Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
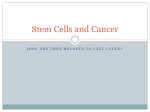
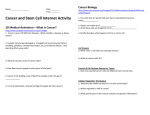
Supported by Boston Biomedical and Distributed as a Special Edition with the November 10, 2015 Issue of Oncology Times Cancer Stem Cells: Current Perspectives, Future Directions C ancer stem cells (CSCs) are becoming an increasingly greater focus of cancer research, as evidence suggests that they may be integral to tumor formation. Understanding the properties and characteristics of CSCs may lead to improvements in cancer diagnosis, therapy, and outcomes. This Special Edition, Cancer Stem Cells: Current Perspectives, Future Directions, distributed by Oncology Times, offers insight into the role of CSCs in tumor initiation, progression, and metastasis, as well as the signaling pathways implicated in cancer, with a focus on gastric and gastroesophageal cancers. The potential for inhibition of these signaling pathways is also reviewed. INSIDE Do Cancer Stem Cells Hold the Key to Controlling Cancer Growth and Spread? Interview with Max S. Wicha, MD Dr Wicha notes that greater understanding of CSCs may hold a key to controlling cancer and potentially achieving durable clinical responses to treatment............................................................................................................................ 2 Cancer Stem Cells: Lessons From Gastroesophageal Cancer Biology Interview with Jaffer A. Ajani, MD Dr Ajani discusses the role of CSCs in tumor development, relapse, and metastasis, as well as the challenges to clinical practice posed by advanced gastric cancer........................................................................................................................ 8 Cancer Stem Cells: Where We Are and Where We’re Going Dr Ajani and Dr Wicha answer questions about the current and future state of CSC research. ..................................................... 14 Supported by: Do Cancer Stem Cells Hold the Key to Controlling Cancer Growth and Spread? Interview with Max S. Wicha, MD Max S. Wicha, MD Distinguished Professor of Medical Oncology and Director Emeritus University of Michigan Comprehensive Cancer Center Ann Arbor, Michigan D espite advances in chemotherapy, targeted agents, and radiation therapy, the prognosis for patients with advanced cancer has remained poor.1 Drug resistance, metastasis, and recurrence—even after extended periods of remission—pose persistent challenges to cancer management.2 A growing body of evidence indicates, however, that a subset of cancer cells, called cancer stem cells (CSCs), may hold a key to controlling cancer and potentially achieving durable clinical responses.1 “Ultimately, patient survival depends on getting rid of these cancer stem cells—the seeds we see in the cancerous tumor after treatment,” said Max S. Wicha, MD, Distinguished Professor of Medical Oncology and Director Emeritus at the University of Michigan Comprehensive Cancer Center in Ann Arbor. CSCs Drive Tumorigenesis Normal stem cells are undifferentiated cells in the body that can self-renew, propagate differentiated cells, and proliferate extensively.3 Laboratory studies have shown that entire organs can be generated from a single stem cell.3 These discoveries have fueled interest in stem cell therapy for a wide variety of diseases, including neurological, inflammatory, and endocrine disorders.3 CSCs are malignant cancer cells that share the capacity of normal stem cells for self-renewal and proliferation and can differentiate into the heterogeneous population of cancer cells that comprise a malignant tumor,4 Dr Wicha explained. A common misconception is that all CSCs arise from mutated normal stem cells, but some CSCs may arise from progenitor cells when a mutation endows these cells with the capacity for self-renewal, normally reserved to stem cells (Figure 1).5,6 The CSC model of cancer formation is hierarchical, in contrast with the traditional stochastic model (see Models of Carcinogenesis on page 3).5,7 A growing body of evidence suggests that CSCs are the drivers not only of tumor initiation and heterogeneity, but of treatment resistance, cancer recurrence, and metastasis.8,9 While the idea that cancers can arise from stem cells goes back about 150 years,5 it was not supported by experimental evidence until the late 1990s. Bonnet and Dick showed that a small subset of acute myelogenous leukemia (AML) cells were capable of transferring AML into immunosuppressed mice. The proteins expressed on these cells were similar to those expressed on normal hematopoietic stem cells.10 A few years later, the role of CSCs in tumorigenesis in solid tumors was supported Models of Carcinogenesis The classical model of cancer formation, termed the stochastic model, defines tumor cells as biologically equivalent. Intrinsic factors, such as signaling pathways and levels of transcription factors, and extrinsic factors, such as the microenvironment, host-specific factors, and immune response, result in varied and unpredictable behavior of the tumor cells. Therefore, tumor-initiating activity cannot be attributed to any specific type of cells. Conversely, the hierarchy model proposes that tumors are made up of biologically distinct types of cells with varying functions and behaviors. Tumor growth can only be initiated by a subset of cells known as cancer stem cells (CSCs), which can self-renew and differentiate to nontumorigenic progeny that comprise the tumor mass (Figure).1 According to Max S. Wicha, MD, research suggests that both models are correct.2,3 “What we know now is that the CSCs themselves can mutate. As cancers develop, the CSC that started the tumor can then mutate and produce a new clone, and at the top of the clone is a CSC. There can be more than one CSC in an individual cancer. Therefore, in a way, the stochastic model and the CSC model are both correct: stem cells mutate and get selected out and each stem cell then generates a clone. Thus, within the tumor are multiple stem cells and multiple clones that come from these tumors.” 3 The stochastic and hierarchy models of tumor heterogeneity. The stochastic model holds that cancer arises through random mutation and clonal selection. Other clones can be selected out with treatment, but the cancers continually mutate. In this model, any cell can become cancerous.4 The CSC model, termed the hierarchy model, is at the other end of the spectrum. It holds that cancers originate only in cells that can self-renew and then produce the differentiated cells that make up the bulk of the tumor.4 1.Dick JE. Stem cell concepts renew cancer research. Blood. 2008;112:4793-4807. 2. Chen K, Huang YH, Chen JL. Understanding and targeting cancer stem cells: therapeutic implications and challenges. Acta Pharmacol Sin. 2013;34:732-740. 3.Chen S, Huang EH. The colon cancer stem cell microenvironment holds keys to future cancer therapy. J Gastrointest Surg. 2014;18:1040-1048. 