Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
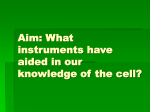
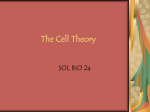
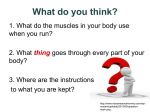
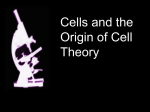
RENAL BIOPSY FOR A HCV POSITIVE PATIENT WITH DIABETIC MELLITUS AND HYPERTENSION Li-Mei Jang1, Cheng-Hsin Chu2,3, Tung-Ying Chen4, Chih-Jen Wu1,2,5, Han-Hsiang Chen1,2,6 , and Yu-Wei Chen1,2 1 Division of Nephrology, 3Division of Gastroenterology, 4Department of pathology, Department of Internal Medicine, Mackay Memorial Hospital, Taipei, Taiwan 2Mackay Medicine, Nursing and Management College, Taipei, Taiwan 5Graduate 6National Institute of Medical Science, Taipei Medical University, Taipei, Taiwan Taipei College of Nursing, Taipei, Taiwan Reprint requests and correspondence to: Dr. Yu-Wei Chen Department of Nephrology, Mackay Memorial Hospital. No.92, sec. 2, Zhongshan N. Rd., Zhongshan Dist., Taipei City 10449, Taiwan Tel:+886-2-25433535; Fax:+886-2-25433642 ; E-mail: [email protected] Words count for title: 12 Words count for case: 332 Words count for answer: 177 58-year-old Taiwanese man, who had history of hypertension and diabetic mellitus with proliferative diabetic retinopathy for ten years. Hepatitis C virus (HCV) related liver cirrhosis was diagnosed one year ago without antiviral therapy. He was referred to nephrologist for impaired renal function with foamy urine. He denied any history of gross hematuria, lower limbs swelling, loss of body weight, and no history of regular taking non-steroidal antiinflammatory drugs or indigenous medicine including chinese-herbs. Antihypertensive (Irbesartan150mg/ hydrochlorothiazide 12.5mg once daily, Lercanidipine-10mg once daily ) and oral hypoglycemic agents (Gliclazide MR 30mg once daily, Rosiglitazone 2mg/ Metformin 500mg once daily) were prescribed for hypertension and diabetic mellitus . On physical examination, the patient’s height was 162 cm, body weight was 61kg.and in no distress. His pulse rate was 98 beats/minute and regular rhythm, blood pressure was 177/106 mmHg, skin showed no rashes, lower limbs revealed no edema, without relevant positive finding on systemic examination. Laboratory findings showed serum creatinine level of 2.0 mg/dL; estimated glomerular filtration rate of 34.5ml/min, spot urine protein to creatinine ratio was 3.2. Lipid profile showed total cholesterol of 158 mg/dL, triglycerides 206 mg/dL, GOT-40 IU/L, GPT-48 IU/L. Urinanalysis revealed proteinuria (3+) and microscopic hematuria (red blood cell [RBC] 5-6/high power field). RBC cast was negative and renal echography was normal. cryoglobulin and anti-HCV antibody were positive, C3 was 89 (normal range: 79-152), C4 was 13 (normal range: 16-38).Other immunological markers were normal. The renal biopsy was performed to explain the persistent microscopic hematuria and declining renal function. The pathological features were showed as below. Questions: What is your clinical differential diagnosis for this patient? What lesions did you observe upon light and electron microscope (Fig-1, Fig-2, Fig-3)? What lesion did you observe upon electron microscope (Fig-4)? What is your final diagnosis? Figure legand Fig-1: hematoxylin and eosin stain, original magnification ×400; Fig-2: electron microscope, original magnification ×4000; Fig-3: electron microscope, original magnification ×40000; Fig-4: electron microscope, original magnification ×40000 Answer of Nephro Quiz 1. The differential diagnosis for this patient’s renal insufficiency and nephrotic range proteinuria included diabetic nephropathy, membranoproliferative glomerulonephritis, and membranous glomerulonephritis (MGN). 2. Light microscope revealed expansion of mesangial matrix and thickening of glomerular basement membrane (Fig-1) with normocellular glomerulus. Under electron microscope, there was effacement of podocyte foot process with microvillus transformation (Fig-3), electron dense particles are deposited in mesangial (Fig-2) and subepithelial areas especially segmental hump like distribution (Fig-3). These features imply secondary MGN (such as infection, medications, autoimmune, diabetic, malignancy, cryoglobulinemia related) rather than primary (1), in which electron dense particles are seen in subepithelial area. Even though, the most common HCV infection related nephropathy was membranoproliferative glomerulonephritis (2), in context of cryoglobulinemia. 3. Electron microscope showed tubulorecticular inclusion (Fig-4) in endothelial cell; which were characterized by small clusters of anastomosing tubule-like structures within cisternae of endoplasmic reticulum. It was not specific for any particular disease, may be clinically correlated with systemic interferon treatment or endogenous overproduction of interferon(3). Tubulorecticular inclusion frequently seen in glomerular endothelial cells and related with certain pathological conditions such as autoimmune disease, viral infection and renal transplant. Final diagnosis: Secondary membranous glomerulonephritis related to hepatitis C infection. REFERENCES 1. Markowitz, Glen S: Membranous Glomerulopathy :Emphasis on Secondary Forms and Disease Variants. Advances in Anatomic Pathology 2001; 8: 119–25. 2. Perico N, Cattaneo D, Bikbov B, Remuzzi G: Hepatitis C Infection and Chronic Renal Diseases. Clin J Am Soc Nephrol 2009; 4: 207–20. 3. An-Hang Y, Bing-Shi L, Ko-Lin K, et al: The clinicopathological implications of endothelial tubuloreticular inclusions found in glomeruli having histopathology of idiopathic membranous nephropathy. Nephrol Dial Transplant 2009; 24: 3419–25.