information, Turnaround Time