Survey
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
* Your assessment is very important for improving the work of artificial intelligence, which forms the content of this project
The Pathology of Pituitary
Doç. Dr. A. Işın DOĞAN-EKİCİ
Anatomy
• The anterior lobe develops from an evagination of
Rathke’s pouch (from the primitive oropharynx).
• The pituitary gland is located in the Sella Turcica in the
base of the skull.
• The anterior pituitary is one of the most vascularized
tissues in the body, due to its portal system.
• Secretion occurs in a 24 hr circadian rhythm .
• The functions of the pituitary gland are controlled by
factors produced in the hypothalamus.
Anatomy
The anterior lobe develops from an evagination
of Rathke’s pouch (from the primitive
oropharynx).
The pituitary gland is located in the Sella Turcica in the base
of the skull.
The anterior pituitary is one of the most vascularized
tissues in the body, due to its portal system.
Hypothalamic Hormones
Pituitary Hormones Affected
Somatotropin releasing factor
Somatotropin
Somatotropin releasing factor inhibitor
Somatotropin
Corticotropin releasing factor (CRH)
Corticotropin
Thyrotropin-releasing-factor (TRH)
Thyrotropin
(TSH)
Gonadotropin releasing hormone (GRH)
FSH and LH
Prolactin releasing factor (PRL)
Prolactin
Prolactin release-inhibiting factor
Prolactin
MSH releasing factor
Melanocyte-stimulating hormone
Topography of Hormone
producing cells in the pituitary
• The anterior hypophisis can be
subdivided into four parts:
• Two lateral wings................produce growth
hormone
• Medial portion:
• a)Medial posterior.................ACTH
• b)Medial Anterior..................TSH
Cell types Anterior Pituitary
• Classification by H&E Staining:
• Eosinophilic Cells:
• Somatotropes (growth hormone),
• Lactotropes (Prolactin)
• Basophilic Cells:
• Gonadotropes (FSH,LH)
• Thyrotropes (TSH)
• Corticotropes (ACTH)
• Melanotropes (MSH)
• Chromophob cells:
• No activity/Prolactin
• Crook’s hyaline -basophilic change in anterior pituitary cells in
Cushing’s Syndrome
Diseases of Pituitary
•
•
•
•
•
•
•
Hormone Production imbalances:
Impaired Synthesis or release
Abnormal target tissue interraction
Abnormal target tissue response
Mass Lesions:
Non-functioning
Functioning
DISEASES of the PITUITARY
GLAND
Clinical Classification
• Hyperpituitarism
• Hypopituitarism (Simmonds's disease)
Multiple endocrine neoplasia
syndromes
&
Hyperpituitarism
Multiple endocrine neoplasia
syndromes
• MEN 1 Syndrome (Werner's Syndrome)
• MEN 2a Syndrome (Sipple Syndrome)
• MEN 2b Syndrome (William Syndrome)
•Common autosomal dominant conditions which
predispose patients to certain endocrine tumors.
•Pre-natal diagnosis is available for these tumor-gene
syndromes.
MEN 1 Syndrome (Werner's Syndrome)
Hyperparathyroidism
90%
Pancreatic Islet Cell Tumors
60%
Gastrinoma
60%
Insulinoma
10%
Vipoma (Vasoactive Intestinal
Peptide-Producing Tumor)
PPoma (Polypeptidoma)
Glucagonoma
Pituitary Tumors
Prolactinoma
GH, ACTH, TSH secreting tumors
Thyroid adenoma
Adrenal adenoma
Carcinoid tumors
5%
MEN 2a Syndrome (Sipple Syndrome)
Medullary Thyroid Carcinoma 100%
Pheochromocytoma
50%
Hyperparathyroidism
10%
MEN 2b Syndrome (William Syndrome)
Medullary Thyroid Carcinoma
100%
Pheochromocytoma
50%
Multiple mucosal neuromas
100%
Ganglioneuromatosis of the gut
100%
Marfanoid appearance
100%>
Hyperpituitarism
• Too much of one (or may be two or more) of
the hormones from the adenohypophysis.
• This may be due either to:
• (1) autonomous over-production (tumors of the
adenohypophysis: adenoma/carcinoma; ~ 15% of all primary
intracranial tumors), or
• (2) excess production of hypophyseal
stimulating factors, or
• (3) Underproduction of inhibiting factors, or
• (4) Loss of inhibition following destruction of
other endocrine glands.
Tumors
ANTERIOR LOBE ADENOMAS
• Pituitary adenomas constitute 10% of all
diagnosed primary intracranial tumors.
• They can occur at any age,
• No great sex predominance.
• They are more common in patients with
autosomal dominant multiple endocrine
neoplasia (MEN) 1 (Werner's)
syndrome.
