Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
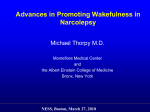
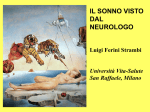
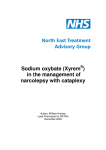
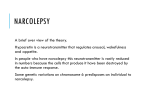
NARCOLEPSY A Randomized, Double Blind, Placebo-Controlled Multicenter Trial Comparing the Effects of Three Doses of Orally Administered Sodium Oxybate with Placebo for the Treatment of Narcolepsy The U.S. Xyrem Multicenter Study Group Study Objectives: To evaluate and compare the efficacy and safety of three doses of sodium oxybate and placebo for the treatment of narcolepsy symptoms. Design: A multicenter, double blind, placebo-controlled trial. Setting: N/A Participants: Study subjects were 136 narcolepsy patients with 3 to 249 (median 21) cataplexy attacks weekly. Interventions: Prior to baseline measures, subjects discontinued anticataplectic medications. Stable doses of stimulants were permitted. Subjects were randomized in blinded fashion to receive 3, 6, or 9 g doses of sodium oxybate or placebo taken in equally divided doses upon retiring to bed and 2.5-4 hours later for 4 weeks. Measurements and Results: Disease symptoms and adverse events were recorded in daily diaries. The primary measure of efficacy was the change from baseline in weekly cataplexy attacks. Secondary measures included daytime sleepiness using the Epworth Sleepiness Scale (ESS), inadvertent daytime naps/sleep attacks and nighttime awakenings. Investigators assessed changes in disease severity using Clinical Global Impression of Change (CGI-c). Compared to placebo, weekly cataplexy attacks were decreased by sodium oxybate at the 6 g dose (p=0.0529) and significantly at the 9 g dose (p=0.0008). The ESS was reduced at all doses, becoming significant at the 9 g dose (p=0.0001). The CGI-c demonstrated a dose-related improvement, significant at the 9 g dose (p=0.0002). The frequency of inadvertent naps/sleep attacks and the nighttime awakenings showed similar dose-response trends, becoming significant at the 9 g dose (p=0.0122 and p=0.0035, respectively). Sodium oxybate was generally well-tolerated at all three doses. Nausea, headache, dizziness and enuresis were the most commonly reported adverse events. Conclusions: Sodium oxybate significantly improved symptoms in patients with narcolepsy and was well tolerated. Key words: Sodium oxybate; gamma hydroxybutyrate; narcolepsy; cataplexy cult to identify, considerably fewer patients are actually diagnosed and treated. The primary cause remains unknown; however, recent human and animal data has provided strong evidence that the pathophysiology of narcolepsy involves the neuropeptide hypocretin (orexin).4 Hypocretin-containing neurons are found in the lateral hypothalamus where they project to various parts of the brain including nuclei believed to regulate sleep. Disrupting hypocretin neurotransmission, either at the level of the neurotransmitter5 or the receptor,6 results in animals exhibiting many of the classic symptoms of narcolepsy. This is supported by the fact that hypocretin is undetectable in cerebrospinal fluid in a large percentage of patients with narcolepsy.7 In addition, postmortem examination of brains from narcoleptics revealed a 85%95% decrease in hypocretin-containing cells.8 The excessive sleepiness associated with narcolepsy is commonly treated with stimulants, such as methylphenidate or dextroamphetamine,9 or with the wakefulness-promoting agent modafinil.10 While they improve daytime sleepiness and diminish cataplexy to a limited extent, they are not considered a principal treatment for cataplexy. The REM-related symptoms of cataplexy, sleep paralysis and hypnagogic hallucinations are typically treated with antidepressants of the tricyclic (TCA) or selective serotonin reuptake inhibiting (SSRI) classes.9 Hypnotics are sometimes prescribed to help maintain sleep at night. Unfortunately, there are disadvantages to these therapies as well. Tolerance to continuous stimulant therapy has been well established and their benefits may wane over time.9 The abrupt withdrawal of TCAs or SSRIs may result in a marked rebound of the REM-related symptoms.9,11 Most importantly, these conventional treatments do nothing to restore the integrity of sleep in INTRODUCTION NARCOLEPSY