Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
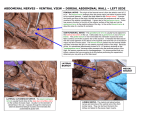
n Feature Article Saphenous and Infrapatellar Nerves at the Adductor Canal: Anatomy and Implications in Regional Anesthesia Sofia Anagnostopoulou, MD; George Anagnostis, MD; Theodosios Saranteas, MD; Andreas F. Mavrogenis, MD; Tilemachos Paraskeuopoulos, MD abstract Conflicting data exist regarding the anatomical relationship of the saphenous and infrapatellar nerves at the adductor canal and the location of the superior foramen of the canal. Therefore, the authors performed a cadaveric study to detail the relationship and course of the saphenous and infrapatellar nerves and the level of the superior foramen of the canal. The adductor canal and subsartorial compartment were dissected in 17 human cadavers. The distance between the superior foramen of the canal and the mid-distance (MD) between the base of the patella and the anterior superior iliac crest were measured; the course of the saphenous and infrapatellar nerves and the level of origin of the infrapatellar branch were detailed. In 13 of 17 specimens, the superior foramen of the adductor canal was distal to the MD (mean, 6.5 cm); in the remaining specimens, it was proximal to the MD. In 12 of 17 specimens, the infrapatellar branch exited the canal separately from the saphenous nerve; in the remaining specimens, it originated caudally to the canal. In all dissections, the infrapatellar branch had a constant course in close proximity to the saphenous nerve within the canal and between the sartorious muscle and femoral artery caudally to the canal. Most commonly, the superior foramen of the adductor canal is located caudally to the MD; the infrapatellar branch originates from the saphenous nerve within the canal and has a constant course in close proximity to the saphenous nerve. These observations should be considered for regional anesthesia techniques at the adductor canal. [Orthopedics. 2016; 39(2):e259-e262.] T he adductor, subsartorial, or Hunter’s canal is an aponeurotic intermuscular tunnel in the middle third of the thigh. It extends from the apex of the femoral triangle to the adductor hiatus. Its boundaries include the sarto- MARCH/APRIL 2016 | Volume 39 • Number 2 rius anteriorly, the adductor longus and adductor magnus posteromedially, and the vastus medialis laterally. The canal contains the femoral artery, femoral vein, and branches of the femoral nerve, more specifically the saphenous nerve and the nerve to the vastus medialis. The saphenous nerve passes beneath the sartorius and lies in front of the artery, behind the aponeurotic covering of the adductor canal, as far as the opening in the lower part of the adductor magnus, where it emerges from behind the lower edge of the aponeurotic covering of the canal.1,2 The infrapatellar branch is the largest branch of the saphenous nerve; it pierces the sartorius and fascia lata and is distributed to the skin in front of the patella.3 Anatomical studies have shown that the distribution of the infrapatellar branch demonstrates significant variability.3-9 This nerve communicates above the knee with the anterior cutaneous branches of the femoral nerve and/or the obturator nerve,8 below the knee with other branches of the The authors are from the Department of Anatomy (SA, GA, TP), the Department of Anesthesiology (TS), and the First Department of Orthopaedics (AFM), National and Kapodistrian University of Athens, School of Medicine, Athens, Greece. The authors have no relevant financial relationships to disclose. Correspondence should be addressed to: Sofia Anagnostopoulou, MD, Department of Anatomy, National and Kapodistrian University of Athens, School of Medicine, 75 Mikras Assias Str, 11527 Goudi, Athens, Greece ([email protected]). Received: April 8, 2015; Accepted: July 6, 2015. doi: 10.3928/01477447-20160129-03 e259 n Feature Article B A saphenous nerve, and on the lateral side of the joint with branches of the lateral femoral cutaneous nerve, forming the plexus patellae.5-8 As yet, the exact anatomical relationship between the adductor canal and the region where the saphenous nerve gives off the infrapatellar branch has not been described. In addition, conflicting data exist concerning the exact anatomic level of the superior foramina of the adductor canal.10,11 The current authors performed this cadaveric