Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Trichinosis wikipedia , lookup
Gastroenteritis wikipedia , lookup
Oesophagostomum wikipedia , lookup
Poliomyelitis eradication wikipedia , lookup
Traveler's diarrhea wikipedia , lookup
Marburg virus disease wikipedia , lookup
Hospital-acquired infection wikipedia , lookup
Eradication of infectious diseases wikipedia , lookup
2009 flu pandemic by country wikipedia , lookup
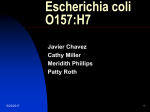
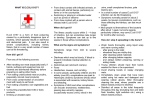
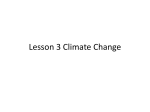
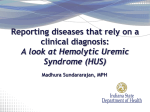
The importance of secondary spread in the epidemiology of Escherichia coli O157 infection in Scotland, 1999-2008 Clifton House, Clifton Place Glasgow G3 7LN, Scotland Email: [email protected] Tel: +44-141 300 1118 Mary Locking1, Kevin Pollock1, Lesley Allison2, Linda Rae1, Mary Hanson2, John Cowden1 1 Health Protection Scotland, Glasgow, Scotland 2 Scottish E. coli O157/VTEC Reference Laboratory, Edinburgh, Scotland Background and Aims: Results: Escherichia coli O157 remains an important public health challenge worldwide, particularly because of its association with haemolytic uraemic syndrome (HUS)1. The low infectious dose exacerbates its potential to cause both secondary spread, and large outbreaks2,3,4. Most information on secondary spread of E. coli O157 worldwide derives from outbreaks, or from settings or sub-groups not necessarily comparable with the population as a whole. From 1999 to 2008, 2228 laboratory-confirmed E. coli O157 cases were reported to HPS (mean 223 annually). The mean annual incidence rate was 4.4 per 100,000 population (Figure 1). Children under 10 accounted for 36% of all cases. Scotland consistently reports higher rates of infection than neighbouring countries (Figure 1). Historically, most cases are sporadic (Figure 2); and research in Scotland found a strong association between sporadic infection and exposures to livestock faeces5. In 1999, in close liaison with the Scottish E. coli O157/VTEC Reference Laboratory (SERL), Health Protection Scotland (HPS) established enhanced surveillance of all E. coli O157 cases – primary and secondary, outbreak and sporadic – based on the entire population. We analysed this data to identify the proportion of secondary spread, and to explore differences between secondary and primary cases, in single households as well as in outbreaks. Methods: A case is defined as one person-infection-episode, with laboratory confirmation as either “culture positive” (isolates of E. coli O157 cultured from faeces) or “serum positive” cases (antibodies to E. coli O157 detected in serum). HPS integrates microbiological information from SERL with epidemiological, clinical and exposure details from local Health Protection and Environmental Health investigations. Secondary cases are those symptomatic cases from whose onset date, and an assumed incubation period3, we can infer that contact3 with a confirmed case was the most likely source of infection. HPS surveillance systems identify “general” outbreaks ie those affecting members of more than one household, or residents of an institution. Other cases are therefore sporadic, or are members of a single household, for ease of reference referred to collectively as “sporadic cases”. Laboratory confirmed cases also meeting the definitions of HUS6 are also included in the HPS E. coli O157 enhanced surveillance dataset. Most cases (2026/2228, 91%) reported gastrointestinal symptoms; 41% were hospitalised and 9% developed HUS. All 1118 cases reported 2004-2008 provided symptoms details; 59% had bloody diarrhoea. Of the 2026 symptomatic cases, 12% were secondary infections (11% of all cases) (Figure 3), with similar risk of HUS as primary cases (p = 0.95) (Figure 4); 12% of all HUS occurred in secondary cases. Secondary cases were younger (median 13 years) than primary cases (median 20 years, p < 0.0005), with 47% of secondary cases under 10 years old. Although 20% of all cases occurred in outbreaks, 80% of all cases (and 64% of secondary cases) were single household cases or clusters (“sporadic cases”) (Figure 2 and Figure 5). Sporadic and outbreak cases had similar risk of HUS (p = 0.89). Bloody diarrhoea was more common in sporadic (62%) than outbreak cases (46%, p < 0.0005). Sporadic and outbreak secondaries had the same risk of HUS (p = 0.97); and risk of HUS increased with bloody diarrhoea, in all cases (p < 0.0005). Figure 4: Secondary spread, hospital admissions and HUS: Symptomatic cases, E.coli O157 Enhanced Surveillance in Scotland 1999-2008 (n=2026) 172 24 58 964 164 644 Primary case Secondary case HUS Figure 1: E.coli O157: Laboratory isolates, 1984-2008 (rate per 100,000 population) Hospitalised, no HUS Recovered at home Figure 5: Secondary spread, outbreak or sporadic cases: Symptomatic cases, E.coli O157 Enhanced Surveillance in Scotland 1999-2008 (n=2026) 12 Cases per 100,000 population 10 8 6 200 4 160 2 120 0 1984 1986 Scotland 1988 1990 1992 1994 1996 1998 England (2000 onwards) England & Wales (pre 2000) 2000 2002 Wales (2000 onwards) 2004 2006 N Ireland 2008 Ireland Data outwith Scotland courtesy of Health Protection Agency Belfast/London, and Health Protection Surveillance Centre Dublin. (Figures outwith Scotland are provisional, and include verotoxin positive cases only; 2008 figures outwith Scotland are provisional) 40 Figure 2: E.coli O157: Laboratory confirmed cases, Scotland 1984-2008 0 Number of cases Sporadic Secondary Outbreak Primary Outbreak Secondary Discussion and Conclusions: 400 300 200 100 1984 1986 1988 1990 1992 1994 1996 1998 General outbreak (involves members of more than one household, or residents of an institution) 2000 2002 2004 2006 Sporadic (sporadic cases or single household clusters) Figure 3: Secondary, primary or asymptomatic cases; E.coli O157 Enhanced Surveillance in Scotland 1999-2008 Number of cases † Only two outbreak secondary cases were identified each year in 2000 and 2007 Sporadic Primary 500 0 80 2008 † 2007 2006 2005 2004 2003 2002 2001 † 2000 1999 2008 Person-to-person spread accounted for 12% of all symptomatic cases. Most secondary cases occurred outside outbreaks ie they acquired infection from members of their own households, as observed in other studies7,8. The extent of secondary spread in Scotland would not be identifiable without enhanced surveillance. Even so, it may be underestimated e.g. if contacts submitted no, or late, samples. Whilst infection control is rightly emphasised in outbreaks, the risk of secondary spread and HUS within single households may be underestimated. We recommend that all cases of suspected infectious bloody diarrhoea (particularly if bloody) should be investigated microbiologically and monitored clinically9. Cases should be given immediate infection control advice, without waiting for confirmation of an outbreak10. References: [1] Tarr PI, Gordon CA, Chandler WL. Shiga-toxin-producing Escherichia coli and haemolytic uraemic syndrome. Lancet 2005; 365: 1073-86. 300 [2] Scottish Executive Health Department/Food Standards Agency (Scotland). Report of the E. coli O157 Task Force. Edinburgh: The Stationery Office, July 2001. http://www.food.gov.uk/news/newsarchive/2001/oct/ecolitask. 250 [3] Health Protection Network. Guidance for the Public Health Management of Infection with Verotoxigenic Escherichia coli (VTEC). Health Protection Network Scottish Guidance 3. Health Protection Scotland; Glasgow (Scotland):2008. http://www.hps.scot.nhs.uk/giz/guidelinedetail.aspx?id=39336. [4] Working Group of the Former PHLS Advisory Committee on Gastrointestinal Infection. Preventing person-to-person spread following gastrointestinal infections: guidelines for public health physicians and environmental health officers. Commun Dis Public Health. 2004; 7:362-384. http://www.hpa.org.uk/cdph/issues/CDPHvol7/No4/guidelines2_4_04.pdf. 200 150 [5] Locking ME, O’Brien SJ, Reilly WJ, Wright EM, Campbell DM, Coia JE et al. Risk factors for sporadic cases of Escherichia coli O157 infection: the importance of contact with animal excreta. Epidemiol Infect 2001; 127: 215‑220. 100 [6] Pollock KGJ, Locking ME, Rae L. Enhanced surveillance of thrombotic microangiopathies in Scotland, 2003‑2008. Health Protection Scotland Weekly Report 2009; 43 (10): 104‑105. http://www.documents.hps.scot.nhs.uk/ewr/pdf2009/0910.pdf. 50 [7] Werber D, Mason BW, Evans MR, Salmon RL. Preventing Household Transmission of Shiga Toxin-Producing Escherichia coli O157 Infection: Promptly Separating Siblings Might Be The Key. Clin Infect Dis 2008; 46: 1189‑96. 0 1999 2000 2001 2002 Primary symptomatic 2003 2004 Secondary symptomatic 2005 2006 Asymptomatic 2007 2008 [8] Seto EYW, Soller JA, Colford Jnr JM. Strategies to Reduce Person-to-Person Transmission during Widespread Escherichia coli O157:H7 Outbreak. Emerg Inf Dis 2007; 13(6): 860‑866. [9] Pollock KGJ, Stewart A, Beattie TJ, Todd WTA, Ahn CK, Tarr PI, Cowden JM. From diarrhoea to haemolytic uraemic syndrome – when to seek advice. J Med Micro 2009, 58, 397‑398. http://jmm.sgmjournals.org/cgi/reprint/58/4/397. [10] Locking M, Cowden J. E. coli O157. Early clinical diagnosis and outbreak identification are essential to prevent serious sequelae and further transmission. BMJ 2009; 339:b4076. http://www.bmj.com/cgi/content/extract/339/oct06_3/b4076. Acknowledgements HPS and SERL particularly wish to thank participating patients and their relatives; and the following groups across Scotland: Health Protection Teams in NHS Boards; Environmental Health Officers; Consultant Microbiologists and Diagnostic Laboratory staff; and participating General Practitioners and Clinicians. We also acknowledge other present and previous staff at HPS and SERL. Poster produced by the Graphics Section, Health Protection Scotland