IS A DEBILITATING, LIFE-LONG CENTRAL NERVOUS SYSTEM DISORDER WHICH MAY FOLLOW A VARIABLE CLINICAL COURSE AND INCLUDE AN ARRAY OF SEEMINGLY UNRELATED SYMPTOMS. Narcolepsy usually begins with excessive daytime sleepiness and sleep attacks during the second and third decades of life. Other symptoms of the disease, including cataplexy, sleep paralysis and hypnagogic hallucinations may follow later. These added symptoms reflect the intrusion of REM sleep and its atonic motor component into normally wakeful periods. In time, sleep fragments and variable periods of non-REM and REM sleep may drift around the clock, alternating with periods of wakefulness.1,2 Although there are no universally accepted figures, the most commonly used estimate for the prevalence of narcolepsy in the general population is about 0.05%.3 As narcolepsy may be diffi- Disclosure Statement None of the U.S. Xyrem Multicenter Study Group Members have any significant financial involvement in any organization with a direct commercial interest in the subject discussed in the submitted manuscript. The research involved in this manuscript involves the use of an Investigational New Drug. This study was sponsored by Orphan Medical, Inc., Minnetonka, MN. Submitted for publication: August 2001 Accepted for publication November 2001 Address correspondence to: H. Cook, Orphan Medical, Inc., 13911 Ridgedale Drive, Suite 250, Minnetonka, MN 55305; Tel: 888-867-7426; Fax: 952-541-9209; E-mail: [email protected] SLEEP, Vol. 25, No. 1, 2002 42 Placebo-Controlled Multicenter Trial—U.S. Xyrem Multicenter Study Group narcoleptic patients.12 The administration of sodium oxybate, a unique endogenous neurotransmitter/neuromodulator,13 has been shown to improve the symptoms of narcolepsy and be well tolerated by patients. Its nocturnal administration appears to consolidate both REM and NREM sleep and diminish fragmented nighttime sleep14,15,16,17 resulting in improved daytime performance.14,15,16 To date, many narcolepsy patients have participated in numerous clinical trials with this agent.16,17,18,19 Two of these were small double blind, placebo-controlled crossover studies in which narcolepsy patients received nightly divided doses of 50-60 mg/kg for approximately one month. In both trials, sodium oxybate showed promise as a treatment of narcolepsy. GHB improved sleep quality and continuity,17,19 improved daytime sleepiness and decreased REM-related symptoms.19 Long-term experiences with open trials of sodium oxybate lasting as long as 20 months have also been described.15,20,21 These long-term studies demonstrated that sodium oxybate therapy alleviated the signs and symptoms of narcolepsy with no evidence of tolerance in doses ranging from 2.5 g-7 g nightly. The objectives of the present study were to evaluate and compare the safety and efficacy of three doses of sodium oxybate and placebo for the treatment of symptoms associated with narcolepsy. This washout period was used to train and habituate patients to the use of daily diaries. Patients were permitted to remain on stimulant medications provided stable doses were used beginning five days prior to baseline and continuing until the end of the trial. Of the 136 patients entering the trial, 113 (83.1%) remained on a stable dose of stimulant. Those patients not taking previous medications entered baseline following the five-day washout period. During a subsequent 14-21 day baseline period, patients recorded the frequency of cataplexy and other specified symptoms of narcolepsy in daily diaries. The daily patient diaries were developed with input from the FDA and included detailed descriptions of the symptoms to be recorded by each patient should they occur. Patients were instructed on the use of diaries by study coordinators and investigators and captured information on the primary outcome measures. These included the frequency of cataplexy events, number and duration of nocturnal awakenings, total amount of sleep each night, the number of hypnagogic hallucinations, and the incidence of sleep paralysis. In addition, they were used to document the occurrence of all adverse events. Patients were encouraged to utilize the daily diary every morning and evening. The use of daily diaries has previously been shown to