4.Wicha MS, Liu S, Dontu G. Cancer stem cells: an old idea—a paradigm shift. Cancer Res. 2006;66:1883-1890. by the finding that human breast cancers also could be transferred to immunosuppressed mice by a small tumorigenic subset constituting only about 1% to 5% of the cancer cells.11 Figure 1. Stem cell development: normal and cancer stem cells (CSCs). Normal tissues develop from a central stem cell that grows and then differentiates to create progenitor and mature cell populations. Normal stem cells have the capacity to self-renew (shown by a curved green arrow), develop into mature tissue (shown by a variety of different color cells), and proliferate. CSCs develop via mutation of normal stem cells or progenitor cells. They go on to grow and differentiate to create primary tumors (the dashed line shows that it is unknown which specific types of progenitors are involved in the generation of CSCs). CSCs can self-renew, generate heterogeneous populations of daughter cells, and proliferate, just like normal stem cells.6 “We need different clinical endpoints in assessing clinical trials that are designed to target CSCs.” – Dr Wicha The finding that most cells in cancer tumors are nontumorigenic has important therapeutic implications, Dr Wicha noted. Cancer treatments that target the nontumorigenic cells will cause tumor regression; however, if they do not affect the CSCs or their signaling pathways, these cells will persist and potentially regenerate the tumor, resulting in relapse.11 One implication of this finding is that “current evaluation of treatment may be inadequate,” he pointed out. Treatment efficacy is based on tumor shrinkage, which is usually defined in the clinic as tumor shrinkage of at least 50%.5 “The problem with that traditional endpoint is that for the vast majority of cancers, tumor shrinkage does not translate to patients living longer,” Dr Wicha said. An explanation for this may be that tumor regression is a mark of the effect of a treatment on the bulk tumor cell population, rather than the CSCs.12 CSCs tend to be resistant to conventional cancer therapies, similar to the resistance to apoptotic therapies observed in normal stem cells.5 “An issue critical Oncology Times • November 10, 2015 • Cancer Stem Cells: Current Perspectives, Future Directions Oncology Times • November 10, 2015 • Cancer Stem Cells: Current Perspectives, Future Directions 2 to understanding why CSCs are treatment resistant is whether CSCs are discrete populations of cells in cancer or whether non-CSCs can revert to stem cells,” Dr Wicha said. Recently, breast cancer stem cells were shown to exist in two states: the epithelial-mesenchymal transition (EMT) state and the mesenchymal-epithelial transition state (MET). In the EMT state, the cells are relatively quiescent but localized at the invasive tumor front, from where they can disseminate via the bloodstream to distant sites and seed micrometastases. In the MET state, the cells are capable of extensive proliferation, growing new tumors.13 Both cell states are needed to form metastases, and evidence suggests that plasticity of breast CSCs allows them to transition from one state to the other.13 Stem Cell Divisions Predict Cancer Risk The incidence of cancer across different tissues varies widely, but the reason for these differences is unclear.14 For example, the lifetime risk for cancers in the alimentary tract varies by a factor of 24 (0.20% in the small intestine but 4.82% in the large intestine). Such differences cannot be explained fully by environmental or genetic factors, which account for only one-third of the risk variation.14 Recent evidence points to stem cells as the key to the differences seen among the incidences of cancer in different organs. Most cells in tissues are differentiated and short-lived; however, stem cells, with their capacity for self-renewal, are essentially “immortal.” Tomasetti and Vogelstein analyzed stem cells in different organs and the number of times these stem cells divide, because mutations can happen any time a cell divides; they found a close linear relationship between the number of stem cell divisions in, and the incidence of, cancer in that organ.14 “The findings of Tomasetti and Vogelstein have been misunderstood as attributing cancer to ‘bad luck,’” Dr Wicha said, “undercutting the role of stem cells in tumorigenesis.” However, the data are highly supportive of the origin of most cancers in stem cells. What the investigators state is that the majority of the differences in cancer risk can be attributed to “‘bad luck,’ that is, random mutations arising during DNA replication in normal, noncancerous stem cells.”14 In other words, mutations occur at a constant rate based on how often the cell divides. Based on the linear correlation of 0.804, 65% of the differences in cancer risk among different tissues can be explained by the total number of stem cell divisions in the tissues.14 However, mutations can be caused by other factors as well. “The best example of this is carcinogenic tobacco smoke,” he said. “In this case, the lung cancer incidence would be higher than expected from just the number of stem cell divisions in lung tissue because of the influence of the environmental carcinogen.” Target Selection May Be the Key to Effective Therapy During the self-renewal process, normal stem cells interact with their microenvironment (termed the stem cell niche) via tightly regulated signaling pathways. In the early stage of cancer formation, after the stem cell or progenitor cell receives its first mutation, these pathways become dysregulated, allowing the CSCs to expand in an abnormal fashion.5 “We are finding that CSCs are driven by a limited number of key pathways,” Dr Wicha said (Figure 2).8 CSCs also interact with other components of the cellular microenvironment, such as cytokines, growth factors, and stromal cells (Figure 3).1 “We are finding that CSCs are driven by a limited number of key pathways.” – Dr Wicha An expanded understanding of the key signaling pathways of CSCs and of the interactions of these cells with the tumor microenvironment is providing new insights into the mechanisms responsible for the resistance of CSCs to conventional cancer therapies and potential targets for new treatment approaches.8 Evidence has shown that not only are CSCs resistant to chemotherapy and radiation therapy, but that their number can actually be increased by these treatments.15 Figure 2. Key signaling pathways in cancer stem cells (CSC) development. Dysregulation of signaling pathways plays a crucial role in the ability of CSCs to self-renew and differentiate. Depending on the signaling pathway involved, CSCs gain the ability to initiate cancer formation or cause tumor recurrence.8 As Dr Wicha explained, evidence shows that cells being killed by chemotherapy secrete inflammatory mediators such as cytokines; some of these are interleukin (IL)-6 and IL-8, which then act to stimulate CSCs. Damage to normal tissue induces a similar response. Injured cells release the same cytokines, signaling the normal stem cells in the tissue to reproduce.16 “This is healthy when it occurs during normal tissue regeneration, but during treatment of cancer with chemotherapy CSC stimulation leads to their increase,” he added. Dr Wicha noted that new approaches to cancer treatment include targeting CSCs and their signaling pathways, such as