Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
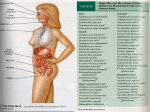
U N D E R S TA N D I N G M I C R O B E S Committee Report: Emerging pathogens — viruses, protozoa, and algal toxins Water utility managers will need to know important issues about microbes of concern in drinking water. AWWA Research Division Microbiological Contaminants Research Committee A coordinated effort is needed to deal with emerging pathogens in drinking water so that water utilities and regulators alike can develop a response plan.1 This plan must assess what is known as well as gaps in information about potential pathogens so that microbial and chemical risks can be balThe American Water Works Association Research Division anced.2,3 In 1995, a group Microbial Contaminant Committee reviewed three viral and three of experts was convened protozoan microorganisms and one set of bacterial toxins of by the International Life greatest concern to the water industry: enterovirus, calicivirus Sciences Institute, the US and Norwalk virus, and hepatitis; Cyclospora cayetanensis, Environmental Protection microsporidia, and Toxoplasma gondii; and cyanobacterial toxins. Agency, and the AWWA To help the water quality specialist, this report describes the Research Foundation to virus, protozoan, or toxin; reviews its health effects; summarizes develop a general frameinformation on its occurrence, waterborne outbreaks, and water work for assessing the risk treatment; discusses analytical procedures; and outlines needed research. For executive summary, see page 191. 110 VOLUME 91, ISSUE 9 © 1999 American Water Works Association, Journal AWWA September 1999 JOURNAL AWWA Water suppliers are familiar with the protozoa Giardia lamblia and Cryptosporidium parvum (left) but may want to learn more about Toxoplasma (below)—a protozoan parasite that can be waterborne and that occurs worldwide. of human disease following exposure to pathogens.4 eter; they replicate in the cytoplasm of host cells, and In 1996, the AWWA Research Division Microbial they resist both high and low pH. Contaminant Committee polled its members and then Health effects. Human enteroviruses cause a varifocused on four bacterial, three viral, and three pro- ety of clinical illnesses ranging from paralytic tozoan microorganisms and one set of bacterial tox- poliomyelitis, myocarditis (heart infection), and diains of greatest concern to the water industry. betes to the common cold. Poliomyelitis (“polio”) has The first part of this report reviewed bacterial been known since ancient times, but it was a major pathogens in water and provided a model for assessconcern in the earlier part of the twentieth century ing the risk of microbes in water.5 This article reviews as epidemics (primarily afflicting young children) other organic contaminants: the caliciviruses and specifically Norwalk virus, enterovirus, and hepatitis virus; the he 1990s can be characterized as the protozoa Cyclospora cayetanensis, microsporidia, and Toxodecade of the microbe. plasma gondii; and cyanobacteria toxins (Table 1). The committee has provided an assessment of risk for became common during the summer and fall. The these microorganisms and toxins by characterizing virus can cause permanent nerve damage that paratheir occurrence and concentration in water, their lyzes the arms, legs, or lungs. Most symptomatic infecsusceptibility to treatment, and their health effects. For tions result only in influenzalike or respiratory illeach contaminant investigated, the following report ness. Because of the development of poliovirus vaccine contains a brief overview, a summary of outstandand large-scale vaccination programs, paralytic ing issues, and access to the relevant literature. Al- poliomyelitis has been absent from the Western Hemithough some would debate whether the organisms sphere for the past five years. Coxsackievirus and listed are emerging pathogens (as opposed to microbes echoviruses are now recognized as a leading cause already recognized as pathogens), the committee’s of acute fevers among young children and infants objective was to highlight organisms that might not and, in developed countries, as the most common be well known to water utility personnel. cause of aseptic meningitis.6 The mortality rate in more severe illnesses (meningitis, myocarditis, paraViruses lytic disease) ranges from 0.01 to 0.9 percent. Enteroviruses. Description. The enteroviruses Occurrence, survival, and outbreaks. Enteroviruses form a genus of the Picornaviridae family that are may be transmitted by either the fecal–oral route or among the smallest ribonucleic acid (RNA) viruses— the respiratory route. One route may predominate, thus the name “pico (small) RNA virus.” Human depending on the serotype. All enteroviruses (except, enteroviruses are divided into four groups: poliovirus possibly, enterovirus type 70) are believed to be capa(three types), coxsackievirus (30 types), echovirus ble of fecal–oral transmission. Enterovirus type 70, (34 types), and enterovirus (68–71 types). They are which causes eye infections, may be transmitted only all nonenveloped, icosahedral, and 25–30 nm in diam- by direct contact with contaminated hands or other T SEPTEMBER 1999 © 1999 American Water Works Association, Journal AWWA September 1999 COMMITTEE REPORT 111 they may not all grow in the same cell line. Enteroviruses are usually isolated from water or other environmental samples by the production AWWA Microbiological US Environmental Protection of CPE in the buffalo green Category Contaminants Research Committee Agency (Contaminant Candidate) 5 monkey kidney cell line. Viruses Enteroviruses Caliciviruses Many of the enteroviruses Norwalk virus/Calicivirus Echoviruses can also be isolated by the Hepatitis viruses Coxsackieviruses Adenoviruses plaque-forming unit method. Protozoa Cyclospora cayetanensis Microsporidia In addition, molecular techMicrosporidia Toxoplasma gondii niques such as polymerase Toxins Cyanobacteria toxins Cyanobacteria toxins chain reaction (PCR) have Acanthamoeba been used to detect enteroviruses in water samples. Water treatment. Conventional water treatment objects (fomites). Most transmission is believed to be with disinfection removes essentially all (99.99 perperson-to-person. Common-source outbreaks of coxcent or more) enterovirus. Coxsackievirus appears sackievirus and echoviruses that originated in water to be more resistant to ultraviolet light disinfection or food have been documented. than the other enteroviruses. The concentration of enteroviruses in raw sewage Research needs. The Information Collection Rule12 has been reported to vary from a few hundred to will provide important information on the occur> 100,000/L. In 279 raw surface water samples and rence of culturable enteroviruses in surface water 260 untreated groundwater samples