be a satisfactory means for collecting patient response information in sleep medicine studies.22 Most patients exhibited moderate to severe cataplexy; however, a minimum of three cataplexy attacks per week during the last two weeks of the baseline period was required to enter the double-blind treatment phase of this study. At the beginning of the four-week treatment period, each patient randomly received 3, 6, or 9 g sodium oxybate or placebo nightly without titration. Sodium oxybate or placebo was administered in equally divided doses immediately upon retiring to bed and 2.5-4 hours later. When necessary, patients were encouraged to use an alarm clock to insure waking for the second nightly dose of sodium oxybate. Each patient received a telephone call from a trial center study coordinator after their first night on medication and three times weekly thereafter during the trial. All patients returned to their trial center after two and four weeks of treatment. Compliance with study protocol was assured by comparing the amount of medication remaining at each visit with the amount predicted to remain if the patient were compliant. Clinical assessments were conducted at the end of the fourweek trial period and three to five days after the study medication was discontinued. Patients who successfully completed this double-blind study were given the opportunity to enter a long-term open-label sodium oxybate trial. Daytime somnolence was assessed using the Epworth Sleepiness Scale (ESS) at study baseline and endpoint. The overall severity of disease was measured at baseline using the Clinical Global Impression of Severity (CGI-s) measure. The change in disease severity was assessed at endpoint with the Clinical Global Impression of Change (CGI-c) measure. During the study, patients used personal diaries to record the number of cataplexy attacks, number and duration of nocturnal awakenings, the total amount of sleep each night, the number of hypnagogic hallucinations, the incidence of sleep paralysis and adverse events. Safety assessment was conducted by reviewing daily diary entries, interviewing patients regarding possible adverse events, clinical laboratory studies, electrocardiogram and changes in METHODS Subjects This study included previously diagnosed narcolepsy patients who were 18 years of age or older and expressed a willingness to complete the entire study. Diagnostic criteria included a valid polysomnogram (PSG) within the previous five years and a current diagnosis of narcolepsy for at least six months based on criteria established by the American Sleep Disorders Association. This study excluded patients who were: diagnosed with sleep apnea or had coexisting causes of daytime sleepiness; taking hypnotics, anxiolytics, antidepressants (for depression), antihistamines, clonidine, or anticonvulsants; at risk of pregnancy; experiencing unstable disease states which placed them at risk during the study or any history of seizure disorder; history of psychiatric disorders which would preclude them from completing the study; at risk of substance abuse because of current or recent history of chemical dependency; shown to have serum creatinine greater than 2.0 mg/dL, aminotransferase values more than twice normal or a serum bilirubin more than 1.5 times normal; shown to have an abnormal electrocardiogram or history of recent myocardial infarction; taking medication for their narcolepsy other than a stable dose of stimulant for treating excessive daytime sleepiness; working in an occupation requiring variable shifts or routine night shifts. Treatments Following an initial screening visit, patients discontinued hypnotic medications and, over a four-week period, gradually withdrew from medications previously used to treat cataplexy symptoms to avoid rebound phenomena. This was followed by a fiveday washout period or five times the half-life of the discontinued anticataplectic medication up to 28 days, whichever was longer. SLEEP, Vol. 25, No. 1, 2002 43 Placebo-Controlled Multicenter Trial—U.S. Xyrem Multicenter Study Group Median change in cataplexy attacks per week from baseline to endpoint 5 0 -5 -10 -15 -20 -25 -30 -35 -40 Placebo 3g 6g 9g Figure 1—Median change in weekly cataplexy attacks at the end of the 4-week