Notch, Wnt, Hedgehog, and JAK/ STAT, which regulate the CSC internal circuitry. Cancer treatments may also target inflammatory cytokines, such as IL-6 and IL-8, which mediate the interaction between CSCs and the tumor microenvironment, he added. The blockade of IL-8 receptors as a potential treatment approach has been studied in breast cancer by Dr Wicha’s group and others.17 “Targeting some of the pathways involved in CSC self-renewal may not only stop CSCs from reproducing, but also lead to their differentiation into non–stem cells, thereby making them chemotherapy-sensitive,” Dr Wicha said. Evidence suggests that when IL-8 receptor blockers are used in combination with chemotherapy, the CSC population decreases to a greater degree than with chemotherapy alone, perhaps Figure 3. The interaction of CSCs with their microenviron- ment. CSCs exist within a microenvironment of stromal cells, immune cells, neighboring vasculature, and secreted factors that are produced by these cells. These elements create a niche where CSCs survive and propagate into the cells that define the tumor mass.1,5 because the CSCs are being prompted to differentiate and become sensitive to chemotherapy.17 Regarding the development of new cancer treatment strategies for cancer, it is important to remember that CSCs represent only a small fraction of the tumor cell population, Dr Wicha noted. If these cells are not killed, the tumor will regenerate. Even if the CSCs are destroyed, the non-CSCs that form the bulk of the tumor can, however, still undergo several rounds of cell division leading to spreading of the cancer. Therefore, for the treatment of advanced cancers, the optimal approach is thought to be a combination of a stem-cell targeting agent with a debulking agent that can destroy the large mass of the tumor cells. That debulking agent can be chemotherapy, for instance, because chemotherapy is effective at targeting the bulk cells, while CSCs are resistant to chemotherapy and radiation therapy.16 According to Dr Wicha, “When treating micrometastatic disease in the adjuvant setting, CSC-targeted therapy alone may be potentially curative. If we knock out the micrometastases, the cancer may not grow back.” For this reason, treatment strategies that target CSCs and the mechanisms responsible for the interaction between CSCs and their microenvironment may represent an important approach to improving patient outcomes.16 CSC Immunotherapy May Improve Outcomes New insights into the biology of CSCs and nontumorigenic cancer cells are providing the rationale for immunologic approaches to targeting CSCs. The gene expression profiles and expressed antigens displayed by CSCs and non-stem cancer cells differ. Immunotherapies that target the differentiated cancer cells that form the tumor bulk may not effectively target the antigens expressed by CSCs. In addition, CSCs themselves exhibit heterogeneity.1 Thus, molecular profiling of CSCs and cancer tumors and targeting of immunotherapy at heterogeneous CSC populations “represent one of the most exciting areas in cancer research. Specifically, targeted immunotherapy offers the potential for durable responses in patients with cancers who previously had few therapeutic options,” noted Dr Wicha. CSCs can evade the immune system even more efficiently than the differentiated cells forming the tumor bulk. For example, CSCs express high amounts of programmed death (PD)–ligand 1 (PD-L1). The PD1/ PD-L1 pathway (an immune checkpoint) is one of two recognized immunoinhibitory pathways that contribute to an immunosuppressive microenvironment that protects cancer cells from immune destruction.1 Thus, a current approach to the treatment of a variety 5 Oncology Times • November 10, 2015 • Cancer Stem Cells: Current Perspectives, Future Directions Oncology Times • November 10, 2015 • Cancer Stem Cells: Current Perspectives, Future Directions 4 of cancers focuses on combinations of such immune checkpoint blocking therapies, other immunotherapies (such as IL-6 or IL-8 inhibitors), and vaccines that target CSCs.1 “The vision for the future of cancer therapy is to base treatment selection on a complete molecular diagnosis of the tumor, including an evaluation of the stem-cell profile of that particular tumor,” noted Dr Wicha. From an analysis of the immune infiltrates of the tumor, it also will be possible to know whether the patient is mounting an immune response against the tumor. Dr Wicha believes that cancer treatment will move toward a combination approach– targeting the tumor bulk, CSC populations, and immune components. This will lead to “substantial, rather than merely incremental, gains in treating cancer. Most importantly, this future approach may offer a more durable patient response as opposed to an increase in survival of only 1 or 2 months.” New Therapies, New Challenges With new treatments come new challenges. As Dr Wicha explained, “The first challenge is to determine whether an agent that targets CSC pathways will be cytotoxic to normal stem cells, because they use the same pathways. Early trials must test low doses of these agents and escalate them carefully,” he said. “Several phase 1 trials have already shown that most agents targeting CSC pathways can be given effectively with relatively low toxicities and that, based on biopsies performed before and after treatment, the targets are being hit.” Going forward, researchers will analyze whether combining these agents with chemotherapy or immunologic agents will have the potential for increased side effects, such as inducing autoimmunity against the normal stem cells. “These investigations must proceed carefully,” he cautioned. “The second challenge is the need to rethink the use of traditional endpoints of tumor regression in clinical trials,” Dr Wicha noted. Because CSC-targeting agents do not cause tumor regression, he explained, investigators must work with the United States Food and Drug Administration to determine how to demonstrate conclusively that these agents provide a benefit. “What are the acceptable endpoints?” he asked. “What should we be measuring?” Obviously, phase 1 trials are designed to study potential agents that target CSC signaling alone, with careful monitoring of potential toxicity risks. Phase 2 studies will then assess chemotherapy alone compared with chemotherapy plus an agent targeting a CSC pathway. Potential endpoints in these studies will likely be time to develop new metastases, time to tumor progression, and progression-free or overall survival, rather than tumor regression. A neoadjuvant trial design that assesses the level of complete pathological response has great appeal for CSC research in a number of tumor types, Dr Wicha said. Complete pathologic response with neoadjuvant therapies is associated with a favorable outcome and has already led to the approval of a new agent to be used as dual anti-HER2 therapy in patients with HER2-positive breast cancer.18 Another possible endpoint in the neoadjuvant setting is the measurement of residual CSCs after treatment, as the presence of these cells after neoadjuvant therapy has been associated with a poor prognosis.15 The other technology receiving