assayed by cell used for large (>100,000 population) water systems. culture, 25 and 8.1 percent, respectively, were posi- Data are needed for other surface water and groundtive for enteroviruses.7 With the exception of polio- water systems. How viruses avoid treatment barrivirus, coxsackieviruses are the enteric viruses that ers and contaminate distribution system water should have been most commonly isolated from water, even be investigated. Additional disinfection data are treated drinking water. Enteroviruses may not be needed under real-world conditions. Simple methods completely removed by domestic sewage treatment, using PCR should be developed for use in water utilincluding disinfection as normally practiced, and they ity laboratories. can usually be isolated. Enteroviruses have been isoCalicivirus and Norwalk virus. Description. The lated in almost any environment that has been caliciviruses are members of the viral genus caliexposed to human fecal contamination—surface water civirus, two of which are characteristically associated and groundwater, marine water and sediments, shellwith humans. The first, human calicivirus, contains fish, crabs, crops irrigated with sewage, domestic solid five recognized strains (Norwalk virus, and Hawaii, waste, soil, aerosols, and fields spray-irrigated with Taunton, Snow Mountain, and Southampton strains) sewage water. and others whose common names are not yet officially The survival of enteroviruses and other enteric recognized. The second is hepatitis E virus. Other viruses depends on many factors, including tem- caliciviruses are associated with infections in mammals perature, sewage pollution, microbial activity, and other than humans. adsorption to solids (clays and sediments). Generally, Health effects. The classic calicivirus illness typically the lower the temperature, the longer the survival affects infants aged 1–24 months. However, calicivirus time. Below 5 oC, enteroviruses may survive for infections and illnesses occur in all age groups. Geriyears in the environment. They are stable at pH 3–5 atric outbreaks are characterized by diarrhea averfor 1–3 hours and can tolerate pH 10–11 for sev- aging four days (range 1–11 days). The incubation eral minutes. period before diarrhea is 48–72 hours. Norwalk virus Several reports have attributed poliovirus out- and Norwalk-like caliciviral strains typically act faster; breaks to contaminated drinking water, although the incubation takes 24–48 hours and symptoms last studies were not conclusive.8 Coxsackieviruses have 12–60 hours. Norwalk or Norwalk-like illness typically been associated with two recreational outbreaks,9,10 produces vomiting in children but diarrhea in adults. and an epidemiological study of bathers in surface It is estimated that 40 percent of the outbreaks of water found a significant increased risk of enterovi- gastroenteritis in adults can be attributed to the Norral infection in children.11 Although enteroviruses walk and Norwalk-like viruses.13 Other symptoms have been isolated from water during waterborne associated with human caliciviruses include abdomdisease outbreaks associated with drinking water, epiinal pain, cramping, low fever, headache, nausea, demiological investigations are lacking. tiredness (malaise), and muscle pain (myalgia). These Analytical methods. All enteroviruses can be grown diseases may be severe and prolonged in immunoin primate or human animal cell cultures with the logically debilitated and elderly patients, but death production of cytopathogenic effects (CPE), although is unlikely if supportive care is available. TABLE 1 112 Viral, protozoan, and other contaminants of concern proposed by AWWA Microbiological Contaminants Research Committee and US Environmental Protection Agency VOLUME 91, ISSUE 9 © 1999 American Water Works Association, Journal AWWA September 1999 JOURNAL AWWA Norwalk virus (left), a member of the viral genus calicivirus (right), is believed to be the cause of 40 percent of the outbreaks of gastroenteritis in adults. Research needs. A quantitative cell culture techHepatitis E virus has an incubation period of 2–8 nique must be developed for assaying the infectivity weeks. Children typically do not show symptoms (their infection is subclinical), although in adults of these viruses. Such a technique will enable the jaundice can persist for many weeks. Mortality caused gathering of better disinfection data and better analyby hepatitis E in the general population is 0.1–4 persis of other water treatment processes. cent,14 but for pregnant women in the third trimester Hepatitis A virus. Description. Hepatitis A virus it can be > 20 percent.13,14 The virus appears to be (HAV) is a small (27-nm diameter), nonenveloped similar to one that causes illness in domesticated picornavirus containing a single-stranded RNA molpigs. At present no antimicrobial therapies effececule. It is a cause of acute infectious hepatitis and was tively treat human calithe first enteric virus to be civiral diseases. associated with a waterOccurrence, survival, borne disease outbreak in and outbreaks. Human the United States.16 HAV caliciviruses and hepatitis is the predominant cause E virus are transmitted of infectious hepatitis in even viral, protozoan, by ingestion of contamithe United States; about nated surface water or 25,000 cases are reported and algal toxin groundwater, ice, conannually. 17 The true pathogens that cause taminated shellfish, or by annual incidence may be swimming in sewagehigher by a factor of two waterborne illness contaminated water.14,15 to ten. are profiled. Outbreaks of human caliHealth effects. More civiruses can occur year than half of the United round, and the incidence States population older increases somewhat during winter months. Illness than 40 years has serum antibody to HAV.18 It is of caused by hepatitis E virus tends to peak in the concern as a cause of gastroenteritis because its sympautumn in temperate areas of the world; it peaks toms are among the most serious of those caused by during floods caused by the rainy season in tropical enteric viruses, and it has a mortality rate of about 0.1 or monsoon areas.13 percent. HAV infects liver cells, causing inflammaAnalytical methods. The human caliciviruses tion, cell damage, and cell death. Symptoms begin currently cannot be cultured in vitro using animal four to six weeks after infection and include fever, tissues or animal cell lines. Therefore, it is necessary nausea, loss of appetite (anorexia), and tiredness, often with mild diarrhea, followed shortly by jaundice to use detection techniques that do not provide in(yellowness of skin). Asymptomatic infection is comformation regarding viral infectivity. These techmon in children. Symptoms usually last one to two niques include visual detection by transmission weeks but may persist for