Survey
* Your assessment is very important for improving the workof artificial intelligence, which forms the content of this project
West Nile fever wikipedia , lookup
Oesophagostomum wikipedia , lookup
Hepatitis C wikipedia , lookup
Middle East respiratory syndrome wikipedia , lookup
Leptospirosis wikipedia , lookup
Trichinosis wikipedia , lookup
African trypanosomiasis wikipedia , lookup
Schistosomiasis wikipedia , lookup
Orthohantavirus wikipedia , lookup
Henipavirus wikipedia , lookup
Microbicides for sexually transmitted diseases wikipedia , lookup
Marburg virus disease wikipedia , lookup
Sexually transmitted infection wikipedia , lookup
Human cytomegalovirus wikipedia , lookup
Hepatitis B wikipedia , lookup
Hospital-acquired infection wikipedia , lookup
Neonatal infection wikipedia , lookup
Herpes simplex wikipedia , lookup
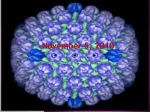
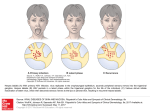
Accurate Info for Patients Version 1.1 (Sept 2016) Genital herpes: The basics more patients should know DISCLAIMER: Rational Vaccines (RVx) is providing this “Accurate Info for Patients” document as a resource to summarize (1) principles that define how HSV infections are controlled and (2) present options for the diagnosis, management, and prevention of genital HSV infections. Patients and doctors are individually responsible for how they choose to use this information. UPDATES: The “Accurate Info” portion of RVx’s website and this document will be updated quarterly based on feedback from doctors and patients. OVERVIEW: The Chief Science Officer of RVx, William P. Halford, has been studying the latency-replication balance of herpes simplex virus since 1991 (see Dr. Halford’s Biosketch). The document that follows is the net result of interweaving the (1) theoretical underpinnings of HSV’s in vivo biology (reviewed in Halford & Gebhardt, 2011) with (2) the perspective of genital herpes sufferers who experience disease symptoms more than 30 days per year. This document summarizes three areas of knowledge that may help herpes sufferers arrive at a better understanding of how to manage their symptoms and risk of HSV transmission. 1. The Biology of Herpes Simplex Virus (HSV) Infections. 2. The Relationship between Latent HSV Infections and Genital Herpes Disease. 3. Strategies to Manage Genital Herpes: Present and Future. OTHER RESOURCES: Beauman, 2007. Genital Herpes: A Review Warren, 2009. The Good News About the Bad News of Herpes: Everything You Need to Know 1. The Biology of Herpes Simplex Virus (HSV) Infections 1-A. Herpes Simplex Virus Serotype 1 vs 2 (HSV-1 vs HSV-2) HSV-1 and HSV-2 are two nearly identical viruses that share ~75 co-linear genes. HSV-1 and HSV-2 produce a similar spectrum of disease. The main difference between HSV-1 and HSV-2 is that they are two different serotypes of the same virus. Due to single amino-acid changes sprinkled through HSV-2’s 75 proteins (relative to HSV-1 proteins), HSV-2 has evolved the ability to superinfect people already infected with HSV-1. The use of multiple related serotypes to allow essentially the same microbe to infect humans more than once (and thus evade pre-existing immunity) is not unique to HSV; Streptococcus pneumoniae, rhinovirus (a cause of the common cold), and human papilloma virus each have >100 serotypes that are all biologically the same microbe, but which contain enough amino acid changes to side-step pre-existing immunity to other serotypes of the same microbe. In this document, the terms HSV-1 and HSV-2 will be used to denote specific viruses when relevant. However, because the biology of HSV-1 and HSV-2 infections are similar in principle, the term “HSV” will be used wherever possible to indicate that the principles under discussion are probably relevant to both HSV-1 and HSV-2. HSV-1 and HSV-2 both cause primary genital herpes. In some patient populations, HSV-1 is a more common cause of genital herpes than HSV-2. It has widely been stated that HSV-2 is the predominant cause of recurrent genital herpes, which most doctors take to mean that HSV-1 never, -1- Accurate Info for Patients Version 1.1 (Sept 2016) or only rarely, causes recurrent genital herpes. There is a dearth of evidence to support this sweeping conclusion that was made in the 1970s before we had the scientific means to fully vet the hypothesis. In the 21st century, HSV-1 appears to be the predominant cause of genital and neonatal herpes (Bernstein, et al, 2013; Jones, et al, 2014). Thus, HSV-1 is equally capable of productive replication in the genital tract and lower spinal ganglia as HSV-2, and likewise genital HSV-1 infections may be transmitted to a sexual partner or to a child during childbirth. The fact that many medical practitioners still believe HSV-2 is the only relevant cause of genital herpes is representative of the larger problem that doctors are too often working with outdated information. Being 80% right is still “wrong enough” to create serious problems with the decisionmaking process used to diagnose and manage genital herpes. 