Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
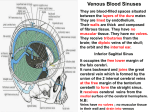
Pamela BL The scalp is the anatomical area that extends from the supraorbital margins of the frontal bones to the superior nuchal lines of the occipital bones and laterally extends over the temporal fascia to the zygomatic arches. The 1. 2. 3. 4. 5. scalp consists of five layers of tissue: Skin Connective tissue Aponeurosis Loose connective tissue Pericranium Skin, thin except in the occipital region. Contains many sweat and sebaceous glands, and hair follicles. Has an abundant arterial supply. Has good venous and lymphatic drainage. Connective tissue, forms the thick, dense, richly vascular zed subcutaneous layer that is well supplied with cutaneous nerves. Aponeurosis, the epicranial aponeurosis-a strong tendinous sheet that covers the calvaria btwn the occipitalis, superior auricular and frontalis muscles(these structures constitute the epicranius muscle). The frontalis; pulls the scalp anteriorly, wrinkles the forehead and elevates the eyebrows. The occipitalis; pulls the scalp posteriorly and wrinkles the skin at the back of the neck. Loose connective tissue, spongy like because of its many potential spaces that may distend with fluid resulting from injury/infection. This layer allows free movement of the 1st three layers over the underlying calvaria. Pericranium, a dense layer of connective tissue that forms the external periosteum of the calvaria. It is firmly attached but can be stripped fairly easily from the calvaria of living people except where it is continuous with the fibrous tissue in the cranial sutures. Innervation of the scalp anterior to the auricles is through branches of all three divisions of cranial nerve V, the trigeminal nerve. Posterior to the auricles, the nerve supply is from spinal cutaneous nerves(C2 and C3). The blood vessels run in layer two of the scalp-the dense subcutaneous layer btwn the skin and epicranial aponeurosis. They are held by the dense connective tissue in such a way that they tend to remain open when cut. Consequently, bleeding from the scalp wound is profuse. Arterial supply of the scalp is from the external carotid artery through the occipital, posterior auricular and superficial temporal arteries. The scalp also receives blood supply from the internal carotid artery through the supraorbital and supratrochlear arteries. The scalp has a rich blood supply, and the arteries anastomose freely with one another in the dense subcutaneous connective tissue layer The venous drainage of superficial parts of the scalp is through the accompanying veins of the scalp arteries-the supraorbital and supratrochlear veins, which begin in the forehead and descend to unite at the medial angle of the eye to form the angular vein that becomes the facial vein at the inferior margin of the orbit. The superficial temporal veins and posterior auricular veins drain the scalp anterior and posterior to the auricles respectively. The occipital veins drain the occipital region of the scalp. Venous drainage of deep parts of the scalp in the temporal region is through deep temporal veins(tributaries of pterygoid venous plexus). There are no lymph nodes in the scalp. Lymph from this region drains into the superficial ring(pericervical collar) of lymph nodes- submental, submandibular, parotid, mastoid/retroauricular and occipital, that is located at the junction of the head and neck. Lymph from these nodes drains into the deep cervical lymph nodes along the IJV. Scalp infections-the loose connective tissue of the scalp is the dangerous area of the scalp because pus or blood can easily spread in it. Infection in this layer can also pass into the cranial cavity through the emissary veins that pass through parietal foramina in the calvaria and infect intracranial structures such as the brain and meninges. An infection cannot pass into the neck because the occipitalis muscle attaches to the occipital bone and mastoid parts of the temporal bones. Neither can a scalp infection spread laterally beyond the zygomatic arches because the epicranial aponeurosis is continuous with the temporal fascia that attaches to these arches. An infection or fluid(blood/pus) can enter the eyelids and the root of the nose because the frontalis inserts into the skin and subcutaneous and does not attach to the bone. Consequently, black eyes result from injury to the scalp/forehead. Most blood enter the upper eyelid, but some may also enter the lower one. Scalp lacerations-are the most common type of head injury requiring surgical