Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
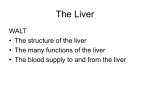
C. Stefanutti et al.: Liver Dysfunction supportive therapies C. Stefanutti1, G. Novelli2, V. Morabito2, S. Di Giacomo1, G. Labbadia1 Transplantationsmedizin 2010, 22. Jahrg., S. 325 Liver Dysfunction Supportive Therapies – From Therapeutic Plasmapheresis to Molecular Adsorbent Recirculating System Background: Because of the scarcity of donor organs, liver support strategies are being developed with the aim of either supporting patients with borderline functional liver cell mass until an appropriate organ becomes available for transplantation. Up until ten years ago Therapeutic Plasmapheresis (TPE) and Continuous Renal Replacement Therapy (CRRT) were the main treatment used. Currently, non-biological systems include Molecular Adsorbent Recirculating System (MARS) which is not only used as “bridging therapy” but also until liver recovery without necessity of liver transplantation (LT). Methods: This report focus on TPE in the form of Plasma-Exchange (PE) that was introduced in our clinical activity since 1987, and MARS utilized since 1999. The above systems were used as bridging therapy either to optimize the clinical status for LT or resolution without necessity to LT with acceptable results. Results: 1326 procedures of TPE on 101 patients with liver dysfunction were carried out from 1987 to 1999. Liver function impairment was related to Acute on Chronic Hepatic Failure (AoCHF) (#76), Fulminant Hepatitis (FH) (#23), Intractable Pruritus (IP) (#2). Since 1999, 2866 treatments on 269 patients were performed with MARS for ACLF [acute-on-chronic liver failure] (#140), FH (#46); Delayed Function (#22), Primary No Function (#18), Acute Hepatic Failure (AHF) after surgery (#25), and IP (#17). The most recent data relative to treatment in our departments in the last 12 months (2009-2010) of patients with TPE (#5 patients) and with MARS (#10 patients) has been reported. Conclusion: According to our clinical experience TPE can lower efficaciously bilirubin and hepatic enzymes. MARS detoxifies great volumes of blood and eliminates pro-inflammatory molecules. TPE daily performed may be helpful in AoCHF patients until transplantation takes place. MARS shows significant improvement above all in AoCHF and in FH. Key words: Bilirubin, therapeutic plasmapheresis, plasma exchange, continuous renal replacement therapy, molecular adsorbent recirculating system Department of Clinical and Medical Therapy; Plasmapheresis Unit, 2Department “Paride Stefanini”; General Surgery and Organs Transplant; “Sapienza” University of Rome; Italy Supportive Therapien bei Leberfunktionsstörungen – von therapeutischer Plasmapherese bis zu MARS (Molecular Adsorbent Recirculating System) Stefanutti C, Novelli G, Morabito V, Giacomo S, Labbadia G (2010) Liver Dysfunction Supportive Therapies – From Therapeutic Plasmapheresis to Molecular Adsorbent Recirculating System. Tx Med 22: 325-332 Hintergrund: Aufgrund des Mangels an Spenderorganen werden Strategien zur Unterstützung der Leber entwickelt, mit denen Patienten mit grenzwertig funktioneller Leberzellmasse behandelt werden sollen, bis ein geeignetes Organ zur Verfügung steht. Bis vor zehn Jahren waren die Therapeutische Plasmapherese (TPE) und die Kontinuierliche Nierenersatztherapie (CRRT) die am meisten eingesetzten Behandlungen. Heute 1 Transplantationsmedizin 2010, 22. Jahrg., S. 326 C. Stefanutti et al.: Liver Dysfunction supportive therapies gehört zu den nicht-biologischen Systemen das "Molecular Adsorbent Recirculating System" (MARS), das nicht nur als "Überbrückung" verwendet wird, sondern auch bis zur Erholung der Leber ohne Notwendigkeit einer Transplantation (LT). Methoden: Dieser Bericht konzentriert sich auf die TPE in Form von Plasmaaustausch (PE), die 1987 in unsere klinische Praxis eingeführt wurde, und auf das MARS-System, das seit 1999 verwendet wird. Die obigen Systeme wurden mit akzeptablen Ergebnissen als "Überbrückung" eingesetzt, entweder um den klinischen Zustand des Patienten für die LT zu verbessern oder bis zur Besserung der Leberfunktion ohne Transplantationsnotwendigkeit. Ergebnisse: 1326 TPE-Anwendungen wurden an 101 Patienten mit Leberfunktionsstörungen im Zeitraum von 1987 bis 1999 