• Pituitary adenomas typically present as one or
more of the following:
• (1) Endocrine problems (both from hormones produced
by the tumor itself and from damage to the rest of the
adenohypophysis and/or the neurohypophysis)
• (2) Visual problems (from an expanding mass impinging
on the optic chiasm, i.e., bitemporal hemianopsia)
• (3) Enlarged sella turcica on skull x-rays (due to
expanding masses; large pituitary adenomas eventually
erode the sella, clinoid processes, diaphragma sellae,
optic nerves and chiasm, and even the cavernous
sinuses, nasal sinuses, or brain.
• (4) Increased intracranial pressure (i.e., headache,
nausea and vomiting).
• (5) Hemorrhage (Hemorrhage into a large pituitary
adenoma can produce pituitary apoplexy, which can
simulate a berry aneurysm rupture).
• (6) Infarct (Large tumors may also infarct themselves,
leading to remission or destruction of the remaining
normal gland as well).
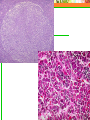
Microscopy:
Pituitary adenomas are typical endocrine adenomas,
i.e. they are composed of cuboidal cells, with round
nuclei and a good blood supply.
• Acidophilic adenomas (eosinophilic adenomas)
typically make growth hormone and/or prolactin.
• Basophilic adenomas typically make ACTH; less
often, they make TSH or the gonadotropins.
• Chromophobe adenomas nothing (null cell
adenoma) or may make prolactin.
Pituitary Adenomas
Immunocytochemical
Classification
Pituitary Adenomas
Causing Growth Hormone Excess
• somatotroph adenoma
• mammosomatotroph adenoma
Pituitary Adenomas Causing Prolactin Excess
• lactotroph adenoma
• psammoma bodies
• endocrine amyloid
• acidophilic stem cell adenoma
Somatotroph adenoma (GH)
Mammosomatotroph adenoma
Lactotroph adenoma
psammoma bodies
a pituitary stone :
extensive form of
psammoma bodies
Lactotroph adenomas produce endocrine amyloid that
stains with Congo red
Lactotroph adenoma: Intense diffuse positivity for
PRL throughout the cell cytoplasm
Acidophilic stem cell adenoma:
The acidophilia is attributable to mitochondrial accumulation,
considered to be a form of oncocytic change
Pituitary Adenomas Causing Thyrotropin
Excess (TSH)
Pituitary Adenomas Causing ACTH Excess
(ACTH)
• corticotroph adenoma
• crook's cell adenoma
Pituitary Adenomas Causing Gonadotropin
Excess (FSH)
Clinically Nonfunctioning Pituitary Adenomas
• silent somatotroph adenomas
• silent thyrotroph adenomas
• silent lactotroph adenomas
• silent corticotroph adenomas
• silent gonadotroph adenomas
• poorly differentiated adenomas
Plurihormonal Adenomas
Pituitary Carcinoma
GROSS APPEARANCE
CLINICAL VARIANTS
CHARACTERIZATION
Adenomas causing
GH excess
Acromegaly or gigantism
Usually diagnosed early because of the clinical
syndrome
GH and PRL
Often associated with acromegaly and are the most
frequent cause of gigantism
PRL
Amenorrhea and galactorrhea
TSH
Less than 1% of adenomas
ACTH
Cushing's disease-accounts for 2/3 of the cases of
Nelson's syndrome
Gonadtropin (FSH/LH)
In general, clinical evidence of excess hormones is
rare and tumors usually present with symptoms
secondary to the mass effects of the tumor
In young women, may present as primary ovarian
failure.
Radiology
• Prolactinoma (30%)
• Men: impotence, loss of libido
• Women: amenorrhea, loss of libido, infertility
• Both: Obesity, Galactorrhea
• Growth hormone adenoma (20%)
• Children: gigantism
• Adults: acromegaly
• Corticotroph cell adenoma (ACTH; 15%)
• Cushing's disease
Hyperprolactinemia
• (1) Functioning Prolactinomas
• (2) Hypothalamic tumors (Stalk effect)*
• craniopharyngiomas,
• gliomas,
• hypothalamic germinomas
*Stalk effect: This may be seen with any disease within
or near the pituitary gland and stalk that interferes
with the delivery of dopamine (a neurotransmitter)
from the hypothalamus to the prolactin secreting cells
of the pituitary. Therefore, other types of pituitary
adenomas, craniopharyngiomas or other tumors or
masses may cause modest elevations in prolactin.
• (3)Medications
• neuroleptics,
• antidepressants
• alfa-methyldopa.
• (4) Other causes of Hyperprolactinemia
• pregnancy or in the post-partum period
• stress (discomfort, exercise, low blood sugar)
• low thyroid function (hypothyroidism)
• kidney failure
• liver failure.
Gigantism & Acromegaly
• Overproduction of growth hormone causes excessive
growth.
• In children: gigantism
• In adults: acromegaly.
