Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Neuropsychopharmacology wikipedia , lookup
Orphan drug wikipedia , lookup
Adherence (medicine) wikipedia , lookup
Psychopharmacology wikipedia , lookup
Compounding wikipedia , lookup
Drug design wikipedia , lookup
Pharmaceutical marketing wikipedia , lookup
Neuropharmacology wikipedia , lookup
Electronic prescribing wikipedia , lookup
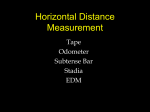
Theralizumab wikipedia , lookup
Drug discovery wikipedia , lookup
Pharmacokinetics wikipedia , lookup
Pharmacognosy wikipedia , lookup
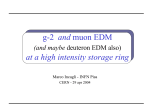
Drug interaction wikipedia , lookup
Pharmacogenomics wikipedia , lookup
Pharmaceutical industry wikipedia , lookup
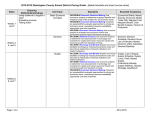
Safety issues of drug use WHO/EDM Technical briefing seminar 2 October 2002 Geneva Lembit Rägo, MD, PhD Coordinator,Quality Assurance and Safety: Medicines Essential Drugs and Medicines Policy Health Technology and Pharmaceuticals Cluster World Health Organization E-mail: [email protected] Pharmaceutical gaps Very different regulatory environments, and likely very different priorities for regulators Huge differences exist in regulatory environment - from 191 WHO Member States One third have advanced regulatory systems One third have some regulatory systems One third have practically no functioning regulatory systems How to guarantee safety in circumstances where regulatory framework is either absent or functioning poorly? WHO - EDM 2 WHO essential drugs & medicines strategy 4 objectives guide country, regional, global work (http://www.who.int/medicines) 1. National Drug Policy guide to coordination of action by all stakeholders 2. Access selection, financing, pricing, supply systems 3. Quality and safety standards, effective regulation, information support 4. Rational use health professionals and consumers, public and private WHO - EDM 3 What is WHO doing in order to reduce quality and safety, and in general regulatory gaps? Supporting capacity building and training of regulators Issuing norms and standards Preparing guidance materials How to fight counterfeit drugs How to register generic drugs How to set up pharmacovigilance centers Preparing training materials Quality Assurance, vol. 1 and 2; TRS publications Validated GMP training modules on CD-rom GCP training modules under creation ... Facilitating information exchange WHO Drug Information, WHO Pharmaceutical Newsletter, Rapid Alerts, increasing information on the web site Biennial International Conferences of Drug Regulatory Authorities (ICDRAs) Annual meetings of National Pharmacovigilance Centers WHO - EDM 4 History of drug safety (1) 2002 - 154 years of pharmacovigilance 29.01.1848 15 year old Hannah Greener died in course of routine anaesthesia with chloroform (problem: ingrown nail of toe; fibrillation of ventricles?). Lancet’i initiated foundation of a commission and starting collection of notifications about side effects (1893) 1906 - US Federal Food and Drug Act (required, that the pharmaceuticals should be “pure” and “free of any contamination”, nothing was said about the efficacy) 1936 - USA-s 107 lethal cases (diethylenglycol was used to solubilize sulphanilamides); the law was amended in 1938 WHO - EDM 5 History of drug safety (2): after thalidomide era 6 1961 - Dr William McBride (Australia) reported 20% increase in foetal abnormalities and significant increase of phocomelia in relation with thalidomide use, later numerous reports from other countries (more than 4000 cases) 1962 - USA Kefauver-Harrise amendment to the law (requirement to prove safety and efficacy before issuing MA) 1963 - resolution WHA 16.36 reaffirmed the need for early action in regard to adverse drug reactions 1964 - UK started “yellow cards” system 1965 - European Union issued EC Directive 65/65 1968 - start of WHO Programme for International Drug Monitoring 1990 - ICH - elaboration of intra-regional requirements for safety starts WHO - EDM Drug Safety: some definitions (1) Adverse event/adverse experience - Any untoward medical occurrence that may present during treatment with a pharmaceutical product but which does not necessarily have a causal relationship with this treatment Side effect - Any unintended effect of a pharmaceutical product occurring at doses normally used in man, which is related to the pharmacological proprieties of the drug Essential elements of this definition are the pharmacological nature of the effect, that the phenomenon is unintended, and that there is no overt overdose WHO - EDM 7 Drug Safety: some definitions (2) Adverse reaction - A response to a drug which is noxious and unintended, and which occurs at