several months. electron microscopy; enzyme-linked immunosorOccurrence, survival, and outbreaks. HAV is transbent assay, which detects viral proteins; and reverse transcriptase–polymerase chain reaction, which mitted by the fecal–oral route, and transmission by fecally contaminated water and food is documented,19 detects viral RNA. Water treatment. Little is known about how effecbut person-to-person transmission is much more comtively water treatment physically removes or inacti- mon. Waterborne transmission of the virus has been vates these viruses, although some work is in progress. reported by a number of investigators. The virus sur- S SEPTEMBER 1999 © 1999 American Water Works Association, Journal AWWA September 1999 COMMITTEE REPORT 113 Cyclospora cayetanensis was proposed28 for the species infecting humans on the basis of Attribute Cryptosporidium parvum Cyclospora cayetanensis sporulation and excystation studies conducted in vitro; Oocyst 4–6-µm spheres are Autofluorescent spheres, 8–10immediately infectious µm diameter, require five- to however, others have ques10-day sporulation to be tioned this species name.27,29 infectious; sporulation is Cyclospora spp. are obligate temperature-dependent. Animal hosts Cross transmissible among most Documented only in humans and intracellular parasites characmammals various nonhuman primates terized with other coccidia, Disease Acute self-limiting diarrhea More prolonged diarrhea with such as Isospora and ToxoNo effective drug treatment bouts of relapse Treatable by co-trimaxazole plasma, because they are inWaterborne 10 in North America, 1985–95 Chicago, 199094 and Nepal, testinal spore- (oocyst-) formoutbreaks 1994102 ing protozoa. 28 Molecular analysis of Cyclospora has suggested that it is closely related vives more than four months at both 5 and 25oC in to Eimeria species.30 Similar oocysts have been found water, wastewater, and sediments.16 However, at 25oC, in nonhuman primates in East Africa,29,31 and the HAV generally survived longer than poliovirus and possibility of transmission from other animals to echovirus, regardless of soil and water quality.20 Stud- humans has been raised. ies suggest that HAV survives for relatively long periCyclospora completes its life cycle in an individual ods in water and soils and that it is not completely host, and the environmentally resistant spherical adsorbed by soils. That HAV survives in the environoocyst (8–10 µm) is excreted in stools.27 The oocysts ment and migrates through soil helps to explain why appear under light microscopy as nonrefractile spheres it has been found in contor ovoids containing a aminated groundwater. Of variable number of incluwaterborne disease outsions. The infectious stage breaks in the United States of the life cycle is the from 1946 through 1980 sporulated oocyst. Sporufor which a causative lation takes 5–14 days at ater suppliers should agent was identified, HAV temperatures of 22–32oC stay updated regarding caused > 20 percent (68 of in the laboratory. 28,32 21 322 outbreaks). Upon complete sporulathese pathogens. Analytical methods. tion, two sporocysts conHAV is difficult to isolate taining two sporozoites in cell culture, and it grows each are formed within inefficiently without producing CPE. The preferred the oocyst. Laboratory exposure to an excystation host cells are primary monkey kidney, a fetal rhesus solution or ingestion and exposure to gastric condikidney-derived cell line (FRhk-4), and a liver carcitions will liberate the four sporozoites.28 noma cell line. Molecular techniques such as PCR and Health effects. Cyclosporiasis is caused by ingesgene probe have been used to detect HAV in water tion of food or liquids that have been contaminated samples. by infectious (sporulated) oocysts. Unsporulated Water treatment. HAV can be removed by conoocysts are not infectious to susceptible hosts. Illventional water treatment (coagulation, flocculation, ness is characterized by watery diarrhea, abdominal and filtration) and disinfection; however, it has been cramping, decreased appetite, and low-grade fever detected in samples containing a free chlorine resid- that can persist several weeks with bouts of remitual of 0.2 mg/L.22 tance and relapse. Oocysts are shed in the feces durResearch needs. Data on HAV distribution in sur- ing illness. Oocysts have been described in the stools face water and groundwater are needed, as well as of residents of and travelers from developing nations additional data about chlorine and other common and in association with diarrheal illness in individudisinfectants. The mechanisms by which HAV may als from North, Central, and South America; the avoid physical and chemical treatment barriers and Caribbean; the Indian subcontinent; Southeast Asia; enter finished drinking water supplies need to be Australia; and Europe. In immunocompetent indiunderstood. viduals the illness is normally self-limiting, whereas in immunocompromised individuals the illness may Protozoa be prolonged. Although clinical disease can resolve Cyclospora. Description. Cyclospora has emerged without treatment, it can be treated with trimethoas a pathogen of concern to public health officials.23–27 prin-sulfamethoxazole (co-trimaxazole), and illness This parasite was likely first observed in 1979,23 but will subside within several days.33 the organism’s coccidian nature and particular genus Occurrence, survival, and outbreaks. Evidence identity were not confirmed until 1993.28 The name strongly suggests that Cyclospora is transmitted by TABLE 2 Attributes of Cryptosporidium and Cyclospora W 114 VOLUME 91, ISSUE 9 © 1999 American Water Works Association, Journal AWWA September 1999 JOURNAL AWWA Because little is known about microsporidia and Cyclospora, water purveyors should keep themselves updated regarding these pathogens. It has been only during the past decade that microsporidia (above left and right) have been documented as human pathogens. Its identity confirmed only recently in 1993, Cyclospora (right) has emerged as a pathogen of concern to health officials. water. Two waterborne outbreaks have been described. In an outbreak among British soldiers and dependents stationed in a small military detachment in Nepal, 12 of 14 people developed diarrhea. Cyclospora oocysts were detected in stool samples from six of eight patients. Water treatment by filtration and chlorination did not affect the integrity of the oocysts. Chlorine residuals remained within acceptable limits (0.3–0.8 mg/L), and no coliform-indicator bacteria were detected. However, Cyclospora oocysts were recovered from the drinking water supply by membrane filtration and detected by light microscopy.34 The only suspected waterborne outbreak of cyclosporiasis in the United States occurred in a hospital in Chicago. Stool samples from 14 of the 21 people reporting diarrheal