durchgeführt. Die Beeinträchtigung der Leberfunktion bezog sich auf "Acute on Chronic Hepatic Failure" (AoCHF) (n=76), Fulminante Hepatitis (FH) (n=23) und hartnäckigen Pruritus (IP) (n=2). Seit 1999 wurden 2866 Behandlungen an 269 Patienten mit MARS durchgeführt zur Behandlung von ACLF [acute-on-chronic liver failure] (n=140), FH (N=46), verzögerter Transplantatfunktion (n=22), primärer Nichtfunktion (n=18), akutem Leberversagen (AHF) nach der Operation (n=25) und IP (n=17). Die neuesten Daten zu den in den vergangenen 12 Monaten (2009 bis 2010) in unseren Abteilungen durchgeführten Behandlungen (TPE: n=5 Patienten und MARS: n=10 Patienten) wurden berichtet. Schlussfolgerung: Nach unserer klinischen Erfahrung kann TPE Bilirubin und Leberenzyme effizient verringern. Das MARS-System entgiftet große Mengen an Blut und entfernt entzündungsfördernde Moleküle. Eine täglich durchgeführte TPE könnte AoCHF-Patienten bis zur geplanten Transplantation helfen. MARS zeigt hauptsächlich bei AoCHF und bei FH eine signifikante Verbesserung. Schlüsselwörter: Bilirubin, therapeutische Plasmapherese, Plasmaaustausch, kontinuierliche Nierenersatztherapie, Molecular Adsorbent Recirculating System Introduction AHF is the sudden destruction of hepatic cells in individuals with no history of hepatic disease. The plasma ammonia concentration increases and cannot be metabolized to urea. Hepatic coma is the following severe complication. On the other hand, bile cannot be excreted, the bilirubin concentration increases, and jaundice and other symptoms related to liver failure occur. The therapeutic intervention consists in nutritional management, CRRT or TPE and other extracorporeal techniques performed to support the patient until liver function is recovered or the patient is submitted to LT (1-9), and AHF lead to hepatic failure and hepatic encephalopathy due to severe liver dysfunction resulting from marked, widespread hepatocyte necro- sis. These two critical, life-threatening diseases are still difficult to treat in emergency medicine. TPE, CRRT, and other extracorporeal procedures are performed for artificial liver support (ALS) in critical care (10-16). ALS results in significant improvement in the patient’s systemic condition. Even the consciousness is maintained. The above mentioned systems are also effective as a bridging therapy to LT (17-20). In these patients, CRRT is used because it allows a slow, moderate blood purification process to reduce the patient’s burden. CRRT is indicated in patients with severe acute pancreatitis (TPE is also indicated), FH, postoperative liver failure, multiple organ failure, cardiovascular disease, and severe renal failure (3,16,21,22). CRRT is provided mainly in critical care and intensive care units. More recently, MARS which has higher detoxification level has been used successfully (23-25). Hyperbilirubinemia is characterized by elevated plasma bilirubin concentrations due to hemolytic anemia, alcoholic hepatitis, liver stones, etc. When the plasma bilirubin concentration becomes greater than 3.0 mg/dL, the patient exhibits jaundice. Plasma adsorption (PA) or PE are performed to remove excessive bilirubin and bile acid from the blood (1,46,8,9,11). To eliminate protein-bound toxic substances, PE was introduced. In the case of FH or other hepatic failure, the supply of coagulation factors is usually necessary; therefore, PE is a suitable method for the elimination of protein-bound toxins, for example, bilirubin. PE needs fresh frozen plasma or another protein fraction from humans. In the case of bilirubin, anion exchange resin was also used to try to eliminate this toxic substance from the patient’s blood or plasma using a bilirubin adsorption column for plasma perfusion (8,9,11). The therapeutic effects of the above mentioned systems in a wide range of hepatic failure patients are reported in literature although some studies show conflicting results. This survey was aimed to review retrospectively the clinical records of the patients with severe liver function decompensation accepted at our Departments in the years 2009-2010, and submitted to intensive treatment to remove toxins of hepatic failure with non-biological systems such as TPE and MARS. Patients and Methods (TPE) The records of all patients at