Gigantisim
• hormone production starts before the growth plates
have closed
• the long bones grow enormously.
• great stature, and the arms and legs lengthen
• hypogonadism (delayed puberty, genitals may not
develop fully).
Acromegalia
•
•
•
•
•
•
•
•
•
•
•
•
prognathism
huge brows
huge tongue
huge hands (with "spade fingers")
develops a deep guttural voice
oily skin (extra sebaceous glands), odor
joint deformities (degenerative arthritis)
barrel chest
secondary diabetes
sleep apnea
cardiomegaly
irregular menstrual cycles and galactorrhea.
Cushing's disease
• Excessive cortisol levels in the blood
• Etiology
• tumors of the pituitary gland (~70%),
• tumor/hyperplasia* of the adrenal glands
• ectopic ACTH producing tumors (lung: small cell ca)
• Production of ACTH by a pituitary tumor
• ACTH-oma: usually small microadenomas
• Nelson’s syndrome
*Most cases of "idiopathic adrenal hyperplasia" are due to ACTH-omas.
• Nelson’s syndrome (people who have both their
adrenal glands removed for Cushing's disease
therapy may develop Nelson's syndrome; ~20%):
• A Pituitary tumor producing: large amounts of
corticotrophin and MSH (hyperpigmentation of the skin)
• Compress effects of the tumor mass:
• headache,
• defects in vision,
• hypopituitarism (pressure atrophy).
Clinical findings
• Weight gain
• in face (moon face),
• above the supraclavicula
• on back of neck (buffalo
hump)
• thickened trunk
• Skin findings
• easy bruising,
• purplish stretch marks (stria)
• red cheeks (plethora)
• hirsutism (face, neck, chest,
abdomen, and thighs
• Generalized weakness and
fatigue
• Wasting of musculature
• Menstrual disorders in women
(amenorrhea)
• Decreased fertility and/or
libido
• Hypertension
• Diabetes mellitus
• Osteoporosis
• Kidney stones
• Depression, mood and
behavior disorders
Adrenal adenoma in Cushing's disease
Hypopituitarism
Hypopituitarism (Simmonds's disease)
• Loss of one or more (often all) of the
hormones from the adenohypophysis
• Panhypopituitarism indicates loss of
most or all of the hormones of the
adenohypophysis.
Etiology of the Hypopituitarism
• Causes affecting primarily the pituitary
gland:
• Empty sella syndrome
• Pituitary tumors (adenoma,
craniopharyngioma, metastasis)
• Inadequate blood supply (severe bleeding,
thrombus, anemia) infarction
Sheehan’s syndrome
• Infections and inflammatory conditions
(mycosis, Tb, syphilis, sarcoidosis)
• Amyloidosis
• Irradiation
• Surgical removal of the gland
• Autoimmune pathology (Lymphocytic
hypophysitis: rare; most patients are
postpartum women).
• Causes affecting
primarily the
hypothalamus:
• Tumors of the
hypothalamus
• Inflammatory
conditions
• Head injuries
• Surgical damage
Pituitary tumors (adenoma,
craniopharyngioma, metastasis)
Inadequate blood supply (severe
bleeding, thrombus, anemia)
infarction Sheehan’s syndrome
Pressure atrophy
Panhypopituitarism
• Clinical findings:
•
•
•
•
•
•
•
•
weight loss
lack of tanning
sexual dysfunction
weakness, easy fatigability
lack of resistance to stress
axillary and pubic hair loss
low blood pressure
disturbance of visual fields.
Empty sella syndrome
• Pressure atrophy
• Slow crushing of the gland by CSF pressure
• Some of these patients develop pituitary
insufficiency.
• Other reasons:
• old Sheehan's syndrome
• total necrosis of an old adenoma
• previous surgery.
Sheehan's pituitary necrosis
(Postpartum pituitary necrosis)
• Occurs when shock complicates a
problem delivery
• The drop in blood pressure
• results in inadequate blood supply to the gland
(its vessels squeezed half-shut).
• Sickle cell disease
• Temporal arteritis
• Trauma.
PITUITARY DWARFISM
• Failure to produce normal amounts of growth
hormone in childhood results in miniature, wellproportioned people.
• Idiopathic
• Genetic syndromes
• Laron dwarves
• short, frontal bossing
• the defect is in the growth hormone receptors
• Pygmies (pituitary dwarfism type II)
• tissues that do not respond well to growth hormone.
Growth Hormone Deficiency (in
childhood):
• in men:
• a lack of growth hormone
• atrophy of the testes
• leads to poor overall growth
• decreased sperm production
• short height (dwarfism).
infertility
Deficiency of Gonadotropins (follicle• loss of some male sexual
stimulating hormone and
characteristics.
luteinizing hormone):
• in premenopausal women:
Kallmann's syndrome :
• amenorrhea,
Deficiencies of luteinizing
• infertility
hormone and folliclestimulating hormone
• vaginal dryness
-a cleft lip or palate
• loss of some female sexual
characteristics.