illness after exposure to a common water source (a storage tank) were collected and examined using a modified acid-fast stain. Samples from 11 of the patients were positive for Cyclospora. Although no Cyclospora sp. oocysts were found in the water supply, an epidemiological survey strongly suggested correlation with the source. The source of the contamination was never positively identified.26 In 1996, 17 geographically unrelated outbreaks of Cyclospora occurred in North America—in Texas, Florida, New York, New Jersey, Massachusetts, Illinois, Pennsylvania, Ohio, South Carolina, Connecticut, Maryland, Vermont, New Hampshire, Virginia, and Washington, D.C., and in Toronto, Canada. The suspected vehicle of transmission was Guatemalan raspberries. A 1995 outbreak of cyclosporiasis was also attributed to the consumption of contaminated raspberries.35 SEPTEMBER 1999 Little is known about survival of the oocysts in various conditions or what treatment can effectively inactivate the oocysts. However, the behavior of Cyclospora may be similar to that of Cryptosporidium, a related pathogen. Analytical methods. Under fluorescent illumination (excitation 375 nm, emission > 420 nm), the oocyst walls autofluoresce and the bluish spherical oocysts can easily be seen at 200X magnification.36 Clinically, Cyclospora sp. oocysts in stools are identified by staining with an acid-fast stain. Some oocysts commonly fail to take up the dye, which may complicate identification.28,37 A modified safranin technique with microwave heating is reported to uniformly stain the oocysts a brilliant orange.38 An epidemiological study in the United Kingdom reported that the coccidian Cryptosporidium and Cyclospora are often confused in the laboratory.27 Although these parasites look similar, differences do exist (Table 2). Cyclospora is twice as large as Cryptosporidium and autofluoresces under ultraviolet illumination using a 330–380-nm filter. Research needs. Fundamental research is needed to develop both species-specific monoclonal antibodies and molecular techniques to determine oocyst viability, taxonomy, species identification, infectivity and virulence; to determine water treatment processes that remove and inactivate Cyclospora oocysts; and to better understand the epidemiology of cyclosporiasis in humans, such as the significance of waterborne transmission and the public health importance of exposure to low concentrations of Cyclospora oocysts. Microsporidia. Description. The word microsporidia (a nontaxonomic term) describes organisms in the order Microsporidia of the phylum Microspora. Only in the past decade have these parasites been documented as human pathogens. Since the first case was © 1999 American Water Works Association, Journal AWWA September 1999 COMMITTEE REPORT 115 documented in 1985, seven genera of microsporidia Occurrence, survival, and outbreaks. In the have been implicated in human disease (EnterocytoUnited States no data suggest widespread occurzoon, Encephalitozoon, Nosema, Pleistophora, Vittaforma, rence of human strains of microsporidia in surface Trachipleistophora, and a catchall genus, “micro- water, although the lack of appropriate analytical sporidium”).39–46 Host specificity may be only modmethods makes this conclusion uncertain. Because erately selective because human infection by nonmicrosporidia spores are excreted, they likely occur mammalian genera has been documented, and in sewage-contaminated water. Also, because the experimental in vitro infection of cells from various apparent reservoir of various types of animal hosts animals does not appear to be particularly restrictive.47 is large, infected hosts might maintain or even Microsporidia are obligate intracellular parasites that amplify the environmental presence of human form environmentally resistant spores. Different species infectious microsporidia. The spores of microsporidia differ in size, location in host cells, and processes of appear able to survive for weeks or months, espespore production. Human cially in cold water.49–51 species are typically ovoid Their small size may or pyriform and 1–5 µm make waterborne microlong. Human infection is sporidia difficult to rethought to follow ingesmove by filtration, and tion or inhalation of spores they could have an inethods for detecting from a contaminated envicreased ability to reach ronmental source or by groundwater under the all of these pathogens direct contact with infected influence of contamineed to be improved. individuals or animals. Innated surface water. fection begins by environAnalytical methods. mental stimulation (e.g., Standard methods for the pH shift or changing ionic sampling, identification, concentration or osmotic pressure) of the spore to and enumeration of microsporidia in water or other extrude its coiled polar filament. That filament becomes environmental media are not yet available. Howa polar tubule through which the spore injects its infecever, sampling and analysis methods currently used tious constituents (sporoplasm) into the host cell. Inside for other protozoa, such as for Giardia and Crypthe cell, the parasite undergoes its replicative life cycle. tosporidium, may allow limited recovery and enumeration of microsporidia. Detection and identifiMature spores have a layer of chitin that protects the cation of microsporidia may be best served by direct transmissible spores. After a period of infection, damaged infected host cells rupture and release large num- or indirect immunofluorescent staining using either bers of infective spores into the original host or into monoclonal or polyclonal antibodies against various components of the spore walls or other structures. the environment. Environmental contamination by Special care must be taken because both monoclonal spores has been attributed to feces, urine, respiratory secretions, or other body fluids of infected individuals and polyclonal antibodies have shown cross-reactivity among species.52–54 Because microsporidia are or animals.39,40,42,44,46 Health effects. Because microsporidia are now in a size range similar to that of bacteria and algae, recognized as capable of infecting humans, reports other organisms may interfere with or mask them of human infection are increasing. The role of micro- during analysis of environmental samples. Research sporidia in waterborne disease in the United States indicates that PCR may be able to detect and deteris yet to be determined. They may pose problems mine species and that tissue culture may be able to for the elderly or immunocompromised. Microdetermine viability.48,55,56 sporidia are isolated from 7 to 50 percent of stool Research needs. The lack of adequate data on the specimens and intestinal biopsies from acquired concentrations or infectivity of the various genera immunodeficiency syndrome (AIDS) patients with and