trial period (* denotes p=0.0008). For placebo, 3, 6 and 9 g groups, the median changes in the frequency of cataplexy attacks were –4.3, -7.0, -9.9 and –16.1, respectively. This change was significant across doses (p=0.0021), indicating a doserelated effect. Median percent change in cataplexy 0 -10 -20 Placebo (-28) -30 -40 3g (-49) -50 -60 6g (-49) -70 9g (-69) * -80 0 2 Time (weeks) 4 Figure 2—Median percent change from baseline for cataplexy attacks per week, by sodium oxybate dose. This change was significantly different across doses (p=0.021) and was significant at the 9 g dose (* denotes p=0.0008). These data also demonstrate the greatest improvement occurred during the first two weeks of therapy. placebo was performed using least-squares means with Dunnet’s adjustment. The significance of the median change from baseline for each treatment group was assessed using a paired t-test. Those measures that did display a normal distribution without log transformation included Epworth Sleepiness Scale, total amount of nighttime sleep, and number of inadvertent naps/sleep attacks per day. For these measures, the analysis was conducted on untransformed values. The CGI-c was assessed using CochranMantel-Haenszel Tests for Nonzero Correlation between the CGI-c score and treatment. For all measures, a level of significance was established at p<0.05. physical condition. Statistical Analysis The planned analysis called for ANOVA on the change from baseline to endpoint done on the intent-to-treat population. In addition, ANCOVA was planned for the primary efficacy variable (change in frequency of cataplexy attacks) using the baseline value as the covariate. In the event that the assumptions for ANCOVA were not satisfied, the planned analysis included logtransformation to provide a more normal distribution of the data. At the time of analysis, the Wilk-Shapiro test for normality indicated several measures required log transformation. These included the total number of cataplexy attacks, daily episodes of sleep paralysis and hypnagogic hallucinations, and number of nighttime awakenings. Comparison of sodium oxybate dose to SLEEP, Vol. 25, No. 1, 2002 Ethics Statement The Institutional Review Board for each of the 18 trial centers approved the protocol. Written informed consent was obtained 44 Placebo-Controlled Multicenter Trial—U.S. Xyrem Multicenter Study Group from each patient prior to initiation of the study. This study was conducted in accordance with the ethical principles delineated in the Helsinki Declaration of 1975, as revised in 1997. significance at the 6 g dose (p=0.0529) becoming highly significant at the 9 g dose (p=0.0008) when compared to placebo. RESULTS Daytime Sleepiness There were 136 patients enrolled in the study: 57 (41.9%) were male and 79 (58.1%) were female. The mean age was 43.1 years, mean height 170.9 cm and mean weight 82.9 kg. Caucasians comprised 124 (91.2%) of the patients, AfricanAmericans 9 (6.6%), Asians 1 (0.7%) and Other 2 (1.5%). At baseline, the frequency of weekly cataplexy attacks ranged from 3-249 (median 21). The study was completed by 120 (88%) patients. The demographics of each dose group were well balanced and there were no significant between-group differences except the 6 g group, which had a higher percentage of male (63.6%), and correspondingly taller, patients. There were no significant differences in the frequency of cataplexy, hypnagogic hallucinations, sleep paralysis, or inadvertent naps/sleep attacks between the different treatment groups during the three-month screening period or during baseline measures. At that time, cataplexy, excessive daytime sleepiness, and inadvertent sleep attacks occurred in virtually all patients. The ESS improved in all of the sodium oxybate treatment groups in a dose-related manner, becoming significant at the 9 g dose (p=0.0001) when compared to placebo. This improvement in wakefulness occurred even though the majority of patients remained on stable doses of stimulant medications. The median score at the 9 g dose dropped from 17.0 to 12.0, indicating that, for some patients at this dose, the subjective measure of sleepiness fell into the normal range (Epworth Scale <10).23 The data from all groups are graphically presented in Figure 