increased attention is the isolation of circulating tumor cells. As Dr Wicha explained, circulating tumor cells are highly enriched in stem cell markers in patients with breast cancer. Whereas 1% to 5% of cells are CSCs in primary cancers, studies have shown that closer to 30% to 50% of circulating tumor cells express stem cell markers.11,19,20 Circulating tumor cells may prove useful as biomarkers for patients in clinical trials; isolating and measuring circulating tumor cells may be a way to monitor patients and determine the efficacy of potential treatments.20 “The utility of these assays as predictive of outcomes must be proven in rigorous clinical trials,” Dr Wicha noted, “but this is the kind of research now being explored, as agents that target CSC pathways are increasingly used in the clinical research setting.” Conclusion CSCs as potential therapeutic targets may be instrumental in developing therapies that control cancer and allow for the achievement of durable clinical responses in patients. Expanded understanding of the biology of CSCs, their key signaling pathways, molecular diagnosis of tumors, and appropriate clinical trial endpoints will help in the development of agents targeting key signaling pathways. References 1.Pan Q, Li Q, Liu S, et al. Concise review: targeting cancer stem cells using immunologic approaches. Stem Cells. 2015;33:20852092. 2.Touil Y, Igoudjil W, Corvaisier M, et al. Colon cancer cells escape 5FU chemotherapy-induced cell death by entering stemness and quiescence associated with the c-Yes/YAP axis. Clin Cancer Res. 2014;20:837-846. 3.Liu Y, Yang R, He Z, Gao W-Q. Generation of functional organs from stem cells. Cell Regen (Lond). 2013;2:1. 4.Clarke MF, Dick JE, Dirks PB, et al: Cancer stem cells—perspectives on current status and future directions: AACR Workshop on cancer stem cells. Cancer Res. 2006;66:9339-9344. 5.Wicha MS, Liu S, Dontu G. Cancer stem cells: an old idea—a paradigm shift. Cancer Res. 2006;66:1883-1890. 6.Jordan CT, Guzman ML, Noble M. Cancer stem cells. N Engl J Med. 2006;355:1253-1261. 7.Dick JE. Stem cell concepts renew cancer research. Blood. 2008;112:4793-4807. 8.Chen K, Huang Y-H, Chen J-L. Understanding and targeting cancer stem cells: therapeutic implications and challenges. Acta Pharmacol Sin. 2013;34:732-740. 9.Tang DG. Understanding cancer stem cell heterogeneity and plasticity. Cell Res. 2012;22:457-472. 10.Bonnet D, Dick JE. Human acute myeloid leukemia is organized as a hierarchy that originates from a primitive hematopoietic cell. Nat Med. 1997;3:730-737. 11.Al-Hajj M, Wicha MS, Benito-Hernandez A, Morrison SJ, Clarke MF. Prospective identification of tumorigenic breast cancer cells. Proc Natl Acad Sci USA. 2003;100:3983-3988. 7 12.Korkaya H, Liu S, Wicha MS. Regulation of cancer stem cells by cytokine networks: attacking cancer’s inflammatory roots. Clin Cancer Res. 2011;17:6125-6129. 13.Liu S, Cong Y, Wang D, et al. Breast cancer stem cells transition between epithelial and mesenchymal states reflective of their normal counterparts. Stem Cell Reports. 2014;2:78-91. 14.Tomasetti C, Vogelstein B. Cancer etiology. Variation in cancer risk among tissues can be explained by the number of stem cell divisions. Science. 2015;347:78-81. 15.Lee HE, Kim JH, Kim YJ, et al. An increase in cancer stem cell population after primary systemic therapy is a poor prognostic factor in breast cancer. Br J Cancer. 2011;104:1730-1738. 16.Korkaya H, Liu S, Wicha MS. Breast cancer stem cells, cytokine networks, and the tumor microenvironment. J Clin Invest. 2011;121:3804-3809. 17.Ginestier C, Liu S, Diebel M, et al: CXCR1 blockade selectively targets human breast cancer stem cells in vitro and in xenografts. J Clin Invest. 2010;120:485-497. 18.Gianni L, Pienkowski T, Im Y-H, et al: Efficacy and safety of neoadjuvant pertuzumab and trastuzumab in women with locally advanced, inflammatory, or early HER2-positive breast cancer (NeoSphere): a randomised multicentre, open-label, phase 2 trial. Lancet Oncol. 2012;13:25-32. 19.Aktas B, Tewes M, Fehm T, Hauch S, Kimmig R, Kasimir-Bauer S. Stem cell and epithelial-mesenchymal transition markers are frequently overexpressed in circulating tumor cells of metastatic breast cancer patients. Breast Cancer Res. 2009;11:R46. 20.Lianidou ES, Markou A. Circulating tumor cells in breast cancer: detection systems, molecular characterization, and future challenges. Clin Chem. 2011;57:1242-1255. Oncology Times • November 10, 2015 • Cancer Stem Cells: Current Perspectives, Future Directions Oncology Times • November 10, 2015 • Cancer Stem Cells: Current Perspectives, Future Directions 6 Cancer Stem Cells: Lessons From Gastroesophageal Cancer Biology Interview with Jaffer A. Ajani, MD Jaffer A. Ajani, MD Professor Department of Gastrointestinal Medical Oncology University of Texas MD Anderson Cancer Center Houston, Texas Percent of Cases by Stage Unknown n Localized Loca (Unstaged) d) (Con (Confined to primary site) prim 26% 10% 29% 35% CSCs and the Role of the Microenvironment As defined by the American Association for Cancer Research Workshop on Cancer Stem Cells, a CSC is a cell within a tumor that possesses the capacity to selfrenew and to give rise to the heterogeneous lineages of cancer cells that comprise the tumor. Because they have an intrinsic ability to propagate tumor cells, CSCs are also referred to as “tumor-initiating cells” or “tumorigenic cells” (Table 1).4,5 The ability of stem cells to self-renew and give rise to multiple cell lineages is termed “stemness.”6 The microenvironment plays an important role in the support and development of CSCs. Essentially, CSCs exist within a microenvironment consisting of stromal cells, immune cells, neighboring vasculature, and secreted factors that are produced by these cells. These elements create a niche where CSCs can survive and subsequently propagate into the cells that comprise the tumor mass. As such, the niche may be considered to be a regulatory microenvironment where the stem cell–like characteristics of CSCs are nurtured to maintain their self-renewal and differentiation activities. Studies have shown that pathological alterations in normal microenvironments may produce tumor microenvironments that serve as CSC niches.4 Distant ant Regional Region (Cancer has metastasized) zed) (Spread to regional lymph nodes) n 5-Year Relative Survival 100 Tumor Progression and Metastasis As noted, gastric cancer is usually diagnosed at later stages. This may be because patients often do not exhibit symptoms until their disease has progressed, or their symptoms have been vague and attributed initially to causes other than cancer. “Patients with gastric cancer often have nonspecific symptoms for a long time. It is not unusual for them to see multiple doctors, until finally, when the diagnosis is made, the tumor is well established,” Dr Ajani said. “One of our biggest problems is that most patients have very advanced tumors when finally seen at our clinic. To me, that signals an older tumor, with many generations of evolved cancer cells and a great deal of resistance to therapy.” – Dr Ajani Research is pointing to the migration of CSCs from the primary tumor site as an underlying mechanism of tumor progression and metastasis. The clinical pattern of patients with metastatic disease bears this out, Dr Ajani said. “Often, we can’t find the metastatic tumors in patients who are treated initially with a curative intent,” he noted. “When the primary tumor is treated, whether with preoperative chemotherapy and/or chemoradiation followed by surgery, we observe several phenomena. The primary tumor is often resistant to therapy. We know from our experience, that the more resistant the primary tumor, the more metastatic potential it has. In other words, this aggressive biology, which is probably related to the number of CSCs (and evolved species of CSCs) present in the primary tumor or volume of the tumor, dictates metastatic potential,” he explained. In addition, although it may appear that local treatment has been successful, highly resistant metastatic disease often becomes apparent very quickly. 