1-B. Primary HSV Infections. Viral replication is the process by which any human virus, including HSV, (1) enters cells in the body and (2) initiates a process of replication (amplification) that increases the number of viruses by 10- to 100-fold over the course of a few hours. The details of HSV replication in a single cell are too complex to warrant discussion here. However, the logic of the process is important. Like a computer virus, an actual virus is a piece of code, which in the case of HSV is a small piece of linear, double-stranded DNA that is about 150,000 base pairs long. For non-scientists, you can think of this as a book that is 75 pages long, where most pages have between 1,000 and 4,000 characters per page. In the context of HSV, each ”page” is called a viral gene and refers to one segment of the code. All of the characters in the “whole book” are called the HSV genome. Against that background, HSV replication proceeds, as follows: i. A small particle (virion) delivers the HSV genome into a cell, which is shown binding to the upper left corner of a single cell in the adjacent Figure. ii. The virion releases the whole HSV genome into the cell and this is carried to the nucleus (dark gray center). There a subset of 5 immediate-early (IE) genes make 5 IE proteins that start a cascade of events that lead to HSV replication, which is the equivalent of photocopying a whole book (the HSV genome) a few hundred times. iii. As the HSV genome is “photocopied,” the increasing numbers of HSV genomes encode more and more viral proteins (1 protein per viral gene), and the new viral proteins assemble around the new HSV genomes to form new infectious virions (particles). These virions are shed from the virus-infected cell and may spread within that person or may be transmitted to another person. To summarize, one infectious HSV virion enters one human cell and within 12 – 18 hours that cell may release up to 100 new infectious HSV virions that may either (1) spread to neighboring cells, propagating the infection, or may (2) be transmitted to another persion. iv. Returning to the scale of a person, this process allows (1) HSV to initially infect the skin of the penis (or labia, vaginal mucosa, or anus) and (2) within 24 hours hundreds of newly synthesized infectious HSV virions are able to infect nerve fibers in the skin and move back into the peripheral nervous system and throughout the infected person’s body. The site of the life-long HSV infection is not in the skin where the infection starts, but rather is in the ganglia (collections of nerve cell -2- Accurate Info for Patients Version 1.1 (Sept 2016) bodies) that emanate off the left and right side of the lower spine (top of red arrow in adjacent Figure). Transport of HSV genomes up nerve fibers from the skin to the ganglia is mediated by a process called retrograde axonal transport, which is akin to an HSV virion hopping on an escalator that carries it from the skin to the spine (depicted as red arrow in the adjacent Figure). Once HSV infection reaches the spine, a life-long infection is established in the sacral ganglia. Because of the rapidity of viral replication, initially microscopic HSV infections go from being undetectable to the human eye (i.e., asymptomatic) to detectable about 5 days after a transmision event. In 80% of cases of HSV infection, the innate immune system suppresses the infection and the person remains asymptomatic and unaware of the infection for the duration of their life. However, ~2% of HSV-infected persons will progress to a lifetime of genital herpes that recurs more than 4 times per year. Although “only 10% of HSV infections” cause overt herpes symptoms, 4 billion people are infected; >100 million people suffer with recurrent herpetic disease caused by HSV-1 or HSV-2. 1-C. Latent HSV Infections. Dr. Halford obtained his PhD for studies of persistent immune responses in HSV latently infected ganglia (Halford, et al, 1996), and invested more than a decade studying how ICP0 regulates HSV’s latency-replication balance (NIH grants that supported this work). A synopsis of the biology of latent HSV infections is presented, as follows: i. HSV latency is not as silent as most doctors have been led to believe. Simply because a patient does not exhibit external symptoms of active HSV disease, does not mean that subclinical HSV reactivation events are not in progress. To the contrary, 20 years of literature suggests subclinical HSV reactivations are a frequent (weekly) event where a single latently infected neuron (out of a pool of thousands) re-initiates productive HSV replication. Hence, 2% of the human population is shedding infectious HSV virions that may be transmitted to others on any given day. Most people shedding infectious HSV virions do not exhibit herpes symptoms at the time. ii. HSV latency may, in essence, be described as an equilibrium between the virus and host. The host immune system cannot destroy HSV-infected neurons because the virus downregulates (turns OFF) viral protein synthesis when CD8+ T cells approach tracts of HSV infected neurons. These T cells encircle (wall off) HSV-infected neurons and non-cytolytically suppress viral replication through the secretion of cytokines such as interferon- (reviewed in Halford & Gebhardt, 2011; illustrated above). iii. In persons who have HSV DNA in their spinal ganglia, the latent infection is stable and consists of a population of hundreds to