our Department undergoing a total of 97 TPEs between 2009 and 2010 were retrospectively reviewed. TPE was performed more frequently before 1999, at which time an aggressive LT policy was instituted. The indication for TPE was acute and chronic hepatic failure, candidacy for LT, and coagulopathy (prothrombin time [PT] > 20 seconds). In the last 12 months # 5 patients (males: #4; females: #1) were submitted to TPE. Daily TPE was performed until the patient recovered, died, or underwent LT. Age at time of treatment was 53±18.4 years. The primary etiology of liver failure was acute decompensation of chronic liver disease (Figure 1). C. Stefanutti et al.: Liver Dysfunction supportive therapies Fig. 1: Primary etiology of liver failure in patients treated with MARS Treatment with TPE The basic procedure consists of removal of blood, separation of blood cells from plasma, and return of these blood cells to the circulation, diluted with fresh plasma or a substitute. Because of concerns over viral infection and allergic reaction, fresh plasma is not routinely used. The most common substitute is saline solution with sterilized human albumin protein. During the course of a single session, two to three liters of plasma is removed and replaced. TPE requires insertion of a venous catheter, either in a limb or central vein. Central veins allow higher flow rates and are more convenient for repeat procedures, but are more often the site of complications, especially bacterial infection. The patients underwent urgent treatment of TPE (a written informed consensus was obtained by the patient or parents in case of loss of consciousness). 1-1.5 plasma volume x procedure was processed (frequency: daily). The vascular accesses utilized were: central venous catheter (CVC) or peripheral venous accesses. According to our extracorporeal treatment protocol, heparin 5000 UI intravenous as a bolus was administered at the beginning of the procedure, while continuous anticoagulation during treatment is guaranteed by the use of Anticoagulant Citrate Dextrose Solution A (ACD-A) ACD-A can be used in a ratio of 1:25–50 to prevent severe hypocalcemia in AHF. Although the plasma is preferable as a replacement fluid due to moderate to severe coagulopathy in AHF, addition of albumin is acceptable. In this sample both plasma and albumin 5% as replacement fluids, were used. The centrifugal apheresis system used was “Spectra” COBE, LRS System Turbo Version 7.0 (COBE Laboratories, Inc., Lakewood, CO, USA). Safety (TPE) When blood is outside the body, it must be treated to prevent it from clotting. While most of the anticlotting agent is removed from the blood during treatment, some is returned to the patient. Side Effects Immediate (related to extracorporeal line, anticoagulation, and replacement fluids): vagus nerve syndrome, low or high blood pressure; venous puncture hazards, air embolism; excessive bleeding, allergy or thrombopenia induced by heparin, citrate poisoning with hypocalcemia symptomatology (headachecramps-swarming-tetanus rarely cardiac arythmia); chills-fever; nauseavomiting, diarrhea (albumin). Delayed (impaired hemostasis): hypocoagulative state 8-12 hours after session; hypercoagulative state 24-72 hours by rebound effect (antithrombin 3 synthesis delayed) and increased thrombosis risk (promoting conditions: inflammation, confinement to bed). Preventive heparin treatment with normal coagulation tests is needed. Patients and Methods (MARS) From February 2009 to February 2010, fourty-nine patients were treated with MARS. In this paper 10 of these patients with acute decompensation of cirrhosis manifested by increasing jaun- Transplantationsmedizin 2010, 22. Jahrg., S. 327 dice and encephalopathy grade I-II will be considered. A written informed consensus was obtained by the patient or parents in case of loss of consciousness. Three patients affected by cirrhosis HBV-related; three patients by cirrhosis HCV-related, two patients by cirrhosis alcohol-related; one patient by primary biliary cirrhosis and one patient by cirrhosis HCV- and alcohol-related. These patients (8 male and 2 female) were treated with MARS® (Gambro Stockholm, Sweden) in association with equipment for dialysis machine Hospal Integra® (Gambro, Zaventem, Belgium). The mean age