care. These wounds bleed profusely because the arteries entering the periphery of the scalp bleed from both ends due to abundant anastomoses. They do not retract when lacerated because they are held open by the dense connective tissue in the 2nd layer of the scalp. Hence an unconscious patient may bleed to death from scalp lacerations if bleeding not controlled. The epicranial aponeurosis is clinically important. Because of its strength, laceration in the skin does mot gape because the margins of the wound are held together by this aponeurosis. Furthermore, when suturing superficial scalp wounds, deep sutures are not necessary because the epicranial aponeurosis does not allow wide separation of the skin. Deep scalp wounds gape widely when the epicranial aponeurosis is spilt or lacerated in the coronal plane because of the pull of the frontal and occipital bellies of epicranius muscle in opposite directions. Cephalotoma, sometimes during a difficult birth, bleeding occurs btwn the baby’s pericranium and calvaria usually over one parietal bone. The bleeding results from rupture of multiple, minute periosteal arteries that nourish the bones of the calvaria. The resulting collection of blood developing several hours after birth is a cephalohematoma. The cranial meninges are internal to the skull. The cranial meninges: 1. Protect the brain 2. Form the supporting framework foe arteries, veins and venous sinuses Enclose a fluid filled cavity, the subarachnoid space(leptomeningeal) which is vital to the normal function of the brain. The 1. 2. 3. cranial meninges consist of three layers: Dura mate(dura)an external, thick fibrous membrane Arachnoid mater(arachnoid-an intermediate, delicate membrane Pia mater(pia)-an internal, delicate vascular membrane.) The meninges also enclose the cerebrospinal fluid and help to maintain the balance of extracellular fluid in the brain. CSF is a clear liquid similar to blood in constitution but has less proteins and a different ion concentration. CSF is formed by the choroid plexuses of the four ventricles of the brain, leaves the ventricular system and enters the subarachnoid space btwn the arachnoid and pia mater where it cushions and nourishes the brain. The dura mater(pachymeninx-thick membrane) a two layered membrane, is adherent to the internal surface of the skull. It consists of: 1. An external periosteal layer, formed by the periosteum covering the internal surface of the calvaria 2. An internal meningeal layer, a strong fibrous membrane that is continuous at the foramen magnum with the spinal dura mater covering the spinal cord. The external periosteal layer is continuous at the cranial foramina with the periosteum on the external surface of the calvaria. It is not continuous with the dura mater of the spinal cord. The meningeal layer is intimately fused with the periosteal layer and cannot be separated from it. In the cranial base the two dural layers are firmly attached and difficult to separate from the bones. The internal meningeal layer of dura draws away from the external periosteal layer of dura to form dural infoldings(reflections), which separate the regions of the brain from each other. The largest of these septa is falx cerebri(cerebral falx). These dural infoldings divide the cranial cavity into compartments that support parts of brain. The dural infoldings include: Falx cerebri(cerebral falx) Tentorium cerebelli(cerebellar tentorium) Diaphragma sellae(sellar diaphragm) Falx is the Latin for sickle, the falces are sickle shaped structures. The falx cerebri, the largest dural reflection lies in the longitudinal fissure and separates the right and left cerebral hemispheres. The falx cerebri attaches in the median plane of the internal surface of the calvaria, from the frontal crest of the frontal bone and crista galli of the ethmoid bone anteriorly to the internal occipital protuberance posteriorly. The falx cerebri ends by becoming continuous with the tentorium cerebelli. The tentorium cerebelli, the 2nd largest dural infolding, is a wide crescentic septum that separates the occipital lobes of the cerebral hemispheres from the cerebellum. The tentorium cerebelli attaches rostrally to the clinoid processes of the sphenoid bone, rostrilaterally to the petrous part of temporal bone and posterolaterally to the internal surface of the occipital bone. The falx cerebri attaches to the tentorium cerebelli and hold it up, giving it a tent like appearance. The tent like shape of the cerebelli tentorium divides the cranial cavity into supratentorial and infratentorial compartments. The