thousands of HSV latently infected neurons. Each latently infected neuron may harbor >300 latent HSV genomes in the form of circular DNA molecules that have the potential to re-awaken (reactivate) when the correct stimuli are provided. A latent HSV -3- Accurate Info for Patients Version 1.1 (Sept 2016) infection cannot be “cured” by removing all of the thousands of copies of latent HSV DNA from the body, and patients should not be duped into believing this is a practical reality. Claims that latent HSV infections may be “cured” with homing endonucleases that destroy 100% of latent HSV genomes are not credible because they are inconsistent with the evidence. Such DNA cutting reactions typically occur with <10% efficiency under the best of conditions. Moreover, this low efficiency of HSV DNA cutting should only decrease in an intact animal or human patient. 1-D. Regulation of HSV’s Latency-Replication Balance. Scientists lack a detailed, mechanistic understanding of how HSV’s latency-replication balance is controlled. However, a general description of the relevant factors provides a framework for understanding the process. i. The HSV genome is arranged in discrete blocks of code known as regions, as illustrated in the Figure below. The unique-long (UL) and unique-short (US) regions are, in essence, a bag of 68 viral genes that predominantly encode machinery required for HSV replication. ii. The regions of the HSV genome that regulate HSV’s latency-replication balance (i.e., the ON-OFF switch) reside in two 15-kilobase repeated regions, RL and RS, that control the expression of 3 of the 4 viral IE regulatory proteins; namely, ICP4, ICP0, and ICP22. iii. The short-repeated (RS) regions encode ICP4, a viral IE protein that serves as HSV’s major transcriptional regulator, which is essential to either positively or negatively regulate HSV gene expression (i.e., the foundational hardware of the ON-OFF switch). iv. The long-repeated (RL) regions control HSV’s latency-replication balance. Two genes that influence the process are the latencyassociated transcripts (LAT) and infected cell protein 0 (ICP0). The adjacent L/ST and ICP34.5 genes play important roles as well. In simple terms, the available evidence suggests that (1) the L/ST-ICP34.5 genes may control the timing of HSV’s exit from productive replication in neurons; whereas (2) the LAT-ICP0 genes may control the maintenance and reactivation of latent HSV genomes. v. The ICP0 and ICP34.5 genes encode proteins that are essential for HSV to resist repression by the host antiviral response (i.e, the human interferon response). Hence, a simple view of HSV’s latency-replication balance, which is consistent with the available evidence, is that HSV’s capacity to alternate between being (1) interferon-resistant (ICP0 and ICP34.5 are expressed) and (2) interferon-sensitive (ICP0 or ICP34.5 fail to accumulate) may lie at the heart of how the HSV genome “chooses” between productive replication or latent infection in neurons in vivo (reviewed in Halford & Gebhardt, 2011). vi. During "latency,” HSV gene expression appears to be restricted to the regulatory regions in the RL and RS regions, such that a collection of regulatory gene products may maintain the latent state. Viral replication cannot proceed because the 68 HSV genes in the UL and US regions are silent. The HSV genome’s UL region appears to be insulated from transcriptional activity in the regulatory RL regions by blocks of GC-rich direct repeats. Such DNA-based “terminators” and virus-encoded “anti-terminators” that regulate RNA polymerase’s processivity (i.e., ability to “bulldoze” through terminators) lies at the heart of how phage regulates its equivalent of a latency-replication balance in E. coli. -4- Accurate Info for Patients Version 1.1 (Sept 2016) 1-E. Reactivation of Latent HSV Infections At the center of HSV’s latency-replication balance lies the ICP0 gene, which encodes the master regulator of this balance. ICP0 was first identified as a protein that transformed HSV’s major transcriptional regulator, ICP4, from a weak to a highly potent activator of viral mRNA synthesis. Accumulation of ICP0 causes the HSV genome to abruptly tip towards productive replication, whereas absence of ICP0 strongly favors establishment of a silent HSV infection. Anything that triggers ICP0 synthesis will promote reactivation of a latent HSV infection. Many of the stressors known to trigger HSV reactivation in animal models (ultraviolet light, hyperthermic stress, irritation of the site of primary HSV infection) have been shown to activate a rapid increase in ICP0 mRNA synthesis, which would tip HSV’s latency-replication balance towards reactivation. In the context of genital herpes, reactivation of latent HSV genomes residing in the sacral ganglia would create a new, active area of HSV replication in the lower spine (which might produce a backache). If this initial single-cell reactivation event were not suppressed by the immune system within the first 24 hours, new infectious HSV virions would be produced (as described in Section 1B) and would be returned to the epithelium via anterograde axonal transport (i.e., blue arrow in adjacent Figure). Within 3 to 4 days, if HSV replication were not