of these patients was 49.3 ± 5.9 years. The mean number of MARS procedures was 6.5 (range 48). Each procedure lasted approximately 8 hours. The patients were evaluated from their enrolment with a survival follow up at three months. Vascular access was obtained by insertion of a double lumen dialysis catheter (Arrow International, Reading, PA, USA) into the right internal jugular vein in two patients and into subclavian vein in eight patients. For anticoagulation, a bolus of 2.500 units of unfractionated heparin was injected into the extracorporeal system during the priming, followed by flushing saline solution every 60 minutes. Two patients presented transitory hypotension (80/40 mmHg) that was positively corrected through administering saline solution and cortisone. Three patients with transitory hypoglycaemia were treated with glucose solution (33%). The thrombocytopenia was controlled through administration of platelets before the start of treatment when the patients showed levels under 50.000 mm3 (two patients). During the sessions, fresh frozen plasma was administered to all patients. Survival data were obtained from hospital medical records as well as clinic notes. Patients were examined before and immediately after MARS. Neurologic status was determined by clinical assessment using a standard hepatic encephalopathy scale and was correlated with the concentration of blood ammonia. Treatment with MARS MARS® (Gambro Stockholm, Sweden) is a blood purification technique which can remove all known substances that accumulate in the blood during liver failure and cause hepatic dysfunction Transplantationsmedizin 2010, 22. Jahrg., S. 328 and neurological abnormalities, aggravate injury to the liver and other organs and inhibit hepatic regeneration. After the introduction of MARS in 1999 our clinical experience has forced us to focus on four aspects concerning this technique: safety, coagulopathy, pump volume flow rate and albumin function. Since 1999, 2866 procedures on 269 patients were performed with MARS. From 2004 we started working closely with a group of engineers from “La Sapienza” University of Rome. Our aim was to optimize MARS treatment by clinically applying what had already been demonstrated in in-vitro studies through the application of a mathematical model (26). By applying this model, improved clearance of different substances (35%) was observed. Safety (MARS) The treatment with MARS can be considered biologically compatible, comprehensive and highly secure. At 2.688 treatments performed, we found 1.81% complications more likely related to the former clinical conditions of patients before treatment. We have observed: severe hypotension (1.7% of sessions had a clinical record of blood pressure of 60/40 mmHg not modifiable by medical therapy or by the interruption of procedure), and bleeding from CVC with change in ranking (4.1%) and infections of CVC catheter, substituted every 15 days (29%) from 1999 to 2002, and since 2003 with replacement of CVC after 10 days (21.7%) at new site. Laboratory Methods Clinical laboratory measurements were performed in a certified central university hospital laboratory. The pattern of coagulopathy was assessed by determination of PT (adjusted to International Normalized Ratio [INR]) and the partial thromboplastin time. Measurements of individual clotting factors were taken before and immediately after exchange and included fibrinogen, factor II, factor V, factor VII, and factor IX. Standard biochemistry panels were taken 1 hour after TPE or MARS and included measurements of sodium, potassium, chloride, bicarbonate, and liver function tests (bilirubin, aspartate transaminase, AST and alanine transaminase, ALT). C. Stefanutti et al.: Liver Dysfunction supportive therapies Laboratory parameters were determined by usual enzymatic and chemical methods. The blood cell count was determined with a Beckman Coulter ACT Diff. (Beckman Coulter, S.p.A, Milan, Italy-EU). Model for End-Stage Liver Disease (MELD) score was evaluated according the following formula: 3.8 x log (e) (bilirubin mg/dL) + 11.2 x log (e) (INR) + 9.6 log (e) (creatinine mg/dL). Creatinine clearance rate (Glomerular Filtration Rate: GFR) was estimated using Cockcroft-Gault formula (27). bly, Venice, Italy, October 1983, and