study to describe the anatomical relationship of the saphenous nerve and its infrapatellar branch at the level of the adductor canal and to precisely delineate the anatomic area that the infrapatellar branch separates from the main trunk of the saphenous nerve. Possible implications for regional anesthesia techniques are also analyzed. Materials and Methods Seventeen lower extremities from 11 adult human formalin-embalmed cadavers (mean age, 71±11 years; male/female ratio, 4/7) were dissected at the anatomy department of the authors’ institution. Approval for this study (No. 1056; 27-92010) was provided by the Committee of the Medical School of the University of Athens, Athens, Greece. Cadavers were in the legal custody of the Department of Anatomy at the Medical School of the University of Athens, Athens, Greece. All e260 Figure 1: Illustration showing the medial anatomy of the thigh and the adductor canal. Abbreviations: a, artery; m, muscle; n, nerve; v, vein (A). Diagram showing the branching of the saphenous nerve. Abbreviations: I, infrapatellar branch; S, saphenous nerve (B). cadavers were donated for teaching and research purposes. Each cadaver was placed in the supine position with the legs abducted. The skin and subcutaneous tissues of the anterior and medial thigh from the level of the inguinal ligament to the level of the medial tibial condyle were carefully excised to expose the sartorious and vastus medialis muscles. The sartorious muscle was meticulously prepared and reflected so that the adductor canal and the subsartorial compartment were clearly exposed and dissected (Figure 1A). The mid-distance (MD) between the base of the patella and the anterior superior iliac crest was determined in each specimen. The distance between the superior foramen of the adductor canal and the MD was also measured. The course of the saphenous nerve from its origin from the femoral nerve to the level of the medial epicondyle of the femur was detailed, and the anatomical level of the origin of the infrapatellar branch was also specified (Figure 1B). The anatomical course, distribution, and variations of the infrapatellar branch were recorded. Results In 4 (23%) of the 17 specimens, the superior foramen of the adductor canal was proximal to the MD. In 13 (77%) of the 17 specimens, the superior foramen of the adductor canal was distal to the MD, with the mean distance between the superior foramen of the adductor canal being 6.5 cm (range, 1.8-10 cm). In 12 (70.6%) of the 17 specimens, the infrapatellar branch of the saphenous nerve exited the adductor canal separately from the saphenous nerve. In 4 (33%) of these 12 specimens, the infrapatellar branch of the saphenous nerve separated the main trunk of the saphenous nerve before the superior foramen of the adductor canal, remaining caudal to the MD (Figure 2); in 8 (67%) of these 12 specimens, the infrapatellar branch of the saphenous nerve separated the main trunk of the saphenous nerve within the adductor canal. In 4 (23.5%) of the 17 specimens, the infrapatellar branch originated from the saphenous nerve after the latter had exited the adductor canal, where the nerve passed between the sartorious muscle and the femoral artery. In 1 (5.9%) of the 17 specimens, the infrapatellar branch originated from the saphenous nerve after the latter had pierced the sartorious muscle (Figure 3). In all anatomical dissections, the infrapatellar branch was always in close proximity to the saphenous nerve; from its origin to the inferior foramen of the adductor canal, the infrapatellar branch passed beneath the sartorius, in front of the femoral artery, behind the aponeurotic covering of the canal. In all specimens, caudally to the inferior foramen of the adductor canal, the infrapatellar branch had a constant anatomical course; the nerve passed between the sartorious muscle and the femoral artery and was distributed to the skin in front of the patella. Discussion Previous anatomical studies have reported various origins of the infrapatellar branch from the saphenous nerve and its distribution to the skin in front of the patella.3-8 The exact anatomical relationship of the infrapatellar branch within the adductor canal and the anatomical area where the nerve originates and separates from the saphenous nerve has not been Copyright © SLACK Incorporated n Feature Article documented. Some