80 Percent G astric and esophageal cancers are, respectively, the third and sixth most common causes of cancerrelated deaths worldwide.1 During the past several decades, the incidence of these cancers has decreased. In the United States, the incidence has shifted rapidly from esophageal squamous cell carcinoma and distal gastric carcinoma to adenocarcinoma of the esophagus and proximal stomach.2 In essence, gastric and esophageal cancers are now being seen more commonly at the gastroesophageal junction.2 In the United States, gastric cancer is mostly diagnosed in later stages, when survival is at its poorest.3 Indeed, localized gastric cancer represents only about one quarter of all gastric cancer diagnosed in the United States (Figure 1).3 “The survival advantage provided by current therapies for patients with regional and metastatic disease is pitifully marginal,” Jaffer A. Ajani, MD, commented. Dr Ajani is Professor in the Department of Gastrointestinal Medical Oncology at the University of Texas MD Anderson Cancer Center in Houston. “Our research is now showing that cancer stem cells (CSCs) are central to the lack of success when we treat patients with gastric or esophageal cancer.” 65.4 60 40 29.9 20 0 21.3 4.5 LLocalized li d R Regional i l Distant Di t t Stage Unstaged U t d Figure 1. Percentage of cases and 5-year relative survival by stage at diagnosis: stomach cancer. Cancer stage at diagnosis determines treatment options and has a strong influence on the length of survival. The earlier stomach cancer is diagnosed, the better chance a person has of surviving 5 years after diagnosis. For stomach cancer, 26.0% and 29.0% of cases are diagnosed at the local and distant stage, respectively. Of note, the stage of disease is unknown at diagnosis in more than one-third of cases. The 5-year survival for localized stomach cancer is 65.4%, compared with 4.5% for distant stomach cancer.3 Table 1. Key Characteristics of Cancer Stem Cells (CSCs)4,5 Self-renewal CSCs serially transplant through multiple generations Differentiation CSCs generate symmetrical and asymmetrical cells Tumorigenicity CSCs can propagate tumor cells Specific surface markers Allow for separation of CSCs from non–stem cells Treatment Patterns Unfortunately, current treatments for gastric cancers provide only a marginal overall survival benefit, as Dr Ajani noted. The 5-year relative survival of all patients with gastric cancer is less than 30%.7 A recent study followed more than 600 patients with localized esophageal or gastroesophageal cancer after treatment with chemoradiation and/or surgery. Regardless of treatment, more than one-third of the patients developed distant metastasis less than 2 years after treatment.8 In a review of second-line therapy in advanced gastric cancer, the overall survival was only about 5 months in most patients.9 While antiHER2–targeted therapy is showing efficacy, Dr Ajani pointed out that only about 20% of gastric cancers and 30% of gastroesophageal cancers overexpress HER2.9 In a review of first-line therapy in patients with metastatic disease, the inclusion of an anti-HER2–targeted agent provided a modest increase in survival to slightly more than 1 year.9 Patients receiving anti-HER2 therapy eventually develop resistance as well, he added. Treatment resistance is usually due to crossactivation of the HER2 signaling pathway by other pathways, including insulin-like growth factor, c-MET, growth differentiation factor 15, and other members of the ERBB family. Moreover, hyperactivation of downstream HER2 pathway components, such as MAPK and PI3K/AKT, may further contribute to anti-HER2 therapy resistance.10 “There is a need for better targeted therapies,” Dr Ajani said. The molecular events involved in tumorigenesis have been explored to a great extent in many types of cancer, Dr Ajani said, but those involved in gastric and gastroesophageal cancers are not well understood10 (see The Molecular Side of Gastric Cancer on page 10). “The CSC phenomenon is seen repeatedly in the clinic,” Dr Ajani said, “but we’re not yet able to do anything about it.” He described three patterns of response and resistance observed in patients with advanced and metastatic tumors following first-line therapy. “In patients with gastroesophageal cancer, there is almost a 50% chance they will experience some reduction in tumor volume and improvement in their symptoms for a short time,” he said, “but after a few months, the cancer starts to grow.” Second-line therapy produces less reduction in tumor volume and for a shorter duration response. This supports some of the preclinical research demonstrating that the CSC population is enriched by cancer treatments, making the tumor more resistant, he added. A second pattern involves patients whose tumors exhibit primary resistance, according to Dr Ajani. These patients never experience tumor shrinkage even with 9 Oncology Times • November 10, 2015 • Cancer Stem Cells: Current Perspectives, Future Directions Oncology Times • November XX, 2015 • Cancer Stem Cells: Current Perspectives, Future Directions 8 “We have conducted a fair amount of research on tumors at the juncture of the esophagus and stomach. Our preclinical findings show that CSCs are central to lack of treatment success of these tumors.” – Dr Ajani Gastric and Gastroesophageal Biology and CSCs CSCs provide a rational explanation for the presence of tumor heterogeneity and the development and progression of cancer, Dr Ajani believes. As he explained, normal stem cells are the source of the propagation of the entire tissue in organs. They are capable of self-renewal, as well as multi-lineage differentiation. They can create an exact copy of themselves or produce progenies with limited renewal and differentiation potential. While normal stem cells possess long life spans, their differentiated progenies can possess limited life spans.11 As examples of these characteristics, Dr Ajani said that investigators have shown that a single breast stem cell can be used to create all the different types of cells that compose a functional breast tissue.12 Using mouse models, a similar phenomenon has been observed in gastric tissue. In addition, the stem cells that propagate the tissue in the