species of microsporidia makes it impractical to otherwise unexplained chronic diarrhea, and they assess potential health risks in the United States. Neihave been detected in coinfections with Crypto- ther is it prudent to determine removal requirements sporidium.39,42,46,48,49 Infections are self-limiting in needed in drinking water treatment to meet US Enviimmunocompetent individuals.42 ronmental Protection Agency goals for health proIn immunocompromised individuals typical symptection. Reliable methods are needed to detect mitoms of microsporidial infection are chronic diarrhea, crosporidia in water so that its prevalence in raw and finished water can be determined. Additional data dehydration, and significant weight loss (> 10 percent of body weight). Microsporidial infection, which may on disinfection and removal by conventional water treatment processes need to be developed. appear like cryptosporidiosis, may contribute to higher Toxoplasma. Description.Toxoplasma is a memmortality rates. Microsporidia may infect the eyes, liver, kidney, heart, and the central nervous system. ber of the same phylum (Apicomplexa) of protozoan The pathology of microsporidia infection varies parasites as Cryptosporidium and Cyclospora. Unlike these parasites, Toxoplasma requires two hosts to comdepending on the organs that are infected. Drug treatplete its life cycle: an intermediate host and a final ment is available.34,35,37,39,41 M 116 VOLUME 91, ISSUE 9 © 1999 American Water Works Association, Journal AWWA September 1999 JOURNAL AWWA TABLE 3 Waterborne viruses, protozoa, and algal toxins of concern to the water industry* Agent Viruses Norwalk virus and caliciviruses Enteroviruses Hepatitis virus Protozoa Cyclospora Microsporidia Toxoplasma gondii Toxins Algal toxins Priority for Water Industry Drinking Water† Treatment Moderate Occurrence In Water Unknown jaundice, death Removed by conventional treatment Removed by conventional treatment Diarrhea, vomiting Unknown Unknown Yes 0.035–0.04 Varied, from diarrhea to paralysis Liver infection and damage Common Long; years Yes 0.025–0.03 Common Long; >4 months Yes 0.027 Moderate Unknown Diarrhea Unknown Unknown 8–10§ Moderate Unknown Unknown Unknown Low Unknown Diarrhea, weight loss Birth defects, brain infection Suspected, mainly foodborne No Unknown Long; up to 18 months Yes, but rare Moderate Not readily removed by conventional treatment Neurotoxins, liver disease Associated with blooms Not applicable No Low Low Environmental Persistence Documented Waterborne Outbreaks‡ Health Effects Size µm 1–5§ 10–12§ Not applicable *See text for complete review. †Priorities reflect research needs and treatment capabilities. ‡In North America §Size of cyst (definitive) host. The species name “gondii” is derived from the name of the north African rodent (the gondii, Ctenodactylus gundi) in which the parasite was first described. Toxoplasma occurs worldwide. A variety of warm-blooded animals, including humans, livestock, feral animals, and birds serve as intermediate hosts, and in these Toxoplasma multiplies asexually. Only felines act as definitive hosts; in them sexual reproduction, resulting in the formation and excretion of oocysts, occurs in the cells lining the intestinal tract. Felines acquire the infection from eating infected tissues of mammals and birds or, more rarely, from ingesting sporulated oocysts. Oocyst excretion occurs for 7–20 days. As with Cyclospora, immature oocysts are excreted in the feces of felines, and an external maturation period of one to five days is required before they become infective. Sporulated oocysts contain two sporocysts, and each sporocyst contains four sporozoites. Following ingestion, sporocysts excyst in the small intestine and release tachyzoites that can spread through the blood and lymphatic systems. Tachyzoites are rapidly dividing forms that multiply within invaded cells, causing their rupture, and that can penetrate other adjacent cells. Tissue cysts, which can contain several thousand bradyzoites (the quiescent or slowly multiplying asexual stage) encased in a cyst wall, develop in various tissues and can transmit infection to both intermediate and definitive hosts that eat the uncooked meat. Health effects. Toxoplasmosis can be acquired in four ways. Sporulated oocysts in soil, inadequately washed vegetables or fruit, and water may be ingested, SEPTEMBER 1999 as may tissue cysts in raw or undercooked meat. Tachyzoites from an infected mother may pass into the developing fetus. Such congenital toxoplasmosis may be clinically unobservable or may present as hydrocephalus, mental retardation, cerebral calcification and retinochoroiditis, or death. Less commonly toxoplasmosis may be acquired from infected organs that are transplanted. Although many infected individuals show no clinical signs or symptoms, others experience a flulike illness or swollen glands in the neck, armpits, or groin. Most people with toxoplasmosis recover without drug treatment. The incubation period is one to three weeks: 10–23 days after consumption of undercooked meat and 5–20 days in an outbreak associated with cats. Immunity is long-lasting, and the degree of immunity depends on age, exposure, and immunological status. Toxoplasmosis can be severe and widely disseminated in immunocompromised individuals, and it is the most common cause of focal brain lesions in AIDS patients. Toxoplasma is a frequent opportunistic infection in AIDS patients. Occurrence, survival, and outbreaks. Sporulation, which produces eight sporozoites within two sporocysts, depends on both temperature and aeration and takes one to five days. Unsporulated oocysts are more sensitive than sporulated oocysts to harsh environmental conditions. For example, unsporulated oocysts fail to sporulate following exposure to 60–70oC for 10 seconds, 4oC for 90 days, –5oC for 14 days, or –20oC for one day, whereas sporulated oocysts remain infectious following exposure to –5oC for 120 days.57 Ex- © 1999 American Water Works Association, Journal AWWA September 1999 COMMITTEE REPORT 117 posure of sporulated oocysts to a relative humidity of third is a colonial blue-green alga that is related to 82 percent for 30 days or 21 percent for 3 days ren- the unicellular blue-green algae. Toxins are proders them noninfective. Oocysts can remain infecduced by many but not all representatives of these tious in moist soils up to 18 months. species. The toxins produced by Anabaena and AphTwo outbreaks of toxoplasmosis associated with anizomenon are generally neurotoxins (affecting the the consumption of contaminated water have been nervous system), although those from Microcystis documented. In 1979, 32 US Army soldiers showed are hepatotoxins (affecting the liver). Other toxic evidence of infection with Toxoplasma after their return cyanobacteria are less common. Toxic