the 41st World Medical Assembly, Hong Kong, September 1989. Ethics Results Informed consent was obtained from all patients or their families, according to the recommendations of the declaration of Helsinki guiding physicians in biomedical research involving human subjects. Adopted by the 18th World Medical Assembly, Helsinki, Finland, June 1964, amended by the 29th World Medical Assembly, Tokyo, Japan, October 1975, the 35th World Medical Assem- The data refers to therapeutic management over the last 5 patients with AHF undergoing treatment through TPE (tables 1, 2) and of the last 10 cases treated with MARS (tables 3, 4, 5) over a period of 12 months, between 2009 and 2010. Patients treated with TPE were two males and 3 females between 58 and 72 years of age (table 1). Those given treatment with MARS were 10 pa- Statistical Analysis Statistical analysis was performed according to parametric tests, depending on parameters under evaluation. All results are expressed as means ± SD. Within group differences were tested for statistical significance using Student’s t test for paired data. Tab. 1: Demographic and biochemical characteristics of # 5 patients with AHF submitted to TPE (12 months: 2009-2010) Patients 1 2 3 4 5 Gender F F M M F Age (years) 46 46 46 72 58 ALT * 185 318 226 68 235 AST 50 134 248 93 84 Total Bilirubin ** 13.4 34.5 44 16 15.6 Ammonia *** 82 192 151 85 122 ALT before 140± 59 314± 46 103.5± 7.5 59.5± 9.5 42± 1 ALT after 83.5± 17.5 141± 27 61.5± 1.5 48± 17 24± 12 AST before 254± 51 362.5± 21.5 150± 60 61.5± 1.5 112.5± 18.5 AST after 163± 42 163± 9 83± 25 51± 10 72.5± 9.5 Total Bilirubin before 27± 1 32± 1 32± 5 27.6± 1.7 19.6±3.5 Total Bilirubin after 13.5± 0.5 14.5± 1.5 19.5± 7.5 17.5± 1.5 9± 2 Ammonia 82 192 151 85 122 Ammonia I session 138 121 151 60 53 Ammonia II session 114 107 158 90 80 Baseline Treatment (TPE) *: UI/L; **: mg/dL; ***: mcg/dL C. Stefanutti et al.: Liver Dysfunction supportive therapies mg/dL Transplantationsmedizin 2010, 22. Jahrg., S. 329 X±SD Total bilirubin before 27.4±9.7 Total Bilirubin after 14.5 ±14.4 ^ Nitrogen before 100±106 Nitrogen after 80.9±118.1 Creatinine before 0.95±0.61 Creatinine after 0.76±0.71 GFR * ml/min Tab. 2: Total bilirubin and renal function in # 5 patients with AHF submitted to TPE 96.4±31 ^: P=0.001 *: evaluated according Cockcroft-Gault's formula Tab. 3: Demographic and biochemical characteristics of # 5 patients (whole sample # 10) with AHF submitted to MARS (12 months: 2009-2010) Patient 1 2 3 4 5 Age (years) 45 41 47 59 49 Gender F M M M M Liver disease Alcohol-related Cirrhosis HBV-related Cirrhosis HBV-related Cirrhosis HCV-Alcohol related Cirrhosis Alcohol-related Cirrhosis # treatments 7 5 6 7 7 MELD pre 32 32 28 30 33 MELD post 22 29 18 17 23 A A A D A Outcome (3 months) AST pre 113 122 144 62 254 AST post 101 102 97 157 70 ALT pre 230 112 124 225 229 ALT post 201 153 99 89 111 Tot Bilirubin pre 19 32 16 24 19 Tot Bilirubin post 9 18 9 7.9 9.1 Ammonia pre 287 129 118 117 123 Ammonia post 76 53 64 130 61 Albumin pre 3 2.7 2.5 2 2.9 Albumin post 3.4 3 2.4 2 3.3 INR pre 3.1 3.1 2.6 2.3 2.9 INR post 1.9 2.8 1.3 1.3 2.1 Urea pre 25 62 37 65 49 Urea post 11 12 14 26 15 Creatinine pre 1.2 0.7 0.7 1.2 1.4 Creatinine post 0.9 1 0.6 0.7 0.5 MELD: Model for End-Stage Liver Disease score; Outcome: Alive (A), Deceased (D); INR: International Normalized Ratio; AST: Aspartate transaminase; ALT: alanine transaminase tients of an average age of 49.3 ± 5.9 (table 5). In the group of patients who underwent TPE, liver and renal functions were taken into consideration. In table 1, values are reported of ALT, of AST, total bilirubin and ammonia to the baseline and in treatment with TPE. The values of the above mentioned variables improved after treatment as expected. In particular, the average variation of the total bilirubin results as being statistically significant. (P=0.001). Also in table 1 there is reference to the ammonia that demonstrates a not linear devel- opment and which is different in every patient. In table 2 values have been reported before and after TPE, of nitrogen, creatinine and GFR. In tables 3 and 4 data is reported in reference to liver and renal functions and the correction of coagulopathy (INR) and the MELD Transplantationsmedizin 2010, 