inner lining of the stomach have been shown to survive for the majority of the life span of a mouse, that is, 48 weeks, while also producing mature stomach lining cells, mucous cells, that live for only a few days.13 The majority of human gastric cancers originate from the stomach mucosa.7 The Molecular Side of Gastric Cancer Gastric cancer is a heterogeneous disease with diverse molecular characteristics. Multiple experimental and clinical investigations have implicated a wide range of germline and somatic alterations that drive tumor progression.1 Recently, the Cancer Genome Atlas Research Network analyzed nearly 300 samples of previously untreated gastric and gastroesophageal cancer and grouped them into four major molecular subtypes.2 • T he Epstein-Barr Virus (EBV)–positive group, which made up 9% of gastric cancers. This group displays high prevalence of DNA hypermethylation, including promoter methylation of the tumor suppressor CDKN2A (p16INK4A). There is a high incidence of PIK3CA mutations, amplifications of several oncogenes, including ERBB2, and recurrent amplifications of chromosome p9 (leading to overexpression of PD L1/2 and JAK2).2 • T he microsatellite instability (MSI) group, which made up 22% of gastric cancers. This group is characterized by enrichment for microsatellite instability (MSI), including hypermethylation at the MLH1 promoter. The MSI subgroup exhibits mutations in many cancer “hotspots,” such as PIK3CA, ERBB3, ERBB2, EGFR, and overexpresses mitotic pathway components.2 The inner lining of the stomach is organized into a cryptlike structure, containing normal stem cells at the bottom, which is similar to that seen in the inner intestinal lining, but not as deep, Dr Ajani explained (Figure 2).14-17 Like other stem cells, gastric stem cells self-renew and produce the remaining components of the mucosa. Studies have shown that these stem cells depend on the Wnt/β-catenin pathway to maintain the number of stem and non-stem mucosa cells. Dr Ajani noted that the Wnt/β-catenin pathway is important for the embryonic development of stomach stem mucosa cells as well. These mucosa cells begin to form precancerous mucosa cells when the inhibiting component of the Wnt/β-catenin pathway, called adenomatous polyposis coli (APC), is removed from the stem cells.14 This suggests that CSCs may be involved in the initiation and progression of gastric cancer, he said. Other stemness signaling pathways have been implicated in esophageal cancer progression, as well. The Hedgehog (Hh) pathway, for example, is transiently upregulated in progenitor cells to induce proliferation after tissue injury. These stem cell progenitors are usually quiescent and return to this state after tissue regeneration via tight regulation of the Hh signaling pathway. Chemoradiation-resistant esophageal cancer has been shown to induce the Hh stemness signal pathway after treatment. Blockade of the Hh pathway components results in reversal of therapy resistance. This suggests that these tumors may be activating this regenerative signaling pathway to support tumor regrowth after injury or chemoradiation.18 A similar phenomenon was • T he genomically stable subgroup, which made up 20% of gastric cancers. This group exhibited mutations in CDH1 and in RHOA, a protein important in cell motility and the STAT3 signaling pathway.2 • The high chromosomal instability (CIN) group, which made up about 50% of gastric cancers. This subgroup is concentrated at the gastroesophageal junction.2 The CIN group exhibited hyperactivation of EGFR and other RAS-driven receptor tyrosine kinases, mutation of the tumor suppressor TP53, and high levels of aneuploidy.2 Chromosomal instability has been shown to be prevalent in several solid tumors, including those of the head and neck, testes, lung, and liver, as well as in gastric and gastroesophageal cancers. Fewer CINs are seen in melanoma, and even fewer in Wilms’ tumors.3 1. Wadhwa R, Song S, Lee JS, Yao Y, Wei Q, Ajani JA. Gastric cancer: molecular and clinical dimensions. Nat Rev Clin Oncol. 2013;10:643-655. 2. Cancer Genome Atlas Research Network. Comprehensive molecular characterization of gastric adenocarcinoma. Nature. 2014;513:202-209. 3.Rooney PH, Murray GI, Stevenson DAJ, Haites NE, Cassidy J, McLeod HL. Comparative genomic hybridization and chromosomal instability in solid tumours. Br J Cancer. 1999;80:862-873. Normal Crypt observed in gastric cancer in which chemotherapy-resistant cells exhibited increased CSC properties, along with an increase in the CSC marker BMI1. Depletion of BMI1 resulted in therapy sensitization.19 Chemotherapy resistance is also associated with increased levels of the CSC marker ALDH1. In research conducted by Dr Ajani’s group, expression of ALDH1 after chemoradiation therapy correlated directly with worse clinical response.20 Dr Ajani added that this suggests that CSCs may play an important role in chemoradiation therapy resistance. “Chromosomal instability-related cancers are more common in organs, such as the lungs, stomach, esophagus, head and neck, and skin, which are exposed to external factors. When they become cancerous, it’s because these malignancies are all carcinogendriven and they have a large number of DNA alterations. On the other hand, pediatric cancers and leukemia are more genetically driven and have very few alterations.” – Dr Ajani CSCs have been shown to play a role in gastric and gastroesophageal cancer metastasis, too. Helicobacter pylori infection has been shown to increase expression of epithelial-mesenchymal transition (EMT) markers during the progression from normal tissue to dysplasia to gastric cancer. An increase in CSC potential (marked by an increase in the Cancerous Crypt Normal gastric epithelium cells Myofibroblast cells Normal stem cells Cancer stem cells Tumor cell Inflammatory microenvironment cells Wnt the initial treatment option, nor do they fare any better with a second-line therapy. “We have lost many patients like that.” A third resistance pattern is one in which the patient has a mixed treatment response. Metastatic lesions in the liver, for example, will become smaller, Dr Ajani said, while those in abdominal lymph nodes will increase in size. “This is a curious phenomenon,” he said, “but we observe it frequently and it reflects intra-patient tumor heterogeneity.” Not only can tumors in different organs exhibit different molecular characteristics, but multiple metastases in the same organ can have different somatic profiles. “These are real problems in the clinic that we cannot control,” he added. “We need to know about the underpinnings of these phenomena.” Signaling/phenotypic gradient Figure 2. Gastric stem cells and tumor formation. Multipotent stem cells positioned at the base of the pyloric antrum gastric crypt support long-term renewal of gastric mucosa, and give rise to all cell lineages of the crypt.15,16 These normal stem cells express the leucine-rich repeat-containing G-protein coupled receptor 5 (Lgr5) stem cell marker,15 and are dependent on Wnt signaling to maintain their stem cell functions at the base of the gastric crypt.14 Loss of adenomatous polyposis coli in Lgr5 positive cells