3. Clinical Global Impressions of Change (CGI-c) The Clinical Global Impression of Change from baseline assessment of severity exhibited a significant difference across doses (p=0.0014), suggesting a dose-related response that became significant at 9 g (p=0.0002). These data are presented graphically in Figure 4. At the 9 g dose, 24 of 30 patients (80%) were either Much Improved or Very Much Improved after four weeks of nightly sodium oxybate therapy compared to 11 of 34 (32.4%) in the placebo group. Efficacy Cataplexy Other Parameters The baseline and endpoint cataplexy values for placebo and the three doses of sodium oxybate are shown in Figure 1. The administration of nightly sodium oxybate produced a decrease in the reported frequency of cataplexy attacks. Figure 2 also illustrates that this change was significant across doses (p=0.0021), representing a dose-related effect. This improvement approached There was a significant reduction in the number of inadvertent naps/sleep attacks seen at both 6 g and 9 g doses of sodium oxybate (p=0.0497 and p=0.0122, respectively). The 9 g dose also produced a significant decrease in nocturnal awakenings (p=0.0035). For each of these symptoms there was evidence of a dose-response relationship. The incidence of sleep paralysis Placebo 24 B 22 E 3.0g B E 6.0g B E 9.0g B E Epworth Sleepiness Score 20 18 Narcolepsy Range 16 14 12 10 8 Normal Range 6 Figure 3—Median change from baseline to endpoint in daytime subjective sleepiness represented by Epworth Sleepiness Scale (ESS), by sodium oxybate dose. The ESS improved in all of the sodium oxybate treatment groups, becoming significant at the 9 g dose (* denotes p=0.0001). The whiskers represent the first and third quartiles. Thus, 25% of patients fall into in the normal range (Epworth Scale <10) for the 6 and 9 g groups. SLEEP, Vol. 25, No. 1, 2002 45 Placebo-Controlled Multicenter Trial—U.S. Xyrem Multicenter Study Group Clinical global impression of change (%) 100 90 80 70 60 50 40 30 20 10 0 Placebo 3g 6g 9g Figure 4—Percent change from baseline to endpoint in Clinical Global Impression of Change (CGI-c). The CGIC-c exhibited a significant difference across doses (p = 0.0014). At the 9 g dose, 24 of 30 patients (80%) were either Much Improved or Very Much Improved after 4 weeks of nightly sodium oxybate therapy (* denotes p = 0.0002). Table 1—Adversie events by costart term Body System Costart Term Body as a whole Headache Infection Pain Digestive Vomit Nausea Nausea vomit Diarrhea Nervous Anxiety Confusion Dizziness Dream abnormality Sleep Disorder Thinking Abnormal Skin and appendages Sweat Urogenital Incontinence, urine Dysmenorrhea Placebo (N = 34) 3 gm (N=34) 6 gm (N= 33) 9 gm (N=35) p-value 7 (20.6%) 1 (2.9%) 2 (5.9%) 3 (8.8%) 3 (8.8%) 3 (8.8%) 5 (15.2%) 5 (15.2%) 4 (12.1%) 11 (31.4%) 0 7 (20.0%) 0.1141 0.0338 0.3382 0 2 (5.9%) 0 0 0 2 (5.9%) 0 0 2 5 2 2 (6.1%) (15.2%) (6.1%) (6.1%) 4 (11.4%) 12 (34.3%) 2 (5.7%) 2 (5.7%) 0.0475 0.0045 0.2594 0.2595 1 1 2 0 1 0 1 3 8 0 2 1 0 1 (3.0%) 10 (30.3%) 3 (9.1%) 4 (12.1%) 0 2 (5.7%) 5 (14.3%) 12 (34.3%) 1 (2.9%) 5 (14.3%) 2 (5.7%) 0.9021 0.2779 0.0178 0.0549 0.3195 0.6167 (2.9%) (2.9%) (5.9%) (2.9%) (2.9%) (8.8%) (23.5%) (5.9%) (2.9%) 0 1 (2.9%) 1 (3.0%) 4 (11.4%) 0.1567 0 1 (2.9%) 0 3 (8.8%) 2 (6.1%) 5 (15.2%) 5 (14.3%) 0 0.0143 0.0338 Selected adverse events by Coding Symbols for the Thesaurus of Adverse Reactions Terms (COSTART) term and sodium oxybate treatment group. Adverse events occurring with statistical significance (p<0.05) across doses are highlighted; term "incontinence, urine" actually reported as enuresis in most instances; term "sleep disorder" included prolonged sleep paralysis, sleep walking, poor sleep maintenance/frequent arousal, and microsleep. and hypnagogic hallucinations ranged from 74%-76% and 74%85%, respectively, across treatment groups. Although there was significant improvement within each treatment group receiving sodium oxybate (p=0.05), these improvements were not significant compared to placebo. SLEEP, Vol. 25, No. 1, 2002 Safety Adverse Events Most adverse events occurred within the first few days following the start of treatment and tended to decrease over time. Of the 16 patients who did not complete the trial, ten patients withdrew from the study due to the occurrence of an adverse event. All but one was considered to be mild or moderate in severity. 