Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
Coronary artery disease wikipedia , lookup
Heart failure wikipedia , lookup
Cardiac contractility modulation wikipedia , lookup
Remote ischemic conditioning wikipedia , lookup
Myocardial infarction wikipedia , lookup
Management of acute coronary syndrome wikipedia , lookup
Jatene procedure wikipedia , lookup
Antihypertensive drug wikipedia , lookup
Electrocardiography wikipedia , lookup
Heart arrhythmia wikipedia , lookup
Dextro-Transposition of the great arteries wikipedia , lookup
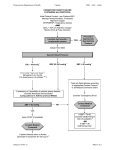
Systemic Blood Pressure and Heart Rate as Prognostic Indicators in Pulmonary Arterial Hypertension Malcolm M. Bersohn, MD, PhD;1 Shelley Shapiro, MD, PhD;1 Dave P. Miller, MS;2 Michelle P. Turner, MS;2 Glenna L. Traiger, RN, MSN;1 Adaani E. Frost, MD3 1 VA Greater Los Angeles Healthcare System and David Geffen School of Medicine at UCLA, Los Angeles, CA, USA; 2ICON Clinical Research, San Francisco, CA, USA; 3Baylor College of Medicine, Houston, TX, USA Introduction • Vital sign measurements such as resting heart rate and systemic systolic blood pressure (SBP) can predict survival in patients with congestive heart failure due to left ventricular systolic dysfunction.1,2 The extent to which these vital sign measurements alone serve as useful prognostic indicators in patients with pulmonary arterial hypertension (PAH) is being explored.3 • We hypothesized that, similar to patients with left ventricular dysfunction, a high or increasing resting heart rate and/or low or decreasing SBP would portend a worse prognosis in patients with PAH. • The Registry to EValuate Early And Longterm PAH Disease Management (REVEAL) is a large (54-center), ongoing, prospective, US-based observational study designed to provide current information about the demographics, course, and management of approximately 3500 patients with PAH. Patients have been enrolled and will be followed for ≥5 years from the time of enrollment.4 Results • At the first vital sign follow-up, SBP data were available for 2521 patients, heart rate data were available for 2497 patients, and SBP/heart rate ratio data were available for 2478 patients. • From enrollment to the first vital sign follow-up, data for changes in SBP were available for 2415 patients, change in heart rate data for 2367 patients, and change in SBP/heart rate ratio data for 2345 patients. • A sensitivity analysis was performed excluding those patients with PCWP >15 mm Hg, thus limiting analysis to those patients with traditional hemodynamic criteria of PCWP ≤15 mm Hg, and it did not have an effect upon the results. That implies that patients with PAH and mildly elevated PCWP are not different from other patients with PAH. Table 1. Survival and Freedom From Hospitalization 1 Year After the First Vital Sign Follow-up by Quintiles of Vital Signs and of Changes in Vital Signs Quintiles • To test the hypothesis that an increasing resting heart rate and a decreasing resting SBP between enrollment and the first vital sign follow-up visit are significant independent predictors of the time to first all-cause hospitalization and all-cause mortality 1 year after the first vital sign follow-up in patients with PAH enrolled in REVEAL. Study Design • Included in this analysis were consecutively enrolled newly or previously diagnosed patients with Group 1 PAH and aged ≥19 at enrollment with documentation of: –– Mean pulmonary artery pressure of >25 mm Hg at rest or >30 mm Hg with exercise –– Pulmonary capillary wedge pressure (PCWP) ≤18 mm Hg at rest or left ventricular end-diastolic pressure (LVEDP) ≤18 mm Hg –– Pulmonary vascular resistance (PVR) ≥240 dynes·sec·cm–5 • Patients were divided into quintiles according to the value of heart rate, SBP, and the ratio SBP/heart rate at the first vital sign follow-up visit and according to the changes in each variable between enrollment and the first vital sign follow-up visit, which occurred after a median of 3 months after enrollment. Q1 ≤102 ≤70 Q2-4 103-130 Q5 Survival Freedom from hospitalization Figure 5. One-year Freedom From Hospitalization by Resting Heart Rate at First Follow-up 100 95 90 85 80 ∆ SBP ∆ Heart Rate ≤1.2 ≤-12 ≤-10 ≤-0.2 71-95 1.2-1.7 -12 to 11 >130 >95 > 1.7 >11 >10 >0.2 2521 2497 2478 2415 2367 2345 Q1 83 ± 2 92 ± 1 80 ± 2 85 ± 2 90 ± 1 84 ± 2 Q2-4 91 ± 1 90 ± 1 91 ± 1 91 ± 1 90 ± 1 90 ± 1 Q5 91 ± 1 84 ± 2 93 ± 1 88 ± 2 86 ± 2 91 ± 1 Hazard ratio 1.9 1.5 2.1 1.3 1.2 1.3 P value <0.001 <0.001 <0.0001 0.006 0.09 0.01 Q1 62 ± 2 74 ± 2 60 ± 2 66 ± 2 70 ± 2 70 ± 2 N Q2-4 72 ± 1 70 ± 1 72 ± 1 72 ± 1 70 ± 1 69 ± 1 Q5 73 ± 2 66 ± 2 75 ± 2 71 ± 2 69 ± 2 74 ± 2 6-minute walk test distance (m), mean ± SD Hazard ratio 1.4 1.3 1.6 1.1 1.1 1.1 P value <0.001 <0.001 <0.001 0.06 0.35 0.11 Mean pulmonary artery pressure (mm Hg), mean ± SD -10 to 10 -0.2 to 0.2 • Patients in the highest quintile of resting heart rate (Q5: >95 bpm) had significantly lower survival at 12 months (84% ± 2%) than those in the other quintiles (Q1: 92% ± 1%, Q2-4: 90% ± 1%); hazard ratio = 1.5, Wald chi-square P < 0.001. Figure 3. One-year Survival by Resting SBP/Heart Rate at First Follow-up • Patients in the highest quintile of resting heart rate (Q5: >95 bpm) had a lower freedom from hospitalization at 12 months (66% ± 2%) than those in the other quintiles (Q1: 74% ± 2%, Q2-4: 70% ± 1%;); hazard ratio = 1.3, Wald chi-square P < 0.001. Figure 6. Freedom From Hospitalization by Resting SBP/Heart Rate at First Follow-up Figure 1. One-year Survival by Resting SBP at First Follow-up Table 2. Traditional PAH Risk Factors Across Quintiles According to Resting SBP, Heart Rate, and SBP/Heart Rate at First Follow-up SBP/Heart Rate (mm Hg/bpm) ≤1.2 >1.2–1.7 >1.7 2478 Q1 Q2–4 Q5 SBP (mm Hg) ≤102 >102–≤130 >130 2521 360 ± 125 373 ± 123 347 ± 123 Heart Rate (bpm) ≤70 >70–≤95 >95 2497 381 ± 120 366 ± 123 350 ± 129 Q1 Q2–4 Q5 51 ± 14 49 ± 14 47 ± 14 47 ± 15 49 ± 14 51 ± 15 51 ± 14 50 ± 14 46 ± 14 349 ± 133 372 ± 120 368 ± 124 SD, standard deviation. Results are mean ± SE; P value from Wald chi-square test comparing the worst quintile to the remaining quintiles. ∆ indicates first follow-up value - enrollment value. • Patients in the lowest quintile of resting SBP (Q1: ≤102 mm Hg) and the highest quintile of resting heart rate (Q5: >95 bpm) had significantly lower survival at 12 months and freedom from hospitalization at 12 months than those in the other quintiles. • Patients in the lowest quintile of resting SBP/heart rate (Q1: ≤1.2) had significantly lower survival at 12 months and freedom from hospitalization at 12 months than those in the other quintiles. • All of the vital sign parameters were better predictors of survival than freedom from hospitalization. • There were no significant differences among quintiles in freedom from hospitalization based on change in SBP/heart rate from enrollment to first follow-up; hazard ratio = 1.1, Wald chi-square P = 0.11. • Changes in SBP or heart rate from enrollment to first follow-up were not significant predictors of hospitalization. Q1 Q2–4 Q5 • Evaluation of other traditional prognostic indicators in PAH showed similarity across quintiles stratified according to the vital sign parameters. Conclusions • Patients in the lowest quintile of resting SBP/heart rate (Q1: ≤1.2 mm Hg/bpm) had significantly lower survival at 12 months (80% ± 2%) than those in the other quintiles (Q2-4: 91% ± 1%, Q5: 93% ± 1%); hazard ratio = 2.1, Wald chi-square P < 0.001. Figure 4. One-year Freedom From Hospitalization by Resting SBP at First Follow-up • Patients in the lowest quintile of resting SBP/heart rate (Q1: ≤1.2 mm Hg/bpm) had significantly lower freedom from hospitalization at 12 months (60% ± 2%) than those in the other quintiles (Q2-4: 72% ± 1%, Q5: 75% ± 2%); hazard ratio = 1.6, Wald chi-square P < 0.001. Figure 7. One-year Survival by Change in Resting SBP/Heart Rate From Enrollment to First Follow-up Statistical Analyses • Data lock was January 14, 2010. • Patients were included if they had at least