may be a driver of tumor formation.14 Inflammatory microenvironment components, such as fibroblasts, lymphocytes, mast cells, and macrophages, may support transformation of gastric stem cells to cancer stem cells.17 11 Oncology Times • November 10, 2015 • Cancer Stem Cells: Current Perspectives, Future Directions Oncology Times • November 10, 2015 • Cancer Stem Cells: Current Perspectives, Future Directions 10 stem cell and CSC marker CD44) has been observed, as well. The expression of these markers decreased a year after eradication of infection—a trend that persisted several years after eradication of the H. pylori. Together, this suggests that H. pylori infection promotes EMT in gastric cancer via CSC-mediated tumorigenesis.21 As discussed earlier, anti-HER2–targeted therapy has been shown to be effective in some patients with gastric cancer. Recently, the mechanism of acquired resistance to the anti-HER2–targeted agent trastuzumab in gastric cancer has been explored. Treatment of gastric cancer cells for 20 weeks with trastuzumab resulted in EMT induction in drug-resistant cells. This EMT induction was characterized by loss of E-cadherin (the hallmark of EMT) and ZO1, as well as overexpression of claudin-1, vimentin, β-catenin, ZEB1, Slug, and Snail.22 These drug-resistant cells also exhibited an aggressive tumor phenotype, including higher motility, invasion potential, tumor formation potential, and metastatic capacity.22 Furthermore, the drug-resistant cells exhibited other CSC properties, including higher sphere-forming capacity and expression of the CSC markers Oct4, CD133, and CD44.22 The increase in CSC potential was accompanied by down-regulation of the AKT signaling pathway and upregulation of the STAT3 pathway. The STAT3 pathway was activated by Notch-dependent autocrine secretion of interleukin 6.22 Conclusion Advanced gastric or gastroesophageal cancer remains one of the most difficult challenges in clinical practice. Research has shown that CSCs can initiate tumor development and play a significant role in tumor relapse and metastasis. Indeed, evidence is accumulating that treatments, such as chemotherapy and radiation, can increase the proliferation of CSCs. Investigations are underway into the molecular signaling pathways involved in tumor cell repopulation. The small subpopulation of CSCs in gastroesophageal and other solid tumors may be a rational treatment target. References 1.Centers for Disease Control and Prevention. Global cancer statistics. http://www.cdc.gov/cancer/international/statistics.htm. 2012. Accessed July 6, 2015. 2.Crew KD, Neugut AI. Epidemiology of upper gastrointestinal malignancies. Semin Oncol. 2004;31:450-464. 3.National Cancer Institute. Surveillance, Epidemiology, and End Results Program (SEER). SEER Stat Fact Sheets: Stomach Cancer. http://seer.cancer.gov/statfacts/html/stomach.html. Accessed August 3, 2015. 4.Clarke MF, Dick JE, Dirks PB, Eaves CJ, Jamieson CH, Jones DL, et al. Cancer stem cells−perspectives on current status and future directions: AACR Workshop on cancer stem cells. Cancer Res. 2006;66:9339-9344. 5.Han L, Shi S, Gong T, Zhang Z, Sun X. Cancer stem cells: therapeutic implications and perspectives in cancer therapy. Acta Pharm Sin B. 2013;3:65-75. 6.Wong DJ, Segal E, Chang HY. Stemness, cancer and cancer stem cells. Cell Cycle. 2008;7:3622-3624. 7.American Cancer Society. Stomach cancer: survival rates for stomach cancer, by stage. http://www.cancer.org/cancer/stomachcancer/detailedguide/stomach-cancer-survival-rates. 2015. Accessed August 11, 2015. 8.Shiozaki H, Sudo K, Xiao L, et al. Distribution and timing of distant metastasis after local therapy in a large cohort of patients with esophageal and esophagogastric junction cancer. Oncology. 2014;86:336-339. 9.Elimova E, Shiozaki H, Wadhwa R, et al. Medical management of gastric cancer: a 2014 update. World J Gastroenterol. 2014;20:13637-13647. 10.Wadhwa R, Song S, Lee JS, Yao Y, Wei Q, Ajani JA. Gastric cancer-molecular and clinical dimensions. Nat Rev Clin Oncol. 2013;10:643-655. 11. Passegué E, Jamieson CHM, Ailles LE, Weissman IL. Normal and leukemic hematopoiesis: are leukemias a stem cell disorder or a reacquisition of stem cell characteristics? Proc Natl Acad Sci USA. 2003;100(suppl 1):11842-11849. 12.Liu Y, Yang R, He Z, Gao WQ. Generation of functional organs from stem cells. Cell Regen (Lond). 2013;2:1. 13.Bjerknes M, Cheng H. Multipotential stem cells in adult mouse gastric epithelium. Am J Physiol Gastrointest Liver Physiol. 2002;283:G767-G777. 14.Barker N, Huch M, Kujala P, et al. Lgr5(+ve) stem cells drive self-renewal in the stomach and build long-lived gastric units in vitro. Cell Stem Cell. 2010;6:25-36. 15.Singh SR. Gastric cancer stem cells: A novel therapeutic target. Cancer Lett. 2013;338:110-119. 16.Schepers A, Clevers H. Wnt signaling, stem cells, and cancer of the gastrointestinal tract. Cold Spring Harb Perspect Biol. 2012;4:a007989. 17.Quante M, Wang TC. Inflammation and stem cells in gastrointestinal carcinogenesis. Physiology (Bethesda). 2008;23:350-359. 18.Sims-Mourtada J, Izzo JG, Apisarnthanarax S, et al. Hedgehog: an attribute to tumor regrowth after chemoradiotherapy and a target to improve radiation response. Clin Cancer Res. 2006;12:6565-6572. 19.Xu ZY, Tang JN, Xie HX, et al. 5-Fluorouracil chemotherapy of gastric cancer generates residual cells with properties of cancer stem cells. Int J Biol Sci. 2015;11:284-294. 20.Ajani JA, Wang X, Song S, et al. ALDH-1 expression levels predict response or resistance to preoperative chemoradiation in resectable esophageal cancer patients. Mol Oncol. 2014;8:142-149. 21.Choi YJ, Kim N, Chang H, et al. Helicobacter pylori-induced epithelial-mesenchymal transition, a potential role of gastric cancer initiation and an emergence of stem cells. Carcinogenesis. 2015;36:553-563. 22.Yang Z, Guo L, Liu D, et al. Acquisition of resistance to trastuzumab in gastric cancer cells is associated with activation of IL-6/STAT3/Jagged-1/Notch positive feedback loop. Oncotarget. 2015;6:5072-5087. Cancer Stem Cells: Where We Are and Where We’re Going 13 Max S. Wicha, MD, and Jaffer A. Ajani, MD Q A Why is cancer stem cell (CSC) research so important? Dr Wicha: Many of our current treatments don’t target CSCs effectively. If these cells are essentially the cells that cause regrowth of tumors after treatment and are the seeds that carry cancer metastasis, it will be necessary to get rid of these cells to really improve the outcome of cancer patients. Dr Ajani: We need to understand some of the properties of CSCs to learn how they can be overcome. In addition to being treatment-resistant, CSCs prefer a hypoxic environment. They don’t need much oxygen to survive and can remain dormant for quite some time. Research that improves our understanding of these characteristics may ultimately lead to depletion of CSCs in the tumor. Q A Why is the concept of targeting CSCs so attractive? Dr Wicha: A mutation that is driving a cancer sometimes is also driving the CSC. A good example is human epidermal growth factor receptor 2 (HER2) in human breast cancer. HER2 is a very potent driver of breast CSCs, and we think that’s why