46 Placebo-Controlled Multicenter Trial—U.S. Xyrem Multicenter Study Group Total number of weekly cataplexy attacks 6g dose group 350 300 250 200 150 100 50 0 0 2 Time (weeks) 4 Figure 5—Mean change in cataplexy attacks per week by individual patients at the 6 g sodium oxybate dose exhibiting the aberrant effect seen in one patient. The adverse events believed to be related to sodium oxybate that occurred at a significant level and in a dose-related fashion included nausea, vomiting, dizziness, and enuresis (for each p<0.05). Adverse events are summarized in Table 1. Enuresis was reported as 15 single events in 8 of the 136 patients in the trial. One patient in the 6 g treatment group experienced a serious adverse event consisting of an acute confusional state. This occurred less than one week following the initiation of therapy, occurred in the afternoon following nighttime dosing on the previous evening and despite the extremely short half-life of the study medication. The patient was treated and recovered. The patient was discontinued from the study medication. During the three to five day washout period at the conclusion of the trial, there was an increase in the mean number of cataplexy attacks occurring in each treatment group, including placebo (actual numbers were extrapolated to seven days). A significant increase was seen in the 6 g group where the median number of cataplexy attacks increased from 8.0 to 16.3 (p=0.0001) but did not approach the mean baseline value of 23.0. A similar change was seen in the 9 g dose, increasing from 8.0 to 14.0 (p=0.0017; median at baseline 23.5). DISCUSSION Efficacy The data from this double-blind placebo-controlled study demonstrate that 3 to 9 g doses of sodium oxybate, taken nightly in equally divided doses at bedtime and repeated 2.5-4 hours later, produced clinical improvement in the symptoms of narcolepsy. These improvements occurred even though the dose of sodium oxybate each patient received was randomly assigned without consideration of patient size or severity of symptoms. Most importantly, sodium oxybate decreased the frequency of cataplexy, the primary outcome measure in this study. This effect was seen at the 3 g dose but became much more apparent at the 6 g and 9 g doses. This improvement in cataplexy is in agreement with several other studies, which have also demonstrated significant improvement in cataplexy after nightly administration of sodium oxybate (GHB).15,16,17,19 A single patient in the 6 g treatment group who reported 249 cataplexy attacks during the week of baseline measures, and 332 and 346 attacks after two and four weeks of therapy, respectively, seriously skewed the results as demonstrated in Figure 5. The patient may have been experiencing REM-rebound following discontinuation of prior anticataplectic medication. Re-evaluation of these results after removing this single patient from the data significantly altered the median number of cataplexy attacks to 7.75 (p=0.0327) at the 6 g dose. This modification results in data that are more consistent with previous reports where total nightly sodium oxybate doses of 50-60 mg/kg, corresponding to approximately 4.2 g or 4.7 g nightly, produced significant improvement in daytime cataplexy.17,19 Over the four-week treatment period, sodium oxybate in nightly 6g and 9g doses significantly improved daytime somnolence as reported by study patients and measured by the ESS. These doses also significantly reduced the reported number of inadvertent naps/sleep attacks during the day. It is noteworthy that these improvements occurred while patients remained on stable doses of stimulant medications. Laboratory Abnormalities The administration of sodium oxybate appeared to have no measurable effect on serum electrolytes, hematological measures, hepatic or renal function or electrocardiogram. A slight dose-related increase in urine pH (0.67 pH unit at the 9 g dose) was attributed to the increased sodium consumption associated with the study medication. Blood pressure remained unchanged. Abnormal laboratory findings were reported in 10 patients, however these were previously either present at