-color-blind,
-unable to sense smells.
Thyroid-stimulating
Hormone
Deficiency:
Underactive thyroid gland
(hypothyroidism)
• confusion,
• intolerance to cold,
• weight gain,
• constipation,
• dry skin,
• partial anodontia.
Corticotropin
Deficiency:
Underactive adrenal gland
(Addison's disease)
• fatigue,
• low blood pressure,
• low levels of sugar in the
blood
• low tolerance for stress
• can be fatal.
Prolactin Deficiency:
reduces or eliminates lactation
• Sheehan's syndrome
• rare complication of childbirth
• excessive blood loss and shock
during childbirth pituitary
infarction inability to produce
breast milk (lactation)
• fatigue,
• loss of pubic and underarm hair.
Polyglandular deficiency syndromes
Hereditary or Autoimmune
disorders
Type 1 (in children):
Type 2 (in adults):
• Underactive glands:
• Underactive glands:
• Parathyroids
• Adrenals
• Complications:
•
•
•
•
•
•
Diabetes
Hepatitis
Gallstones
Malabsorption
Fungus infections
Hair loss
• Thyroid
• Adrenals
• Complications:
• Diabetes
Type 3 (in adults):
• Underactive glands:
• Thyroid
• Complications:
• Diabetes
CRANIOPHARYNGIOMA
• Benign tumor of Rathke's pouch remnants
• Occurs just above the pituitary and sella
turcica
• It is locally aggressive but does not
metastasize
• like the closely-related ameloblastoma of the jaws
• The optic nerves and chiasm, and then the
hypothalamus, are damaged.
• Most patients are under twenty, but no strict age
predilection.
• Grossly, the tumor is usually filled with little cysts which
contain an unsavory, cholesterol-rich fluid ("machine
oil").
• Microscopically, the tumor generally recalls
• developing tooth enamel,
• with areas of columnar cells (ameloblasts),
• stellate mesenchyme,
• calcification,
• sometimes stratified squamous stuff and/or bone.
Posterior Lobe Diseases
• Posterior lobe secretes:
• Antidiuretic hormone (ADH) which acts in the
kidney to retain fluid.
• Oxytocin
• Most common pathology is:
• ADH deficiency causes Diabetes
Insipidus
DIABETES INSIPIDUS
• Polyuria, polydipsia and dehydration
• can't concentrate urine
• Causes within the sella
•
•
•
•
•
compression by pituitary adenoma
pituitary infarction from any cause
pituitary ablation (surgical, radiation)
sarcoidosis
mutant ADH (autosomal dominant; or acquired in
chronic lithium administration or other serious renal
medullary disease).
• Causes above the sella
•
•
•
•
•
•
•
•
old bacterial meningitis
damage from encephalitis
meningeal tuberculosis
hypophyseal glioma or germinoma
craniopharyngioma
metastatic cancer
skull trauma/fracture
nephrogenic diabetes insipidus (the inability of the
kidney to respond to ADH).
SYNDROME OF INAPPROPRIATE ADH
PRODUCTION
Almost always due to :
• ectopic ADH production by a tumor
•
•
•
•
oat cell carcinoma
carcinoid,
thymoma,
lymphoma
• widespread pulmonary Tbc
• produces excess ADH.
PITUITARY-HYPOTHALAMIC
SYNDROMES
• These result from abnormal function of
the hypothalamus, reflected in problems
with sexual development.
• Fröhlich's syndrome (adiposogenital
dystrophy) is hypothalamic
hypogonadism + obesity.
•
•
•
•
Affected boys are obese
show a female pattern of fat distribution,
dwarfism
retarded sexual development.
• Bardet-Biedl syndrome (LaurenceMoon-Biedl")
• retinitis pigmentosa,
• polydactyly,
• similar picture to Fröhlich's.
• Kallmann's syndrome
• a brain malformation with anosmia (no
sense of smell)
• Fröhlich's findings.
• McCune-Albright syndrome
• with cutaneous café-au-lait ("coffee with
milk") spots,
• polyostotic fibrous dysplasia,
• precocious puberty,
• caused by a curious hypothalamic
hamartoma that produces LH-releasing
hormone.
• Septo-optic dysplasia
• multiple birth defects including several
malformations of the forebrain.
PITUITARY NON-DISEASES
• Little pituitary infarcts
• common in patients who die with intracranial
problems.
• Crooke's hyaline change
• dense cytoskeleton in pituitary cells which
ordinarily make ACTH, when they have suffered
chronic suppression by exogenous glucocorticoid
administration:
• Iatrogenic,
• from an autonomous adrenal adenoma (Cushing’s).