cyanobactefrom maneuvers in Panama. The most likely source of ria have been reported from localities in the United infection was creek water contaminated with oocysts States, Canada, Australia, New Zealand, Japan, excreted by jungle cats,58 even though most affected China, South Africa, and Europe. individuals claimed to The toxins themselves have treated their drinkare fairly complex organic ing water with iodine compounds. The chemitablets. The second outcal structures of some break occurred in British have been known for Columbia, Canada, in many years, and new orwalk virus and 1995. Acute Toxoplasma ones have been identified calicivirus, Cyclospora, infections were identified and their structures deterin 110 people, of whom mined only recently. microsporidia, and algal 42 were pregnant. Eleven Health effects. Most infants became infected. reports of poisonings by toxins were ranked Epidemiological evidence cyanobacterial toxins of moderate concern. was consistent with a waworldwide have involved terborne source and imcattle, horses, sheep, dogs, plicated the municipal and waterfowl. Of the drinking water.59 Domesfew well-documented tic and feral cats and cougars were likely sources of cases describing humans, most involved single indioocysts that contaminated the reservoir or its feeder viduals or small groups—likely because few people streams. Water was treated by chloramine disinfec- would drink water covered by a thick algal bloom. tion without filtration. Primary chlorination was The symptoms of the various algal toxins depend thought to be unlikely to either prevent Toxoplasma on which type of toxin is involved, the amount of oocysts from sporulating or to kill sporulated oocysts. material ingested, and the body weight of the aniLittle is known about disinfection regimes that inacmal or human. Generally, the neurotoxins cause tivate oocysts. convulsions, difficulty breathing, and eventual death Analytical methods. Analytical methods to detect in susceptible animals. Humans can experience tinthe organism in water are not readily available. In gling of the fingers and toes, numbness, and hay one study,60 conventional Cryptosporidium methods fever-like symptoms. The hepatotoxins (called were used to concentrate and clarify water samples, microcystins) lead to abdominal pain, diarrhea, and after an aeration step to trigger sporulation, the vomiting, injury to the liver, and death. The effects water concentrates were fed to mice. Tissue from of the neurotoxins are more rapid than those of mice that died following inoculation were examined the hepatotoxins. microscopically for evidence of Toxoplasma infections. Occurrence and outbreaks. A few reports The blood of surviving mice was examined for anti- describe swimmers whose symptoms probably were bodies to T. gondii. caused by cyanobacterial toxins.61,62 Generally, these Research needs. Fundamental research should symptoms were brief (one to seven days) and were develop both species-specific monoclonal antibodies correlated with exposure to water that contained a and molecular techniques to identify oocysts and cyanobacterial bloom. More cases likely have determine oocyst viability, infectivity, and virulence; occurred, as most physicians probably do not recogdevelop water treatment processes that remove and nize the symptoms of algal toxins. inactivate Toxoplasma oocysts; and investigate the sigSeveral outbreaks of gastrointestinal disease nificance of waterborne transmission and the public were attributed to the ingestion of water containhealth importance of exposure to low concentrations ing toxic cyanobacteria. One in Palm Island (off the Queensland coast of Australia) in 1979,63 and one of waterborne Toxoplasma oocysts. in Salisbury, Rhodesia (now Harare, Zimbabwe),64 Toxins occurred in the absence of any other identifiable Description. Many cyanobacteria (blue-green microbial agent. Each involved the ingestion of algae) can produce toxins. The three most com- water in which a toxic cyanobacterial bloom was in mon species in North America are Anabaena flos- progress or had just been killed with copper sulaquae, Aphanizomenon flos-aquae, and Microcystis aerugfate. In Armidale, Australia, people who received inosa. The first two are filamentous species, and the water from a particular reservoir that had a bloom N 118 VOLUME 91, ISSUE 9 © 1999 American Water Works Association, Journal AWWA September 1999 JOURNAL AWWA of Microcystis developed elevated concentrations of a certain liver enzyme, although those receiving water from other sources did not. 65 One of the hepatotoxins may strongly promote liver tumors.66 A study in China suggests a correlation between exposure to water containing microcystins and the incidence of liver cancer.67 Analytical methods. An older method is a bioassay, in which an extract is prepared from algal material and injected into laboratory animals, usually mice. Early work on algal toxins incorporated this method, which determines the effects of the various toxins on animals. A newer method involves extraction and analysis by high-performance liquid chromatography.68,69 This method obviates the need for laboratory animals and identifies the particular toxins present, which the bioassay does not. Water treatment. Although conventional water treatment methods do not readily remove or inactivate cyanobacterial toxins, 70,71 activated carbon does.72,73 Ozone is also effective.70,71 Ozone oxidizes microcystin-LR extremely fast—99 percent of the toxin is removed in 15 seconds.70 The cells themselves can be removed by filtration, but it is best not to allow their entry into a treatment plant, as they may release toxins into the water upon lysis by chlorine or other disinfectants. Controlling cyanobacterial blooms with copper sulfate can cause its own problems. Cyanobacteria killed by copper sulfate may release the toxin into the water.74 However, treatment with lime has been found to counteract cyanobacteria without the release of the toxin, partly by precipitating phosphorus and by causing sedimentation of the cells.74,75 Research needs. Further research is needed on the relationship of toxic cyanobacteria to short-term and long-term human health effects such as gastroenteritis and liver cancer. Treatment strategies that use algicides such as copper sulfate and lime need further study. Studies of how to protect watersheds to prevent algal growth in reservoirs may ultimately prove the most useful. Summary—viruses, protozoa, and algal toxins Table 3 summarizes and prioritizes emerging viruses, protozoa, and toxins on the basis of information reviewed in this report. The setting of priorities involves many subjective factors and can change as new information becomes available. No members of these categories were ranked of high concern for the water treatment industry. Norwalk virus and