authors have reported that the infrapatellar branch originates most commonly from the saphenous nerve in the middle third of the thigh.5 A previous anatomical study5 reported that the infrapatellar branch of the saphenous nerve originated from the main trunk of the saphenous nerve in the proximal third of the thigh in 17.6% of anatomical specimens, the middle third in 58.8%, and the distal third in 23.5%.5 Similar imaging studies clearly identified the infrapatellar branch using ultrasound; however, they did not confirm the exact anatomical area of its origin from the saphenous nerve.11-13 Moreover, there are no published studies that examine the nerve block of the saphenous and infrapatellar branch, either cephalad or caudal to the adductor canal. Conflicting data also exist regarding the anatomic level whereby proper needle insertion can result in successful adductor canal block. Jæger et al11 advocated placing the needle for adductor canal saphenous/infrapatellar nerve block in the MD between the anterior superior iliac spine and the base of the patella, whereas others supported a more distal placement of the needle.10 Recently, a clinical study reported successful nerve block of both the saphenous nerve and the infrapatellar branch using subsartorial ultrasoundguided local anesthetic injection within the adductor canal.14 These observations and conflicting reports have important implications for regional anesthesia nerve block techniques at the anatomic region of the adductor canal. In the current anatomical study of human cadavers, the infrapatellar branch of the saphenous nerve most commonly separated the main trunk of the saphenous nerve within the adductor canal. In addition, once the main trunk of the saphenous nerve divided prior to the superior foramen of the adductor canal, the 2 nerves entered together within the adductor canal. During dissection, the infrapatellar branch, either as a part of the main trunk of the saphenous nerve or as a separate branch, always MARCH/APRIL 2016 | Volume 39 • Number 2 Figure 2: The adductor canal has been dissected to reveal the anatomical relationship of the saphenous nerve (S) and infrapatellar branch (I). The infrapatellar branch separates from the main trunk of the saphenous nerve cephalad to the superior foramen of the adductor canal. Both nerves exit independently from the inferior foramen of the canal. Abbreviations: F, femoral artery; T, tendon of the adductor magnus; V, vastoadductors membrane. coursed beneath the sartorious muscle in close proximity to the saphenous nerve within the adductor canal. Therefore, in the clinical setting of adductor canal nerve block, irrespective of the level of origin of the infrapatellar branch from the saphenous nerve, subsartorial injection of local anesthetic will likely lead to successful nerve block of both the saphenous nerve and the infrapatellar branch. The adductor canal nerve block occurs more distally with respect to femoral nerve block and therefore covers a smaller area of the leg. Previous research demonstrated that adductor canal blocks are effective in providing analgesia after knee surgery and can spare function of the quadriceps.11 Doses as high as 8 mL of local anesthetic can lead to sufficient blockade of the saphenous nerve in the adductor canal, whereas lower volumes of local anesthetic (5 mL)15 have been proven less effective.16 Although the literature confirms the significance of this block in clinical practice, questions remain regarding the exact anatomic region where this block must be implemented.11,15,16 Therefore, the insertion point of the needle for adductor canal nerve block is also clinically important for the accurate implementation of adductor canal nerve block. According to the authors’ observations, the infrapatellar branch always originated from the saphenous Figure 3: The sartorious muscle has been dissected to show the exit of the saphenous nerve (S) and the femoral artery (F) from the inferior foramen of the adductor canal (AC). The saphenous nerve pierces the sartorious muscle, and then the infrapatellar branch (I) originates. nerve caudal to the MD, whereas in most cases the MD was always cephalad to the superior foramen of the adductor canal. Based on these observations, the adductor canal block by Jæger et al11 is mainly a subsartorial saphenous nerve block out of the canal, whereas