Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
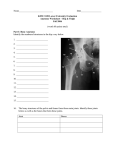
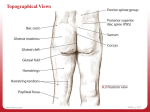
Diagnosis and Treatment of Femoro-acetabular Impingement and other Hip Conditions in the Athlete Thomas Brandon, MD Peninsula Orthopaedic Associates Salisbury University Sports Medicine Symposium January 2010 Overview • Femoro-acetabular Impingement including labral tears • Ligamentum Teres injuries • Snapping hip (coxa saltans) • Instability CLINICAL ANATOMY • Femoral head/neck & acetabulum ( nl anteversion 15-20 degrees) • Acetabular labrum & cartilage • Ligamentum teres • Iliofemoral ligaments CLINICAL ANATOMY • Iliopsoas muscle • Tensor fascia lata • Trochanteric bursa History & Examination of the Hip • Onset: acute or chronic, traumatic, atraumatic • Type of pain: catching, locking, aching, stiffness, slipping • Location of pain: central of peripheral History and Examination of the Hip • Gait and posture • Back exam • Pelvic obliquity, LE rotation and leg length • Atrophy & palpation • Active and passive ROM • Neurovascular exam Hip examination – Specific Tests • Thomas test • Ober’s test Hip Examination – Specific Tests • Faber’s test • Anterior labral test • Posterior labral test Hip Examination – Special Tests • Lateral compression test (osteitis pubis) • Piriformis test Imaging Imaging Femoro-acetabular Impingement (FAI) - Ganz • Abnormal contact of femoral head and/or neck on the acetabulum • Creates either abnormal shear forces on acetabulum or direct contact on the head or neck causing damage to the cartilage and labrum Femoro-acetabular Impingment • Congenital etiology: abnl femoral and acetabular anteversion are caused by various intrauterine position of the fetal limbs • Decrease in acetabular +/- femoral anteversion are a major cause of hip pain and arthritis (Tonnis et al, JBJS, 1999) Femoro-acetabular Impingement • Sub clinical SCFE or growth disturbance of proximal femur produces nonspherical head (pistol grip deformity) • Coxa profunda (deep acetabulum) FAI • 2 types – both cause abnormal forces: labral & cartilage damage, ? Increased risk of OA • Cam type • Pincer type • Combination of both FAI – Cam Type • Increased retroversion of head/neck (measured with CT) • Decreased off set of head neck ( <10mm) and/or loss of sphericity ( alpha angle > 50 deg) • More common in young athletic malesretroversion of femur more common FAI-CAM TYPE • Non-spherical head creates shear forces causing outside-in abrasion • Anterior superior chondral damage first then labral avulsion at base and detachment FAI – PINCER TYPE • Anterior rim of acetabulum contacts the head or head/neck junction • Increased acetabular retroversion (figure of 8 sign) • Coxa profunda: center of head is medial to posterior acetabular wall or medial wall of acetabulum is medial to ilioischial line FAI – PINCER TYPE • More common in middle age athletic women • Direct contact of acetabular rim on femoral head neck causing labral tear FAI – SYMPTOMS & SIGNS • Typically chronic onset but can be acute • Groin pain aggravated by activities and sitting • Night pain common • Locking, catching , giving way • Limp, trendelenberg, positive impingement sign • Decreased flexion and internal rotation FAI TREATMENT • • • • NSAID’s Therapy Steroid injection Often not successful FAI TREATMENT • Open versus arthroscopic versus combined • Goal is to address the bony and/or labral pathology FAI – OPEN TREATMENT • Surgical dislocation of the hip (Ganz, JBJS, 2006 OPEN TREATMENT RESULTS • Depends on labral debridement vs repair (Espinosa et al. JBJS,2007) • Patients with labral repair had superior clinical and radiographic results at 2 yrs OPEN TREATMENT DISADVANTAGES • Large exposure requiring trochanteric osteotomy • Theoretical increased risk to blood supply • Requires experienced hip surgeon • Prolonged recovery FAI – ARTHROSCOPIC TREATMENT • Out patient procedure • Can address central and peripheral compartments treating intra- and extra-articular pathology FAI – ARTHROSCOPIC TREATMENT • • • • Supine or lateral position Distraction of hip joint 3-4 portals Labral repair/ debridement + rim trimming – pincer lesions • Osteochondroplasty of head/neck junction – cam lesions FAI – ARTHROSCOPIC TREATMENT RESULTS • Larson, et al. Arthroscopy,2008 • 96 pts 3 yr f/u cam and pincer FAI • Significant improvement of pain, function and alpha angle FAI – ARTHROSCOPIC TREATMENT • Technically difficult • Amount of acetabular version correction limited? • Obesity a relative contra-indication Complications • Iatrogenic cartilage injury • Nerve or vessel injury: direct or traction • Fracture or subluxation/dislocation • Adhesions • DVT/PE • Progressive arthritis • Infection • Abdominal fluid extravasation FAI - Combined • Arthroscopy + limited open approach (Hueter) • Allows treatment of intra-articular pathology and easier contouring/bone trimming +/- labral fixation (Arthroscopy 2009) Post OP Management • 20 lbs wt bearing & cpm 4 hrs/d x 2 wks • If microfx : pwb x 8 wks • Rotation boots to prevent ER x 14-21 days • PT to restore passive IR & hip pendulums • Return to sports avg 3.4 mos (Phillipon AJSM, 2009) LIGAMENTUM TERES TEARS • Diagnosis is increasing • 3rd most common finding at arthroscopy • Symptoms include deep anterior groin pain, catching, locking, popping and giving way • Often occurs after a injury: football, skiing, gymnastics, MVA • Exam is non-specific groin pain with ROM LIGAMENTUM TERES TEARS • Imaging may be diagnostic but majority found at time of arthroscopy LIGAMENTUM TERES TEARS • Treatment: arthroscopic debridement • 96% improvement of symptoms and return to activity (Byrd, Arthroscopy, 2004) SNAPPING HIP – COXA SALTANS • External – snapping of iliotibial band over greater trochanter • Internal – snapping of iliopsoas tendon over femoral head and/or iliopectineal eminence SNAPPING HIP - ETIOLOGY • Direct injury – falls and direct blows • Training errors – common in dancers, gymnasts • Mal-alignment of lower extremities – decreased head/neck angle, varus knees, pronated feet SNAPPING HIP • External – snapping painful sensation localized to greater trochanter • Internal – clicking sensation rather than snapping more internal and central SNAPPING HIP • Internal occurs in athletes who have frequent rotation of hip at high flexion angles • Click & pain with flexion/abd of hip followed by ext/adduction SNAPPING HIP • External is usually caused by abnormal thickening of posterior band of ITB • Common in cyclists and runners • Athlete can often demonstrate painful snapping that is palpable SNAPPING HIP • Internal: pain reproduced by flexion & abd followed by ext & adduction • May have palpable snap sometimes reduced with finger pressure SNAPPING HIP • Others causes : trochanteric burstis, loose bodies and labral tears, gluteus medius tears, ? instability SNAPPING HIP • Imaging: xrays and CT to r/o other pathology; MRI occasionally helpful • US and bursography can be diagnostic with experienced radiologists SNAPPING HIP • Both usually respond to rest, NSAID’s, stretching and strengthening exercises • Steroid injections • Return to sports in 46 wks SNAPPING HIP - Treatment • External : open or arthroscopic iliotibial band release and bursectomy • Excellent results in small series; Ilizalituri, et al, Arthoscopy, 2006 SNAPPING HIP – Post-op Rehab • External release – crutches wbat until pain free; stretch/strengthen abd, etc; return to sports when pain free and strength 90% SNAPPING HIP - Treatment • Internal: open – difficult dissection • Complication rates up to 50%: nerve injury, hematoma, infection, etc SNAPPING HIP - Treatment • Arthroscopic release • Successful in small series; Flanum, AJSM, 2007 • Few complications • Return to sports at ~6 mos SNAPPING HIP INTERNAL– Post-op Rehab • Wks 1-4: protected WB until active hip flexion regained and pain 3/10 • Wks 4-8: functional gait, ROM and strengthening to limits of pain • Return to sports when strength 90% HIP INSTABILITY • Inherently stable joint due to bony and