calicivirus, Cyclospora, microsporidia, and algal toxins were ranked of moderate concern because so little is known about these agents. Water suppliers should stay updated regarding these pathogens and determine, for their utility, the likelihood of these pathogens causing waterborne disease outbreaks. Ranked of low concern were enteroviruses and hepatitis virus primarily because they can be controlled by conventional treatment and disinfection. SEPTEMBER 1999 Toxoplasma gondii was ranked low because of its rarity as a waterborne pathogen and the likelihood that it is controlled by measures that control Giardia and Cryptosporidium. However, methods for detecting all of these pathogens need to be improved, and with a better understanding of the occurrence and control of these agents, the concern about their health risks in water may change. Knowledge is the first line of defense for those who provide safe drinking water. References 1. SOBSEY, M.D. ET AL. Using a Conceptual Framework for Assessing Risks to Health From Microbes in Drinking Water. Jour. AWWA, 85:3:44 (Mar. 1993). 2. CRAUN, G.F. ET AL. Balancing Chemical and Microbial Risks of Drinking Water Disinfection. Part I. Benefits and Potential Risks. Jour. Water SRT— Aqua, 43:192 (1994). 3. CRAUN, G.F. ET AL. Balancing Chemical and Microbial Risks of Drinking Water Disinfection. Part II. Managing the Risks. Jour. Water SRT—Aqua, 43:207 (1994). 4. International Life Sciences Institute. A Conceptual Framework to Assess the Risks of Human Disease Following Exposure to Pathogens. Risk Anal., 16:841 (1996). 5 AWWA Research Division, Microbiological Contaminants Research Committee. Emerging Pathogens—Bacteria. Jour. AWWA, 91:9:101 (Sept. 1999). 6. D AGAN , R. & M ENEGUS , M.A. Nonpolio Enteroviruses and the Febrile Infant. Human Enterovirus Infections (H.A. Rotbart, editor). ASM Press, Washington (1995). 7. S CHNEIDER , K.M.; L E C HEVALLIER , M.W.; & ABBASZADEGAN, M. Occurrence of Protozoans and Enteroviruses in US Surface Water Supplies. Proc. 1997 Ann. Conf. Amer. Soc. Microbiol., Miami Beach. 8. MOSLEY, J.W. Transmission of Viral Diseases by Drinking Water. Transmission of Viruses by the Water Route. Interscience, New York (1966). 9. HAWLEY, H.B. ET AL. Coxsackievirus B Epidemic at a Boys’ Summer Camp. Jour. Amer. Medical Assn., 226:33 (1973). 10. DENIS, F.A. ET AL. Coxsackie A16 Infection From Lake Water. Jour. Amer. Medical Assn., 226:1370 (1974). 11. D’A LESSIO , D.J. ET AL . Epidemiologic Studies on Virus Transmission in Swimming Waters. EPA 600/1-80-006. USEPA, Cincinnati, Ohio (1980). 12. USEPA. National Primary Drinking Water Regulations: Monitoring Requirements for Public Drinking Water Supplies; Final Rule. Fed. Reg., 61:94:24354 (1996). 13. WHITE, D.O. & FENNER, F.J. Caliciviridae and Astroviridae. Medical Virology. Academic Press, San Diego (4th ed., 1994). © 1999 American Water Works Association, Journal AWWA September 1999 COMMITTEE REPORT 119 14. HURST, C.J.; CLARK, R.M.; & REGLI, S.E. Estimating the Risk of Acquiring Infectious Disease From Ingestion of Water. Modeling Disease Transmission and Its Prevention by Disinfection (C.J. Hurst, editor). Cambridge University Press, Cambridge, England (1996). 15. HURST, C.J. & MURPHY, P.A. The Transmission and Prevention of Infectious Disease. Modeling Disease Transmission and Its Prevention by Disinfection (C.J. Hurst, editor). Cambridge University Press, Cambridge, England (1996). 16. SOBSEY, M.D. ET AL. Survival and Persistence of Hepatitis A Virus in Environmental Samples. Viral Hepatitis and Liver Disease (A.J. Zuckerman, editor). Alan R. Liss Inc., New York (1988). 17. ALTER, M.J. National Surveillance of Viral Hepatitis. Morbidity & Mortality Weekly Rept., 32:23SS (1981). 18. Centers for Disease Control. Immune Globulin for Protection Against Viral Hepatitis. Morbidity & Mortality Weekly Rept., 30:423 (1983). 19. CRAUN, G.F. Waterborne Disease in the United States. CRC Press, Boca Raton, Fla. (1986). 20. SOBSEY, M.D. ET AL. Survival and Transport of Hepatitis A Virus in Soils, Groundwater and Wastewater. Water Sci. & Technol., 10:97 (1986). 21. LIPPY, E.C. & WALTRIP, S.C. Waterborne Disease Outbreaks—1946–80: A Thirty-five Year Perspective. Jour. AWWA, 76:2:60 (Feb. 1984). 22. BOSCH, A. ET AL. Waterborne Viruses Associated With Hepatitis Outbreaks. Jour. AWWA, 83:3:80 (Mar. 1991). 23. ASHFORD, R.W. Occurrence of an Undescribed Coccidian in Man in Papua, New Guinea. Annals of Tropical Medicine & Parasitol., 73:497 (1979). 24. OOI, WINNIE W.; ZIMMERMAN, SARAH K.; & NEEDHAM , C YNTHIA A. Cyclospora Species as a Gastrointestinal Pathogen in Immunocompetent Hosts. Jour. Clinical Microbiol., 33:1267 (1995). 25. ZERPA, R.; UCHIMA, N.; & HUICHO, L. Cyclospora cayetanensis Associated With Watery Diarrhoea in Peruvian Patients. Jour. Tropical Medicine & Hygiene, 98:325 (1995). 26. HUANG, PHILIP ET AL. The First Reported Outbreak of Diarrheal Illness Associated With Cyclospora in the United States. Annals of Internal Medicine, 123:409 (1995). 27. BENDALL R.P. & CHIODINI, P.L. The Epidemiology of Human Cyclospora Infection in the UK. Protozoan Parasites and Water (W.B. Betts et al, editors). The Royal Society of Chemistry, Cambridge, England(1995). 28. ORTEGA, YNES R. ET AL. Cyclospora Species—A New Protozoan Pathogen of Humans. New England Jour. Medicine, 328:1308 (1993). 29. ASHFORD, R.W.; WARHURST, D.C.; & REID, G.D.F. Human Infection With Cyanobacterium-like Bodies. Lancet, 341:1034 (1993). 30. RELMAN, DAVID A. ET AL. Molecular Phylogenetic Analysis of Cyclospora, the Human Intestinal Pathogen, Suggests That It Is Closely Related to 120 VOLUME 91, ISSUE 9 31. 32. 33. 34. 35. 36. 37. 38. 39. 40. 41. 42. 43. 44. 45. 46. 47. Eimeria Species. Jour. Infectious Diseases, 173:440 (1996). SMITH, H.V. ET AL. Cyclospora in Nonhuman Primates in Gombe, Tanzania. Veterinary Record, 138:528 (1996). SMITH, H.V. ET AL. Sporulation of Cyclospora sp. Oocysts. Appl. & Envir. Microbiol., 63:1631 (1997). MADICO, GUILLERMO ET AL. Treatment of Cyclospora Infections With Co-trimoxazole. Lancet, 342:122 (1993). RABOLD, GREGORY J. ET AL. Cyclospora Outbreak Associated With Chlorinated Drinking Water. Lancet, 344:1360 (1994). CHAMBERS, J. ET AL. Outbreaks of Cyclospora cayetanensis Infection—United States, 1996. Morbidity & Mortality Weekly Rept., 45:549 (1996). BERLIN, O.G.W. ET AL. Autofluorescence and the Detection of Cyclospora Oocysts. Emerging Infectious Diseases, 4:127 (1998). KNIGHT, PAMELA. Once-misidentified Human Parasite Is a Cyclosporan. ASM News, 61:520 (1995). V ISVESVARA , G.S. ET AL . Uniform Staining of Cyclospora Oocysts in Fecal Smears by a Modified Safranin Technique With Microwave Heating. Jour. Clinical Microbiol., 35:730 (1997). BRYAN, R.T. Microsporidia. Principles and Practices of Infectious Diseases (G. Mandel, J.E. Bennett, and R. Dolin, editors). Churchill