baseline, occurred in placebo patients or resolved during the study, making a relationship with the study medication unlikely. SLEEP, Vol. 25, No. 1, 2002 47 Placebo-Controlled Multicenter Trial—U.S. Xyrem Multicenter Study Group Although the ESS does not correlate well with more objective measures of sleepiness, such as the maintenance of wakefulness test (MWT) or multiple sleep latency test (MSLT),24 it remains a valid assessment tool for daytime sleepiness23 and has been useful in measuring drug-induced changes in sleepiness in narcolepsy patients.25,26 Additional studies, which may confirm these results using MWT, are currently being conducted. The CGI-c indicate that investigators judged their patients to be Very Much Improved or Much Improved in more than half the patients in the 6 g and 9 g doses after four weeks of sodium oxybate therapy. These results compare very favorably with other recent pharmacological interventions, which improved the overall disease state of narcolepsy patients.25,26 Secondary measures of clinical improvement included decreased frequency and duration of reported inadvertent naps/sleep attacks that were significant at 6 g and 9 g doses. The reported number of nighttime awakenings was also significantly reduced at the 9 g dose. Together, these results confirm the observations of other investigators,15,16,17,19 and provide further evidence for a therapeutic role of sodium oxybate for the treatment of narcolepsy. and Wake Disorders, Chevy Chase, MD; N. Feldman, St. Petersburg Sleep Disorders Center, St. Petersburg, FL; M. Hagaman, Sleep Medicine Associates, Nashville, TN; G. Hertz, Center for Sleep and Insomnia Disorders, Huntington, NY; V. Iyer, Sleep Disorders Center University of Louisville Hospital, Louisville, KY; S. Kathawalla, Pulmonary Department Park Nicollet Clinic, Minneapolis, MN; D. Lankford, Sleep Disorders Center of Georgia, Atlanta, GA; M. Mitler and R. Hayduk, Pacific Sleep Medicine Services, La Jolla, CA; R. Pascualy, Providence Sleep Disorders Center, Seattle, WA; P. Sahota, University of Missouri Division of Neurology, Columbia, MO; T. Roth, Sleep Center Henry Ford Hospital, Detroit, MI; M. Scharf, Center for Research in Sleep Disorders, Cincinnati, OH; L. Scrima, Sleep-Alertness Disorders Center, Inc., Aurora, CO; J. Schwartz, Southwest Medical Center, Oklahoma City, OK; G. Zammit, Sleep Disorders Institute St. Luke’s—Roosevelt Hospital Center, New York, NY. The authors extend their deep appreciation to Dr. Merrill Mitler for his thoughtful review of this manuscript. Safety 1. Bassetti C, Aldrich MS. Narcolepsy. Neurol Clin 1996;14(3):545571. 2. Aldrich MS. Diagnostic aspects of narcolepsy. Neurology 1998; 50(Suppl 1):S2-S7. 3. Hublin C, Partinen M, Kaprio J, Koskenvuo M, Guilleminault C. Epidemiology of narcolepsy. Sleep 1994;17:S7-S12. 4. Seigel JM. Narcolepsy: a key role for hypocretins (orexins). Cell 1999; 98(4):1-20. 5. Chemelli RM, Willie JT, Sinton CM et al. Narcolepsy in orexin knock-out mice: molecular genetics of sleep regulation. Cell 1999;98(4):437-451. 6. Lin L, Faraco J, Li R et al. The sleep disorder canine narcolepsy is caused by a mutation in the hypocretin (orexin) receptor 2 gene. Cell 1999;98(3):365-376. 7. Nishino S, Ripley B, Overeem S, Lammers GJ, Mognot E. Hypocretin (orexin) deficiency in human narcolepsy. Lancet 2000;355(9197):39-40. 8. Thannickal TC, Moore RY, Niehuis R, et al Reduced number of hypocretin neurons in human narcolepsy. Neuron 2000;27(3):469-474. 9. Hublin C. Narcolepsy. Current drug treatment options. CNS Drugs 1996;5(6):426-436. 10. Fry JM. Treatment modalities for narcolepsy. Neurology 1998;50 (Supplement 1):S43-48. 11. Scharf MB, Fletcher KA, Jennings SW. Current pharmacologic management of narcolepsy. Am Fam Physician 1988;38:143-148. 12. Parkes JD, Fenton GW. Levo(-) amphetamine and dextro(+) amphetamine in the treatment of narcolepsy. J Neurology Neurosurg Psychiatry 1973;36:1076-1081. 13. Tunnicliff G: Significance of γ-hydroxybutyric acid in the brain. Gen Pharmacol 1992;23:1027-1034. 14. Broughton R, Mamelak M. Effects of nocturnal gamma-hydroxybutyrate on sleep/waking patterns in narcolepsy-cataplexy. Can J Neurol Sci 1980;7(1):23-30. 