doses normally used in man for the prophylaxis, diagnosis, or therapy of disease, or for modification of physiological function (WHO Technical Report No 498, 1972, ICH definition regarding marketed products practically the same) Pharmacovigilance is a science and activities relating to the detection, assessment, understanding and prevention of adverse effects or any other possible drug-related problems. WHO - EDM 8 Drug Safety: some definitions (3) Signal - Reported information on a possible causal relationship between an adverse event and a drug, the relationship being unknown or incompletely documented previously. Usually more than a single report is required to generate a signal, depending upon the seriousness of the event and the quality of the information WHO - EDM 9 How do we get information on drug safety? Main sources of information: Pre-clinical studies Clinical studies pre- and post-marketing Spontaneous adverse reaction reporting* national and international Epidemiological studies case-control cohort Data collected for other purposes routine statistics databases of prescription and outcomes WHO - EDM 10 Limitations of Pre-approval Clinical Trials Size (maximum 3,000-5,000 subjects) Sometimes larger for vaccine Narrow Population Often does not include special groups (e.g., children, elderly) Narrow indications not covering actual evolving uses in practice Short Duration (1-3 years) Latent effects not directly measured WHO - EDM 11 The Likelihood of Observing an Adverse Drug Reaction Employing Numbers Usually Studied in Premarketing Trials Number of Patients 2,000 Threshold for ADR Probability 1 / 500 (Lymphoma From Azathioprine) 0.98 1 / 1,000 (Eye Damage From Practolol) 0.86 1 / 10,000 (Anaphylaxis From Penicillin) 0.18 1 / 50,000 (Aplastic Anemia From Chloramphenicol) 0.04 WHO - EDM 12 How many patients one needs to treat to see with high probability the reaction? Pre-marketing studies are carried out in limited number of patients: “The law of three” In order to detect for sure SAE that occurs as 1 event per 2000 patients treated we need to treat 6000 patients for 1 case 9600 patients for 2 cases 13 000 patients for 3 cases The number of patients involved in pre-marketing studies has been increasing but is still limited in comparison with the exposure to the drug in post-marketing phase WHO - EDM 13 Are drugs safer today ? (1) During 1960-1999 there were 121 safety related withdrawals Worldwide Market life was known for 87 of those Market life less than 2 years 31% Market life less than 5 years 50% Fung et al. Drug Information Journal, 2001; 35:293-317 During 1972-1994 in 583 new active substances were approved Of these 59 were withdrawn later During 1990-2001 in UK 24 drugs were withdrawn due to safety reasons WHO - EDM 14 Are drugs safer today? (2) In England and Wales the number of deaths related to ADRs has raised during last 10 years Study of 3,277 Coroner’s Inquests in one UK district showed during 1986-1991 10 deaths due to prescribing errors and 36 due to ADRs These 46 deaths made approximately 1 in 2000 A meta-analysis of 39 prospective studies in USA ADRs between fourth and sixth leading cause of death in USA; fatality rate as a result of ADRs was estimated 0.32% among hospitalised patients The annual cost of ADR related hospital costs 1.6-4 billion US $ 15 Ferner et al. J R Soc Med, 1994;87:145-148 Lazarou et al. JAMA, 1998;279:1200-1205 WHO - EDM The cost of adverse drug events: estimated lost patient activity days per year in hospitalised patients Country Serious ADRs Lost Activity Days US Germany UK Australia Sweden 700,000 206,000 148,000 48,000 22,000 1,218,000 358,440 257,520 83,520 38,280 WHO - EDM 16 WHO Collaborating Centre called Uppsala Monitoring Centre (UMC): operational arm of WHO Drug Monitoring Programme Established in 1978 as Swedish Foundation Based on agreement between Swedish Government and World Health Organization Originally financial contributions from Sweden, selffinancing today Formerly Swedish administrative board, international board today (3 of 6 members nominated by WHO) WHO headquarters responsible for policy WHO - EDM 17 From pilot to permanence: Countries participating in the WHO Programme 2002 Member countries Associate member countries 18 (68) (7) WHO - EDM Uppsala Monitoring Centre (UMC): major resource for WHO pharmacovigilance related activities 19 Major areas of work - cooperation and support to national centres Collection and processing of case reports of ADRs Data utilization (3 million reports in database) Information exchange and feedback Education, training and advise Harmonization Research and evaluation Main function Signal generation (identification of