22. Jahrg., S. 330 C. Stefanutti et al.: Liver Dysfunction supportive therapies Tab. 4: Demographic and biochemical characteristics of # 5 patients (whole sample # 10) with AHF submitted to MARS (12 months: 2009-2010) Patient 6 7 8 9 10 Age (years) 48 47 47 50 60 Gender M F M M M Liver disease Primary Biliary Cirrhosis HCV-related Cirrhosis HCV-related Cirrhosis HCV-related Cirrhosis HBV-related Cirrhosis # treatments 4 6 7 8 8 MELD pre 32 32 34 29 27 MELD post 32 21 28 20 20 D D D A A AST pre 266 216 117 108 210 AST post 256 92 68 104 201 ALT pre 129 78 94 222 185 ALT post 121 104 170 287 305 Tot Bilirubin pre 32.6 16.4 24 44 31 Tot Bilirubin post 28.4 11 7.2 19 12 Ammonia pre 132 121 128 120 232 Ammonia post 84 134 138 73 111 Albumin pre 2.4 2.1 2.7 2.5 3.1 Albumin post 2.5 2.3 2.9 3.1 3.4 INR pre 3.1 2.3 3.3 2.1 2 INR post 2.8 1.2 2.2 1.2 1.4 Urea pre 55 87 64 52 39 Urea post 48 74 38 24 15 Creatinine pre 0.7 1.9 1.3 0.9 0.6 Creatinine post 1.1 1.4 1.8 0.6 0.6 Outcome (3 months) MELD: Model for End-Stage Liver Disease score; Outcome: Alive (A), Deceased (D); INR: International Normalized Ratio; AST: Aspartate transaminase; ALT: alanine transaminase X ± SD Age (years) P 49.3 ± 5.9 # treatments 6.5 ± 1.2 MELD before 30.9 ± 2.2 MELD after 23 ± 2.2 AST before 161.2 ± 70 AST after 124.8 ± 61.1 ALT before 163 ±61.3 ALT after 164 ± 78 Tot Bilirubin before 25.8 ± 9 Tot Bilirubin after 13.06 ± 7 Ammonia before 151 ± 59 Ammonia after 91.6 ± 31.5 Albumin before 2.54 ± 0.3 Albumin after 3 ± 0.4 INR before 2.2 ± 0.4 INR after 2 ± 0.6 Urea before 53.5 ± 17.5 Urea after 28 ± 2.2 Creatinine before 1 ± 0.4 Creatinine after 0.9 ± 0.4 Tab. 5: Demographic and biochemical characteristics (X ± SD) of # 10 patients with AHF submitted to MARS (12 months: 2009-2010) 0.001 ns ns 0.001 ns ns ns 0.001 ns MELD: Model for End-Stage Liver Disease score; Outcome: Alive (A), Deceased (D); INR: International Normalized Ratio; AST: Aspartate transaminase; ALT: alanine transaminase; ns: not significant C. Stefanutti et al.: Liver Dysfunction supportive therapies score in patients who underwent treatment with MARS. In tables 3 and 4, the pathology that determined AHF in each patient and not only the necessity of treatment with MARS has been reported. Also reported in these tables is the clinical outcome of survival at 3 months. In the follow up at 3 months 6 patients were alive (A), while 4 patients were deceased (D). Finally, in table 5, the mean ± standard deviation of the variables given before and after treatment with MARS, with the exception of the clinical outcome, have been reported. The MELD score, the total bilirubin and the urea, demonstrate a variation which is statistically significant after treatment (all variables: P=0.001). Discussion Without spontaneous recovery of liver function, the standard treatment of AHF is supportive care as a bridge to LT. Plasmapheresis is indicated in severe hepatic disease, metabolic disease, collagen disease, autoimmune disease, neurological disease (12,13,28). Centrifugation and membrane separation techniques are used for plasma separation. There are four main types of membrane plasmapheresis: plasma exchange (PE), double filtration plasmapheresis (DFPP), plasma adsorption (PA), and immunoadsorption (IA). ASFA has categorized the use of TPE in Acute Liver Failure as a Category III (Strenght of evidence II-3) indication: “suggestion of benefit for which existing evidence is insufficient, either to establish the efficacy of therapeutic apheresis or to clarify the risk/benefit (or sometimes the cost/benefit) ratio.” (29). In AHF, TPE removes albumin bound and large molecular weight toxins – aromatic amino acids, ammonia, endotoxin, indols, mercaptans, phenols –, and other factors. The increase in plasma of these toxic substances may be responsible for hepatic coma, hyperkinetic syndrome, decreased systemic vascular resistance, and cerebral blood flow. TPE restores hemostasis by supplying the coagulation factors and removing activated clotting factors, tissue plasminogen activator, fibrin, and fibrinogen degradation products. It was also reported improved cerebral blood flow, mean arterial pressure, cerebral perfusion pressure and cerebral metabolic rate, in- creased hepatic blood flow, after TPE. Laboratory parameters