supratentorial compartment is divided into right and left halves by the falx cerebri. Its concave anteromedial border is free, producing a gap-the tentorial notch/incisura of tentorium through which the brainstem extends from the posterior into the middle cranial fossa. The cerebellar falx is a vertical dural infolding that lies inferior to the tentorium cerebelli in the posterior part of the posterior cranial fossa, it partially separates the cerebellar hemispheres. The diaphragma sellae, the smallest dural infolding, is a circular sheet of dura that is suspended btwn the clinoid processes forming a roof over the hypophysial fossa in the sphenoid bone. The diaphragma sellae covers the pituitary gland in this fossa and has an aperture for passage of the infundibulum(pituitary stalk) and hypophyseal veins. Tentorial herniation-the opening in the tentorium cerebelli for the brainstem is slightly larger than necessary to accommodate the midbrain. Space occupying lesions like tumors in the supratentorial compartment produce increased intracranial pressure and may cause part of the adjacent temporal lobe of the brain to herniate through the tentorial notch. During tentorial herniation, the temporal lobe may be lacerated by the tough tentorium cerebelli and the oculomotor nerve may be stretched/compressed or both. Such oculomotor lesions produce paralysis of the extrinsic eye muscles supplied by oculomotor nerve. The dural venous sinuses are endothelium lined spaces btwn the periosteal and meningeal layers of the dura, they form where the dural septa attach. Large veins from the surface of the brain empty into these sinuses. And all blood from the brain drains through them into the IJV. The superior sagittal sinus lies in the convex attached border of the falx cerebri. It begins at the crista galli and ends near the internal occipital protuberance at the confluence of sinuses, a meeting place of the superior sagittal, straight, occipital and transverse sinuses. The superior sagittal sinus receives the superior cerebral vein and communicates on each side through slit like openings with the lateral venous lacunae-lateral expansions of the superior sagittal sinus. The inferior sagittal sinus, much smaller than the superior sagittal sinus, runs in the inferior concave free border of the falx cerebri and ends in the straight sinus. The straight sinus is formed by the union of the inferior sagittal sinus with the great cerebral vein. It runs inferoposteriorly along the line of attachment of the falx cerebri to the tentorium cerebelli where it joins the confluence of sinuses. The transverse sinuses pass laterally from the confluence of sinuses grooving the occipital bones and the posteroinferior angles of parietal bones. The transverse sinuses course along the posterolateral attached margins of the tentorium cerebelli and become sigmoid sinuses as they approach the posterior aspects of the petrous temporal bones. Blood received by the confluence of sinuses is drained by the transverse sinuses but rarely equally. Usually the left sinus is dominant(larger). The sigmoid sinuses follow S-shaped courses in the posterior cranial fossa forming deep grooves in the temporal and occipital bones. Each sigmoid sinus runs anteriorly and then continues inferiorly as the IJV after traversing the jugular foramen. The occipital sinus lies in the attached border of the cerebellar falx and ends superiorly in the confluence of sinuses. The occipital sinus communicates inferiorly with the internal vertebral venous plexus. The cavernous sinus/lateral sellar compartment is situated bilaterally on each side of the sella turcica on the upper surface of the body of the sphenoid bone, which contains the sphenoidal(air) sinus. Each sellar compartment contains a cavernous sinus consisting of a venous plexus of extremely thin walled veins. The superior petrosal sinuses run from the posterior ends of the veins comprising the cavernous sinus to the transverse sinuses at the site where these sinuses curve inferiorly to form the sigmoid sinuses. Each superior petrosal sinus lies in the anterolateral attached margin of the tentorium cerebelli, which attaches to the superior border of the petrous part of the temporal bone. The inferior petrosal sinuses also commence at the posterior end of the cavernous sinus inferiorly. Each inferior petrosal sinus runs in the groove btwn the petrous part of temporal bone and the basilar part of occipital bone. The inferior petrosal sinuses drain the veins of the lateral cavernous sinus directly into the origin of IJV.