soft tissue constraints • Acetabulum is oriented 45 degrees caudally and 15-20 degrees anteverted HIP INSTABILITY • Soft tissues provide secondary restraints • Capsuloligamentous structures • Labrum • Cartilage • Ligamentum teres • Transverse acetabular ligament HIP INSTABILITY • Traumatic: acute defined event resulting in subluxation or dislocation • Atraumatic: subtle, not well defined, can be overuse or due to congenital abnormality TRAUMATIC HIP INSTABILITY • Obvious or subtle minimal trauma • Most common mechanism is MVA • Athletics: fall on knee with hip flexed or blow from behind • Reported in almost all sports: football, rugby, gymnastics, soccer, etc TRAUMATIC HIP INSTABILITYDISLOCATION • Acute injury: usually posterior • Hip held in flexion, IR and adduction • Xrays show dislocation +/-fx TRAUMATIC HIP DISLOCATION • Management: closed reduction within 6 hrs to reduce AVN • CT to confirm reduction • Surgery if loose body or fx • Crutches TTWB x 6 wks • MRI @ 6 wks to R/O AVN • Return to play depends on imaging results and exam TRAUMATIC HIP SUBLUXATION • Misdiagnosed as sprain or strain • Same mechanism as dislocation • Usually less energy involved • Have high index of suspicion TRAUMATIC HIP SUBLUXATION • PE: pain with rom and may have loss of motion • Xrays usually negative but oblique may show post lip fx (bankart- like lesion) TRAUMATIC HIP SUBLUXATON • MRI- characteristic triad: posterior lip fx, iliofemoral ligament disruption, hemarthrosis (Moorman, JBJS,2003) • Can also show marrow edema, chondral injury, loose bodies TRAUMATIC HIP SUBLUXATION • Consider fluoroscopic aspiration if large hemarthrosis • MRI @ 6wks to r/o avn – hip arthroscopy if indicated • Repeat MRI at 12 wks to r/o AVN MANAGEMENT OVERVIEW Shindle,et alClin sports med2006 TRAUMATIC HIP INSTABILITY PROGNOSIS • Traumatic dislocationavn reported in 117%, increased risk of late OA up to 30% • Traumatic subluxation –risks unknown; avn in 2/8 pro football players (Moorman, JBJS,2003) ATRAUMATIC HIP INSTABILITY • No discrete event • Difficult diagnosis • Symptoms include leg giving out, pain when rising from a chair or getting in or out of a car, painful clicking or catching • Broad DDX: labral tear, FAI, dysplasia, AVN, loose bodies, osteitis pubis, GU, spine, hernia, GYN, PVD, infection, tumors, stress fx, inflammatory arthritis, etc ATRAUMATIC HIP INSTABILITY • Overuse or repetitive motion injury involving hip rotation with axial loading: hockey, gymnastics, golf, ballet • Hip dysplasia • Congenital conditions: Ehlers-Danlos, Marfan’s ATRAUMATIC HIP INSTABILITY • Athlete can often describe motion that reproduces pain: driving ball in golf and sideline throws in FB • Over time can lead to coxa saltans due to overcompensation of iliopsoas ( flexion contracture & back pain) ATRAUMATIC HIP INSTABILITY • Evaluate other joints for laxity • Positive dial test • Axial distraction/apprehension test • Prone extension-external rotation test produces anterior hip pain • Increased prom • Pt may voluntarily sublux hip ATRAUMATIC HIP INSTABILITYIMAGING • CE angle of Wiberg: nl greater than 25 degrees • Tonnis angle: nl less than 10 degrees • Sharp’s angle greater than 45 degrees is abnl ATRAUMATIC INSTABILITY IMAGING • MRA – capsule appears thickened at lateral margin of anterior capsule with increased signal intensity • Local anesthetic injection at time of MRA can confirm pain is intra-articular ATRAUMATIC INSTABLILITY MANAGEMENT • Modification of activity, nsaid’s, therapy • Arthroscopy to reduce volume of hip capsule • Byrd (Arthroscopy,2003); Philippon, Knee Surg Sports Trauma, 2007) report significant improvement and return to sports. ATRAUMATIC HIP INSTABILITY MANAGEMENT • Open osteotomy for dysplastic hips • Prognosis for return to sports? SUMMARY • Hip pain in athlete is multi-factorial • Diagnosis can be difficult • Must have a high index of suspicion as misdiagnosis can have poor prognosis • Hip arthroscopy is becoming an important diagnostic and therapeutic technique in the treatment