such as cholinesterase activity, or galactose elimination capacity were improved by TPE. In some patients, the liver may regenerate during TPE and in other patients TPE can be viewed as bridging therapy to LT (17-19). The molecular adsorbent recirculating system (MARS) represents a cell-free, extracorporeal, liver assistance method for the selective removal of albumin-bound substances (23-25). Moreover, it enables the removal of excess water and water-soluble substances via an inbuilt dialysis step. According to our previous clinical experience and even in the last case series TPE can lower bilirubin and hepatic enzymes, meanwhile improving coagulopathy in AHF. TPE performed daily may be helpful until transplantation takes place or self-regeneration occurs. A limitation in our interpretation of the available data is that we have a poor knowledge about the clinical outcome as our therapeutic plasmapheresis unit usually is requested to treat patients from other departments that have a major role in the clinical management of patients and consecutive clinical evolution. On the contrary the department of general surgery and organs transplant has a complete awareness of what is the life expectancy and the survival rate of patients submitted to MARS. Moreover their clinical management of the patients is not limited to the extracorporeal treatment but also finalized to the LT. MARS has a role in the treatment of liver failure where the primary goal is to provide blood purification. Notwithstanding the response to TPE or MARS should be evaluated daily. In fact, the improvement determined by the removal of bilirubin and hepatic enzymes and other toxic substances does not necessarily reflect a favourable change in the patient’s clinical condition which can be highly critical and irreversible. To conclude, liver dysfunction supportive therapies are essential techniques when the clinical target is to make any effort to control severe, overwhelming and above all life-threatening liver failure, and valuable bridging therapies supporting the decision making process leading to the LT (28,30-32). The data reported in the present survey which refers to the use of TPE and MARS in our departments over the last 12 months confirms our data which is already available and reported in literature. In Transplantationsmedizin 2010, 22. Jahrg., S. 331 our opinion, these are superimposable to findings reported by other authors. The tendency in our hospital is for progressive increase in the use of MARS in grave hepatic insufficiency in patients who are awaiting or not awaiting LT, without undermining the therapeutic importance of TPE which is widely used in the same pathology. Conflict of Interest and Financial Disclosure The authors certify that they have no affiliation with or financial involvement in any organization or entity with a direct financial interest in the subject matter or materials discussed in this manuscript. References 1. Freeman JG, Matthewson K, Record CO (1986) Plasmapheresis in acute liver failure. Int J Artif Organs 9: 433-438 2. Stefanutti C, Russo A, Pretagostini R, Lopez A, Quaglia MG (1992) Role of extracorporal removal techniques in clinical toxicology. XV International Congress of the European Association of Poison Centres and Clinical Toxicologists. Istanbul, Türkiye, May 25-27 1992. Abstract, p. 84 3. Okada M, Kioka Y, Masui Y, Kondou H (1996) New Treatment of Myonephropathic Metabolic Syndrome: Concomitant Plasma Exchange and Continuous Venovenous Hemofiltration. Jpn J Apheresis 15 (1): 137-138 4. Singer AL, Olthoff KM, Kim H, Rand E, Zamir G, Shaked A (2001) Role of Plasmapheresis in the Management of Acute Hepatic Failure in Children. Ann Surg 234 (3): 418-424 5. Kondrup J, Almdal T, Vilstrup H et al. (1992) High-volume plasma exchange in fulminant hepatic failure. Int J Artif Organs 15: 669-676 6. Place E, Wenzel JE, Arumugam R, Belani K, Messinger Y (2007) Successful plasmapheresis for extreme hyperbilirubinemia caused by acute Epstein-Barr virus. J Pediatr Hematol Oncol 29 (5): 323-6 7. Rozga J, Podesta L, LePage E et al. (1994) A bioartificial liver to treat severe acute liver failure. Ann Surg 219: 538-546 8. Yang KS, Kenpe K, Yamaji K, Tsuda H, Hashimoto H (2002) Plasma adsorption in critical care. Ther