and Livingstone, New York (1995). CALI, A. & OWEN, R.L. Microsporidiosis. The Laboratory Diagnosis of Infectious Diseases: Principles and Practice (A. Balows, W. Hausler Jr., and E.H. Lennette, editors). Springer-Verlag, Georgetown, Texas (1992). FIELD, A.S. ET AL. Myositis Associated With a Newly Described Microsporidian, Trachiplestophora hominis in a Patient With AIDS. Jour. Clinical Microbiol., 34:2803 (1996). GARCIA, L.S. & BRUCKNER, D.A. Diagnostic Medical Parasitology. American Society for Microbiology, Washington (1993). HARTSKEERL, R.A. ET AL. Genetic and Immunological Characterization of the Microsporidian Sepata intestinalis. Cali, Kotler, and Orenstein, 1993 reclassification to Encephalitozoon intestinalis. Parasitol., 110:277 (1995). M ARSHALL , M. ET AL . Waterborne Protozoan Pathogens. Clinical Microbiol. Review, 10:67 (1997). SILVIERA, H. & CANNING, E.U. Vittaforma corneae: n-comb for the Human Microsporidium Nosema corneae Shaduck, Meccoli, Davis, and Font 1990, Based on Its Ultrastructure in the Liver of Experimentally Infected Athymic Mice. Jour. Eukaryotic Microbiol., 42:158 (1995). WEBER, R. ET AL. Human Microsporidial Infections (Review). Clinical Microbiol. Review, 7:426 (1994). SILVIERA, H. & CANNING, E.U. In Vitro Cultivation of the Human Microsporidium Vittaforma corneae: Development and Effect of Albendazole. Folia Parasitologica, 42:241 (1995). © 1999 American Water Works Association, Journal AWWA September 1999 JOURNAL AWWA 48. COYLE, C.M. ET AL. Prevalence of Microsporidiosis Due to Enterocytozoon bieneusi and Encephalitozoon (Septata) intestinalis Among Patients With AIDS-related Diarrhea—Determination by Polymerase Chain Reaction to the Microsporidian Small-subunit rrna Gene. Clinical & Infectious Diseases, 23:1002 (1996). 49. AMIGO, J.M. ET AL. Longevity and Effects of Temperature and Viability and Polar Tube Extrusion of Spores of Gluged stephoni Microsporidian Parasite of Commercial Flatfish. Parasitol. Res., 82:21 (1966). 50. AVERY, S.W. & UNDEEN, A.H. The Isolation of Microsporidia and Other Pathogens From Concentrated Ditch Water. Jour. Amer. Mosquito Control Assn., 3:54 (1987). 51. WALLER, T. Sensitivity of Encephalitozoon cuniculi to Various Temperatures, Disinfectants, and Drugs. Laboratory Animals, 13:227 (1979). 52. ALDRAS, A.M. ET AL. Detection of Microsporidia by Indirect Immunofluorescence Antibody Test Using Polyclonal and Monoclonal Antibodies. Jour. Clinical Microbiol., 32:608 (1994). 53. NEIDERKORN, J.Y.; SHADDUCK, J.A.; & WEIDNER, E. Antigenic Cross-reactivity Among Different Microsporidian Spores as Determined by Immunofluorescence. Jour. Parasitol., 66:675 (1980). 54. VAN G OOL , T. ET AL . High Seroprevalence of Encephalitozoon Species in Immunocompetent Subjects. Jour. Infectious Diseases, 175:1020 (1997). 55. DIDIER, E.S. ET AL. Characterization of Encephalitozoon (Septata) intestinalis Isolates Cultures From Nasal Mucosa and Bronchoalveolar Lavage Fluids of Two AIDS Patients. Jour. Eukaryotic Microbiol., 43:34 (1996). 56. FEDORKO, D.P. & HIJAZI, Y.M. Application of Molecular Techniques to the Diagnosis of Microsporidial Infection. Emerging Infectious Diseases, 2:183 (1996). 57. JACKSON, M.H. & HUTCHISON, W.M. The Prevalence and Source of Toxoplasma Infection in the Environment. Advances in Parasitol., 28:55 (1989). 58. BENENSON, M.W. ET AL. Oocyst-transmitted Toxoplasmosis Associated With the Ingestion of Contaminated Water. New England Jour. Medicine, 307:666 (1982). 59. BOWIE, W.R. ET AL. Outbreak of Toxoplasmosis Associated With Municipal Drinking Water. Lancet, 350:173 (1997). 60. ISAAC-RENTON, J. ET AL. Detection of Toxoplasma gondii in Drinking Water. Appl. & Envir. Microbiol., 64:2278 (1998). 61. SCHWIMMER, M. & SCHWIMMER, D. Medical Aspects of Phycology. Algae, Man, and the Environment (D.F. Jackson, editor). Syracuse University Press, Syracuse, N.Y. (1968). 62. GORHAM, P.R. & CARMICHAEL, W.W. Hazards of Freshwater Blue-green Algae (Cyanobacteria). Algae and Human Affairs (C.A. Lembi and J.R. Waaland, editors). Cambridge University Press, Cambridge, England (1988). SEPTEMBER 1999 63. HAWKINS, P.R. ET AL. Severe Hepatoxicity Caused by the Tropical Cyanobacterium (Blue-green Alga) Cylindrospermopsis raciborskii (Woloszynska) Seenaya and Subba Raju Isolated From a Domestic Water Supply Reservoir. Appl. & Envir. Microbiol., 50:1291 (1985). 64. ZILBERG, B. Gastroenteritis in Salisbury European Children—A Five-Year Study. Central African Jour. Medicine, 12:164 (1966). 65. FALCONER, I.R.; BERESFORD, A.M.; & RUNNEGAR, M.T.C. Evidence of Liver Damage by Toxin From a Bloom of the Blue-green Alga Microcystis aeruginosa. Medical Jour. Australia, 1:511 (1983). 66. NISHIWAKI-MATSUSHIMA, R. ET AL. Liver Tumor Promotion by the Cyanobacterial Cyclic Peptide Toxin Microcystin-LR. Jour. Cancer Res. & Clinical Oncol., 118:420 (1992). 67. YU, S.-Z. Blue-green Algae and Liver Cancer. Toxic Cyanobacteria: Current Status of Research and Management (D.A. Steffensen and B.C. Nicholson, editors). Australian Center for Water Quality Research, Salisbury, Australia (1994). 68. CODD, G.A. ET AL. Production, Detection, and Quantification of Cyanobacterial Toxins. Toxicity Assessment, 4:499 (1989). 69. MERILUOTO, J.A.O. & ERIKSSON, J.E. Rapid Analysis of Peptide Toxins in Cyanobacteria. Jour. Chromatography, 438:93 (1988). 70. ROSITANO, J. & NICHOLSON, B.C. Water Treatment Techniques for the Removal of Cyanobacterial Peptide Toxins From Water. Australian Center for Water Quality Research Rept. 2/94 (1994). 71. KEIJOLA, A.M. ET AL. Removal of Cyanobacterial Toxins in Water Treatment Processes: Laboratory and Pilot-scale Experiments. Toxicity Assessment, 3:643 (1988). 72. FALCONER, I.R. ET AL. Using Activated Carbon to Remove Toxicity From Drinking Water Containing Cyanobacterial Blooms. Jour. AWWA, 81:2:102 (Feb. 1989). 73. HIMBERG, K. ET AL. The Effect of Water Treatment Processes on the Removal of Hepatotoxins From Microcystis and Oscillatoria Cyanobacteria: A Laboratory Study. Water Res., 23:979 (1989). 74. KENEFICK, S.L. ET AL. Toxin Release From Microcystis aeruginosa After Chemical Treatment. Water Sci. & Technol., 27:433 (1993). 75. LAM, A.K.-Y., ET AL. Chemical Control of Hepatotoxic Phytoplankton Blooms: Implications for Human Health. Water Res., 29:1845 (1995). About the authors: This article is the work of the Microbiological Contaminants Research Committee of the AWWA Research Division. It was prepared by Mark W. LeChevallier (chair) with contributions from committee members Morteza Abbaszadegan, Anne K. Camper, Christon J. Hurst, George Izaguirre, Marilyn M. Marshall, Donna Naumovitz, Pierre Payment, Eugene W. Rice, Joan Rose, Steve Schaub, Theresa R. Slifko, Darrell B. Smith, Huw V. Smith, Charles R. Sterling, and Mic Stewart. © 1999 American Water Works Association, Journal AWWA September 1999 COMMITTEE REPORT 121