previously unknown adverse drug reactions) and communication WHO - EDM Uppsala Monitoring Centre (UMC): major recent achievements New innovative tools A sophisticated Bayesian confidence propagation neural network (BCPNN) programme (1998), which partly automates the signal detection, provides earlier signals But effectiveness depends on Size of database Quality of reports Timeliness of reporting Active and reliable reporting culture WHO - EDM 20 Recent trends: enlarging the scope of pharmacovigilance Pharmacovigilance concerns have been widened to include: herbal medicines traditional and complementary medicines blood products biologicals vaccines medical devices WHO - EDM 21 World Health Assembly resolution 54.11, 21 May 2001: WHO Medicines Strategy … bearing in mind the previous report on the subject, that highlight challenges related to the international trade agreements, access to essential drugs, drug quality and rational use of medicines, together with the urgent need to improve access to treating priority health problems such as malaria, childhood illnesses, HIV/AIDS and tuberculosis, among others; REQUESTS Director-General: … (3) to provide support for implementation of drug monitoring systems in order better to identify developing resistance, adverse reactions and misuse of drugs within health systems, thus promoting rational use of drugs; (6) to provide support to Member States to set up efficient national regulatory mechanisms for quality assurance that will help ensure compliance with good manufacturing practices, bioavailability and bioequivalence WHO - EDM 22 World Health Assembly resolution, May 2002: Quality of Care: Patient Safety … Concerned that the incidence of adverse events is a challenge to quality of care, a significant avoidable cause of human suffering, and high toll in financial loss and opportunity cost to health services; Noting that significant enhancement of health systems’ performance can be achieved … by preventing adverse events in particular, and improving patient safety and health care quality in general; REQUESTS Director-General: … (1) to develop global norms, standards and guidelines for the definition, measurement and reporting of adverse events..., and to provide support to countries in developing reporting systems, taking preventive action … ; (2) to promote framing of evidence-based policies, including global standards that will improve patient care, with particular emphasis on such aspects as product safety, safe clinical practice … and safe use of medicinal products and medical devices, and creation of a culture of safety within health care organizations. WHO - EDM 23 What is WHO doing to follow the recommendations by the World Health Assembly? Publications published and under preparation. - Safety Monitoring of Medicinal Products - Guidelines for Setting Up and Running a Pharmacovigilance Centre (2000) - The Importance of Pharmacovigilance (2002) - Safety of Medicines - A Guide to Detecting and Reporting of Adverse Drug Reactions. Why Health Professionals Need to Take Action (2002) http://www.who.int/medicines/library/qsm/who-edm-qsm2002-2/esd_safety.pdf - Safety Monitoring of Medicinal Products in Communities (first draft) - Safety Monitoring of Herbal Medicines (process started) WHO - EDM 24 A Future challenges: safety of drugs for neglected diseases (1) Research and developemnt for neglected diseases intensifying Problems with regulatory assessment - who does it? Launch in places where no monitoring, no health systems, no health care professionals All drugs immediately OTC No incentive for post-marketing studies No ... More responsibility and care needed that in case of launching in developed markets! Regulatory guidance/requirements missing 25 How to ensure drug safety in communities affected by neglected diseases? WHO - EDM A Future challenges: improvement of existing systems (3) Are existing systems exhausted? Likely improvement of spontaneous reporting by medical doctors can enable more early signal detection Can patients and pharmacists reporting improve patients safety? Initiatives of creating data bases of patient reports Pharmacists based reporting Regulatory guidance in which cases new/alternative methods have to be imposed WHO - EDM 26 A Future challenges: improvement of information, education and communication (4) Improvement of information In many parts of the World information is either not readily available or of poor quality In some countries still only OTC drugs have PIL although both POM and OTC are delivered without prescription Education Can education of consumers/patients improve drug safety? Communication Health professionals Patients Media WHO - EDM 27