Apher 6 (3): 184-8 9. Yoshinori Takenaka (2007) Bilirubin Adsorbent Column for Plasma Perfusion. Therap Apher Dial 2 (2): 129-133 10. Hirasawa H, Sugai T, Oda S et al. (1997) Efficacy and limitation of apheresis therapy in critical care. Ther Apheresis 1: 228-232 11. Mineshima M, Akiba T (2002) Double filtration plasmapheresis in critical care. Ther Apher 6 (3): 180-3 12. Siami GA, Siami FS (2001) Membrane plasmapheresis in the United States: a review over the last 20 years. Ther Apher 5 (4): 315-20 13. Bosch T (2003) Recent advances in therapeutic apheresis. J Artif Organs 6 (1): 1-8 14. Mineshima M, Yokoi R, Horibe K et al. (2001) Effects of operating conditions on selectivity of a plasma fractionator in double filtration plasmapheresis. Ther Apher 5 (6): 444-8 Transplantationsmedizin 2010, 22. Jahrg., S. 332 15. Stefanutti C, Vivenzio A, Di Giacomo S et al. (1996) A new treatment of refractory ascites: ascitoapheresis. J Clin Apheresis 11: 46-47 16. Barshes NR, Gay AN, Williams B, Patel AJ, Awad SS (2005) Support for the acutely failing liver: a comprehensive review of historic and contemporary strategies. J Am Coll Surg 201 (3): 458-76 17. Gibbons RD, Meltzer D, Duan N (2000) Waiting for organ transplantation. Institute of Medicine Committee on Organ Transplantation. Science 287: 237-238 18. Skerrett D, Mor E, Curtiss S et al. (1996) Plasmapheresis in primary dysfunction of hepatic transplants. J Clin Apheresis 11: 10-3 19. Mandal AK, King KE, Humphreys SL et al. (2000) Plasmapheresis: an effective therapy for primary allograft nonfunction after liver transplantation. Transplantation 70: 216-220 20. Novelli G, Rossi M, Pugliese F et al. (2007) Molecular Adsorbents Recirculating System Treatment in Acute-on-Chronic Hepatitis Patients on the Transplant Waiting List Improves Model for End-Stage Liver Disease Scores. Transplantation Proceedings 39: 1864-1867 21. Naruse K, Tang W, Makuuch M (2007) Artificial and bioartificial liver support: a review of perfusion treatment for hepatic failure patients. World J Gastroenterol 13 (10): 1516-21 22. Stefanutti C, Di Giacomo S, Vivenzio A et al. (2009) Therapeutic Plasma Exchange in Patients with Severe Hypertriglyceridemia: a Multicenter study. Artif Organs 33 (12): 1096-1102 C. Stefanutti et al.: Liver Dysfunction supportive therapies 23. Mitzner SR, Jan Stange J, Klammt S, Peszynski P, Schmidt R, Nöldge-Schomburg G (2001) Extracorporeal Detoxification Using the Molecular Adsorbent Recirculating System for Critically Ill Patients with Liver Failure. J Am Soc Nephrol 12: S75-S82 24. Novelli G, Rossi M, Pretagostini R et al. (2002) MARS (Molecular Adsorbent Recirculating System): experience in 34 cases of acute liver failure. Liver 22 (s2): 43-47 25. Novelli G, Rossi M, Ferretti G et al. (2009) Predictive criteria for the outcome of patients with acute liver failure treated with the albumin dialysis molecular adsorbent recirculating system. Ther Apher Dial 13 (5): 404-12 26. Annesini MC, Piemonte V, Turchetti L (2007) Artificial Liver Optimization: Analysis of Albumin Bound Toxin Adsorption. Chemical Engineering Transactions 11: 551-556 27. Cockcroft DW, Gault MH (1976) Prediction of creatinine clearance from serum creatinine. Nephron 16: 31-41 28. Hung YM, Hung GC, Hsu PI, Hung SY, Chou KJ, Chung HM (2004) Short-term survival advantage after plasma exchange in the treatment of acute on chronic liver failure or acute liver failure. Clinical Intensive Care 15 (2-3): 93-99 29. Szczepiorkowski ZM, Shaz BH (2007) The new approach to assignment of ASFA categories-introduction to the fourth special issue: clinical applications of therapeutic apheresis. J Clin Apher 22: 96-105 30. Kjaergard LL, Liu J, Als-Nielsen B, Gluud C (2003) Artificial and Bioartificial Support Systems for Acute and Acute-on-Chronic Liver Failure. JAMA 289: 217-222 31. Pless G, Sauer IM (2005) Bioartificial liver: current status. Transplant Proc 37: 3893-3895 32. Yu CB, Pan XP, Li LJ (2007) Progress in bioreactors of bioartificial livers. World J Gastroenterol 13 (10): 1516-21 Claudia Stefanutti, M.D., Ph.D. Professor of Internal Medicine Department of Clinical and Medical Therapy Plasmapheresis Unit University of Rome “La Sapienza” “Umberto I” Hospital 155, Viale del Policlinico I-00161 Rome Italy [email protected]