one vital sign recorded (SBP and/or heart rate) at the first follow-up visit occurring within 1 year of enrollment and if they had at least 1 year of follow-up thereafter. A total of 2540 patients were included in the analysis. • Vital sign parameters were divided into quintiles to analyze survival and freedom from hospitalization one year after the first follow-up using Kaplan-Meier curves. • The results for quintiles 2–4 were similar and were combined in the final analysis. Log-rank analysis with a Bonferroni correction was used to assess differences (Bonferroni adjusted alpha = 0.017). • Hazard ratios were computed from univariate Cox regression models comparing patients in the worst quintile for the parameter to all others. Figure 8. One-year Freedom From Hospitalization by Change in Resting SBP/Heart Rate at First Follow-up ∆ SBP/ Heart Rate N Methods Objective SBP Heart Rate SBP/ Heart Rate Figure 2. One-year Survival by Resting Heart Rate at First Follow-up • Current values of vital signs were more useful than changes in vital signs in predicting mortality and hospitalization. The predictive value of vital signs at the first follow-up visit was similar to the predictive value of enrollment vital signs, which we have previously presented.3 Thus, the presence of hypotension and or tachycardia at any time predicts a worse clinical outcome. • High heart rate (>95 bpm), low SBP (≤102 mm Hg), and a ratio of SBP/heart rate ≤1.2 mm Hg/bpm identified high-risk groups of patients that had 50-100% increase in mortality and 30-60% increase in hospitalization over 1 year among a large group of adults with PAH. These simple vital sign parameters are useful by themselves and as part of a more comprehensive predictive formula.5 • These data reflect the similarity to left ventricular dysfunction, where low SBP and high heart rate are also predictive of poor outcome. Acknowledgments Funding for the REVEAL Registry and the development of this poster was provided by Actelion Pharmaceuticals US, Inc. Editorial assistance was provided by Kathryn Leonard of inScience Communications, a Wolters Kluwer business. References • Patients in the lowest quintile of resting SBP (Q1: ≤102 mm Hg) had significantly lower survival at 12 months (83% ± 2%) than those in the other quintiles (91% ± 1%); hazard ratio = 1.9, Wald chi-square P < 0.001. • Patients in the lowest quintile of resting SBP (Q1: ≤102 mm Hg) had significantly lower freedom from hospitalization at 12 months (62% ± 2%) than those in the other quintiles (Q2-4: 72% ± 1%, Q5: 73% ± 2%); hazard ratio = 1.4, Wald chi-square P < 0.001. • Patients in the lowest quintile of change resting SBP/heart rate (Q1: ≤-0.2 mm Hg/bpm) had lower survival at 12 months (84% ± 2%) than those in the other quintiles (Q2-4: 90% ± 1%, Q5: 91% ± 1%); hazard ratio = 1.3, Wald chi-square P = 0 .01. • Comparison with Figure 3 shows that the change in SBP/heart rate was not as strong a predictor as the SBP/heart rate at first follow-up. 1.Abraham WT, Fonarow GC, Albert NM, et al. Predictors of in-hospital mortality in patients hospitalized for heart failure: insights from the Organized Program to Initiate Lifesaving Treatment in Hospitalized Patients with Heart Failure (OPTIMIZE-HF). J Am Coll Cardiol. 2008; 52:347-356. 2.Levy WC, Mozaffarian D, Linker DT, et al. The Seattle Heart Failure Model: prediction of survival in heart failure. Circulation. 2006; 113:1424-1433. 3.Bersohn M, Shipiro S, Turner M, et al. Prognostic Value of Heart Rate and Systemic Blood Pressure in Pulmonary Arterial Hypertension. J Am Coll Cardiol. 2010; 55: A154.E1443. 4.McGoon MD, Krichman A, Farber HW, et al. Design of the REVEAL registry for US patients with pulmonary arterial hypertension. Mayo Clin Proc. 2008; 83:923-931. 5.Benza RL, Miller DP, Gomberg-Maitland M, et al. Predicting survival in pulmonary arterial hypertension: insights from the Registry to Evaluate Early and Long-Term Pulmonary Arterial Hypertension Disease Management (REVEAL). Circulation. 2010; 122:164-172.