an accurate adductor canal block is that described by Manickam et al.14 Importantly, comparison of the 2 techniques, either on infrapatellar or saphenous nerve blocks, has not yet been performed. Fresh-frozen cadavers were not used in the current study; this may be considered a limitation. The authors acknowledge that the type of preservation directly affects the biomechanical properties of tissues. Frozen cadavers are frozen and stored at subzero temperatures, approximately -20°C. Embalmed cadavers are preserved with embalming chemical compounds, including preservatives, sanitizers, disinfectant agents, and additives, used to temporarily delay the decomposition process from anaerobic bacteria. Embalming agents are administered to the cadaveric body mainly through the femoral or carotid artery. Frozen cadavers provide betterquality tissues for teaching in surgical specialties. Formalin-embalmed cadavers are considered the method of choice in dissection anatomy. Conclusion The infrapatellar branch of the saphenous nerve most commonly originates e261 n Feature Article from the saphenous nerve within the adductor canal; the superior foramen of the adductor canal is mainly caudal to the MD between the base of the patella and the superior iliac crest, and the infrapatellar branch has a constant course in close proximity to the saphenous nerve within the adductor canal. These observations should be kept in mind for accurate and successful saphenous/infrapatellar nerve block at the level of the adductor canal. References 1. Saranteas T, Anagnostis G, Paraskeuopoulos T, et al. Anatomy and clinical implications of the ultrasound-guided subsartorial saphenous nerve block. Reg Anesth Pain Med. 2011; 36(4):399-402. 2. Gosling JA, Harris PF, Whitmore I, Willan P. Medial compartment of the thigh. In: Gosling JA, Harris PF, Whitmore I, Willan P, eds. Human Anatomy Color Atlas and Text. 4th ed. Philadelphia, PA: Mosby Elsevier; 2002:234236. 3. Ebraheim NA, Mekhail AO. The infrapatellar branch of the saphenous nerve: an anatomic e262 study. J Orthop Trauma. 1997; 11(3):195-199. 4. Arthornthurasook A, Gaew-Im K. Study of the infrapatellar nerve. Am J Sports Med. 1988; 16(1):57-59. 5. Horner G, Dellon AL. Innervation of the human knee joint and implications for surgery. Clin Orthop Relat Res. 1994; 301:221-226. 6. Arthornthurasook, A, Gaew-Im K. The sartorial nerve: its relationship to the medial aspect of the knee. Am J Sports Med. 1990; 18(1):41-42. 7. Tubbs RS, Loukas M, Shoja MM, Apaydin N, Oakes WJ, Salter EG. Anatomy and potential clinical significance of the vastoadductors membrane. Surg Radiol Anat. 2007; 29(7):569-573. 8.Purner J. Peripheral course of saphenous nerve [in German]. Anat Anz. 1971; 129(2):114-132. 9. Marhofer P, Harrop-Griffiths W, Kettner SC, Kirchmair L. Fifteen years of ultrasound guidance in regional anaesthesia: part 1. Br J Anaesth. 2010; 104(5):538-546. 10.Bendtsen TF, Moriggl B, Chan V, Peder sen EM, Børglum J. Defining adductor canal block. Reg Anesth Pain Med. 2014; 39(3):253-254. 11. Jæger P, Zaric D, Fomsgaard JS, et al. Adductor canal block versus femoral nerve block for analgesia after total knee arthroplasty: a randomized, double-blind study. Reg Anesth Pain Med. 2013; 38(6):526-532. 12. Le Corroller T, Lagier A, Pirro N, Champsaur P. Anatomical study of the infrapatellar branch of the saphenous nerve using ultrasonography. Muscle Nerve. 2011; 44(1):50-54. 13. Lundblad M, Kapral S, Marhofer P, Lön nqvist PA. Ultrasound-guided infrapatellar nerve block in human volunteers: description of a novel technique. Br J Anaesth. 2006; 97(5):710-714. 14. Manickam B, Perlas A, Duggan E, Brull R, Chan VW, Ramlogan R. Feasibility and efficacy of ultrasound-guided block of the saphenous nerve in the adductor canal. Reg Anesth Pain Med. 2009; 34(6):578-580. 15. Head SJ, Leung RC, Hackman GP, Seib R, Rondi K, Schwarz SK. Ultrasound-guided saphenous nerve block—within versus distal to the adductor canal: a proof-ofprinciple randomized trial. Can J Anaesth. 2015; 62(1):37-44. 16. Adoni A, Paraskeuopoulos T, Saranteas T, Sidiropoulou T, Mastrokalos D, Kostopanagiotou G. Prospective randomized comparison between ultrasound-guided saphenous nerve block within and distal to the adductor canal with low volume of local anesthetic. J Anaesthesiol Clin Pharmacol. 2014; 30(3):378-382. Copyright © SLACK Incorporated