HER2-targeted therapies have been so successful. However, in some cancers where the epidermal growth factor receptor (EGFR) appears to be important, the benefit of EGFR inhibitor therapies appears to be short-lived. This may be because we’re selecting clones that are resistant to those therapies, but also because the stem cells in those tumors don’t depend on HER2 signaling but rather different pathways. Dr Ajani: Another aspect to consider is that if we can target CSCs effectively, we may reduce the tumor burden in patients. We may not be able to eradicate the tumor, but we can certainly reduce the tumor bulk. A tumor with fewer stem cells could become indolent. That’s what we hope we can do. Q A Do you think that all cancers will be shown to have CSCs as the key player? Dr Wicha: I think they do play a role in all types of cancers; however, the frequency of cells that are stem-like varies tremendously between different cancers. At one end of the spectrum are hematologic malignancies, where it looks like maybe 1 of 1,000 or 1 of 10,000 cells may be a CSC. The tumors that probably have the highest percentage of CSCs are melanoma. All tumors probably have CSCs within, but to understand these cells we must understand not only the biology of the cell but how it relates to the microenvironment, including the immune system, in our patients. Dr Ajani: The short answer to that question is yes; many researchers believe cancer originates in the stem cells and there is a nice explanation for that. In a cell with stem cell properties, damaging the deoxyribonucleic acid (DNA) could cause the cell to become malignant. However, if the DNA is damaged in a cell with no stem cell properties, the cell dies because it has a limited number of life cycles. If, for example, DNA damage occurs in 100 cells but only 1 of them is a stem cell, that cell will survive with the DNA damage and eventually accumulate more damage and become cancerous. Q A What should practicing oncologists know today about CSCs? Dr Wicha: Practicing oncologists will start seeing more clinical trials of CSCs and immunotherapies. The key is to follow very closely the results of these clinical trials because oncology is moving at a quicker pace than we’ve ever seen before. I think we’re going to see advances in the CSC area, with the potential for achieving much more durable responses. I would also encourage practicing oncologists to participate in these trials as members of cooperative groups. Understanding CSCs may help us to develop new approaches to cancer prevention. Some interventions, like weight reduction, diet, and exercise, may affect stem cells through inflammatory mediators, like interleukin (IL)-6 and IL-8. We know that IL-6 is an important driver of breast CSCs. Women with breast cancer who either lose weight or undergo an active exercise intervention program lower their levels of inflammatory cytokines, such as IL-6, by 50%. Dormancy of cancers is also an issue. In diseases like estrogen receptor–positive breast cancer, cancers can recur after 15 or even 20 years, and molecular analyses are able to show that the recurrent cancers share almost all the same mutations as the original cancers—that they’re actually the same cancer. How did this happen? We think that these are dormant CSCs. Normal stem cells can sit for long periods and become active only Oncology Times • November 10, 2015 • Cancer Stem Cells: Current Perspectives, Future Directions Oncology Times • November 10, 2015 • Cancer Stem Cells: Current Perspectives, Future Directions 12 after damage is sustained; CSCs may act the same way. This may be why a cancer recurs 1 or 2 years after a woman has a great trauma, like losing a spouse or being involved in an accident. This might not be a coincidence and may be related to dormant CSCs, which can be found on biopsies in the bone marrow and may present during times of extreme stress and inflammation. If that’s the case, it tells us that stress reduction and exercise are important, and that potentially there may be new ways in the future of administering a therapy and eradicating these dormant CSCs. This is just speculation at this stage, but it’s exciting to think about the possibilities. In addition, many of the practicing oncologists are members of cooperative groups. They will start seeing many more cancer stem cell trials be added, along with immunotherapy trials, giving them many more options for their patients who may be appropriate candidates. I would highly encourage practicing oncologists to participate in these trials. Dr Ajani: Oncologists in the community need to be aware of the ramifications of treating stem cells and non–stem cells. Certain cancers behave like an organ. For example, when skin is injured, normal adult stem cells are animated and cause the skin to heal. They repopulate and maintain the skin. The same phenomenon occurs with cancer. When CSCs are injured by chemotherapy, they will also automatically repopulate. Further, in patients with colon cancer, it has been shown that if all the CSCs are killed, some of the non– stem bulk tumor cells will reformulate and transform into CSCs. Most clinicians tend to focus on the non–stem cells when treating cancer. We use cytotoxic drugs against this proliferative group of cells and sometimes we have success, but most of the time they produce only a transient effect. Treatment success will occur when CSCs and non–stem bulk tumor cells are treated in unison. That is where we need to go. To learn more about cancer stem cells, visit: www.bostonbiomedical.com or scan EDU-NPS-0051 ©2015 Boston Biomedical, Cambridge, MA 02139. All rights reserved. Printed in USA/November 2015 NOTES: 15 Oncology Times • November 10, 2015 • Cancer Stem Cells: Current Perspectives, Future Directions Oncology Times • November 10, 2015 • Cancer Stem Cells: Current Perspectives, Future Directions 14 Now Available Cancer Stem Cells: The Promise and The Potential A Seminars in Oncology Supplement Despite advancements in treatment modalities, many patients with cancer experience tumor recurrence and metastasis at regional or distant sites. Evolving understanding of tumor biology has led to the hypothesis that tumors possess a stem cell– like subpopulation known as cancer stem cells (CSCs), which may be involved in driving pathogenesis and tumor propagation. This supplement updates clinicians on the accumulated evidence characterizing the role of CSCs in tumor initiation, heterogeneity, therapy resistance, recurrence and metastasis, and the potential for effectively treating patients by targeting these cells. Jaffer A. Ajani, MD Howard S. Hochster, MD Shumei Song, MD, PhD Ira B. Steinberg, MD The University of Texas MD Anderson Cancer Center Houston, Texas The University of Texas MD Anderson Cancer Center Houston, Texas Yale School of Medicine New Haven, Connecticut Boston Biomedical Cambridge, Massachusetts Published April 2015 Cancer Stem Cells: The Promise and The Potential http://education.seminoncol.org/stem-cell-qr Scan your smart phone over the QR Code to retrieve the COMPLETE article online. ©2015 Boston Biomedical, Cambridge, MA 02139. All rights reserved. Printed in USA/November 2015