15. Scharf M, Brown D, Woods M, Brown L, Hirschowitz J. The effects and effectiveness of g-hydroxybutyrate in patients with narcolepsy. J Clin Psychiatry 1985;46(6):222-225. 16. Scrima L, Hartman PG, Johnson FH Jr., Hiller FC. Efficacy of gamma-hydroxybutyrate versus placebo in treating narcolepsy-cataplexy: double blind subjective measures. Biol Psychiatry 1989;26:331343. 17. Scrima L, Hartman PG, Johnson FH, Thomas EE, Hiller FC. The effects of g-hydroxybutyrate on the sleep of narcolepsy patients: a dou- REFERENCES Sodium oxybate appeared to be generally well tolerated. Adverse events reported in this study were consistent with expectations and affected primarily the central nervous and digestive systems. Most adverse events were relatively minor, occurred at the beginning of the study and abated over time. The incidence of nausea, vomiting, dizziness, and enuresis occurred with greater frequency at higher doses. Following abrupt discontinuation of sodium oxybate therapy there was no evidence of rebound phenomena. In addition, there was no evidence of tolerance to the beneficial effects of sodium oxybate. In summary, these data support and extend previous findings that demonstrate sodium oxybate is an effective treatment for the symptoms of narcolepsy. These improvements occur in a doserelated fashion and within a range of 6 g-9 g nightly, taken in equally divided doses at bedtime and 2.5-4 hours later. At the 9 g dose, statistically significant improvements were seen in the reported number of cataplexy attacks per week, the number of awakenings that occurred during the night, and the number of inadvertent naps during the day. In addition, significant improvement was seen in daytime sleepiness and the overall investigator assessment of disease severity. Significant clinical improvements in the frequency of cataplexy attacks and inadvertent naps were also reported at the 6 g dose. The results of a long-term, open label extension trial will provide data on the continued improvement in both cataplexy and excessive daytime sleepiness seen with chronic administration of sodium oxybate. Additional studies utilizing objective measures of narcolepsy symptom improvement are currently underway. Sodium oxybate appears to be a generally well-tolerated medication. ACKNOWLEDGMENTS The members of the U. S. Xyrem Multi-Center Study Group were J. Black and C. Guilleminault, Stanford Sleep Disorders Clinic, Stanford, CA; R. Bogan, Baptist Medical Center Sleep Disorders Center, Columbia, SC; H. Emsellem, Center for Sleep SLEEP, Vol. 25, No. 1, 2002 48 Placebo-Controlled Multicenter Trial—U.S. Xyrem Multicenter Study Group ble blind study. Sleep 1990;13(6):479-490. 18. Mamelak M, Escriu JM, Stokan O. The effects of gamma-hydroxybutyrate on sleep. Biol Psychiatry 1977;12(2):273-288. 19. Lammers GJ, Arends J, Declerck AC, Ferrari MD, Schouwink G, Troost J. Gammahydroxybutyrate and narcolepsy: a double- blind placebo-controlled study. Sleep 1993;16(3):216-220. 20. Broughton R, Mamelak M. The treatment of narcolepsy-cataplexy with nocturnal gamma-hydroxybutyrate. Can J Neurol Sci 1979;6(1):16. 21. Mamelak M, Webster P. Treatment of narcolepsy and sleep apnea with gamma-hydroxybutyrate: a clinical and polysomnographic case study. Sleep 1981;4(1):105-111. 22. Bastuji H, Jouvet M. Interet de l’agenda de sommeil pour l’etude des troubles de la vigilance. Electroencephalogr Clin Neurophysiol 1985;60:299-305. 23. Johns MW. Sensitivity and specificity of the multiple sleep latency test (MSLT), the maintenance of wakefulness test and the Epworth sleepiness scale: Failure of the MSLT as a gold standard. J Sleep Res 2000;9:5-11. 24. Sangal RB, Mitler MM, Sangal JM. Subjective sleepiness ratings (Epworth sleepiness scale) do not reflect the same parameter of sleepiness as objective sleepiness (maintenance of wakefulness test) in patients with narcolepsy. Clinical Neurophysiol 1999;110:2131-2135. 25. US Modafinil in Narcolepsy Study Group Randomized trial of modafinil for the treatment of pathological somnolence in narcolepsy. Ann Neurol 1998;43:88-97. 26. US Modafinil in Narcolepsy Study Group. Randomized trial of modafinil as a treatment for the excessive daytime somnolence of narcolepsy. Neurology 2000;54:1166-1175. SLEEP, Vol. 25, No. 1, 2002 49 Placebo-Controlled Multicenter Trial—U.S. Xyrem Multicenter Study Group