suppressed in the skin, the n the ongoing spread of the reactivated HSV infection would manifest as an area of redness that would eventually progress to a lesion at the site innervated by the HSV latently infected nerve fiber that reactivated (e.g., the epithelium of the penis, labia, vaginal mucosa, or anus). Typically, 7 to 10 days of active viral spread would be required from the initial HSV reactivation event in a single neuron of the lower spine to progress to lesions the size of those pictured in the adjacent Figure. A critical concept that many doctors and patients miss is that HSV reactivation is not the same as recurrent herpetic disease. HSV reactivation occurs in a single HSV latently infected neuron and leads to the release of new infectious virions (per the scheme shown in Section 1B). Considering that a person may contain hundreds or thousands of HSV latently infected neurons distributed through ganglia of their lower spine, single-cell HSV reactivation events are likely occurring at least once per week in all HSV latently infected persons; even those who are asymptomatic. Most individuals mount an immune response that controls HSV reactivation events in the first 48 – 72 hours, and thus these individuals do not experience the later symptoms of herpetic disease. Those individuals who require 10 to 14 days to suppress a HSV reactivation event will (1) shed infectious virus from 3 to 5 days post-reactivation in the absence of symptoms and (2) will manifest areas of redness or open lesions after 6 days post-reactivation. In summary, HSV reactivation is a molecular event that occurs in a single cell, whereas recurrent herpes symptoms only become apparent 5 or more days later. The available evidence suggests that fewer than 5% of single-cell HSV reactivation events progress to what a well-trained doctor would recognize as the symptoms of recurrent herpes. -5- Accurate Info for Patients Version 1.1 (Sept 2016) 2. The Relationship between Latent HSV Infections and Genital Herpes Symptoms Over 3 billion people are infected with HSV-1, and HSV-1 is the predominant cause of genital herpes in younger age groups. Although many doctors are taught that HSV-2 is the primary cause of recurrent genital herpes, the evidence to support this supposition is limited at best. The literature of the past decade indicates that, in the 21st century, HSV-1 and HSV-2 are both significant causes of genital herpes. The most obvious functional difference between HSV-1 and HSV-2 is that (1) HSV-2 kills host cells more quickly (i.e., is more cytopathic) and (2) HSV-2 infection spreads cell-tocell more rapidly than HSV-1. It would appear HSV-2 has evolved these more aggressive traits to allow it to efficiently superinfect persons already infected with HSV-1. The severity of primary HSV infection can be hugely influenced by two variables: - trauma to epithelium at time of HSV transmission (Fig. 1 of Halford, et al., 2004) - immune status at the time of primary HSV infection (Fig. 6 of Halford, et al., 2005) Examples of the first principle include women who have had a “Brazilian” pubic hair removal just prior to contracting HSV and men who shave over primary herpes lesions. In both cases, a compromised epithelial barrier promotes more severe herpetic disease. As the duration of primary HSV infection increases, the risk of recurrent herpetic disease increases. Primary genital herpes may last as long as 2 months with frequent recurrences spanning the first year. In contrast, 80% of primary HSV infections are so brief that no symptoms are noted. The duration of the primary infection will be proportional to (1) the number of HSV latently infected neurons colonized in the lower spine and (2) the copy number of latent HSV genomes an individual carries for the remainder of their life. This “viral DNA load” may vary widely from person-to-person, and may range from less than 1,000 to >1,000,000 copies of the latent HSV genome. As the reservoir of HSV latently infected neurons increases, so do the odds of recurrent herpetic disease. Among the greatest challenges for clinicians in diagnosing herpetic disease is that HSV infections may produce a wide variety of symptoms. Medical textbooks tend to emphasize “typical” herpes symptoms, but less than 20% of HSV-infected persons will present with these symptoms. Likewise, only a subset of patients with recurrent genital herpes will have the “typical” 4 outbreaks per year. Patients who are latently infected with HSV may suffer from recurrent herpes symptoms that impacts them anywhere from 0 - 100% of the days in any calendar year. Rules are only useful when they are applicable most of the time. With recurrent genital herpes, it is simply not useful to think in terms of a “median case of herpes,” because 80% of HSV infections are completely asymptomatic and 1-2% are far more chronic and debilitating than the “typical” presentation. Clinicians should think of recurrent genital herpes as being highly variable in (1) frequency of outbreaks, (2) duration of outbreaks, and (3) spatial extent of skin symptoms (localized or widespread across more than one dermatome). Additionally, patients may exhibit symptoms that are more internal than external in nature, such as chronic herpes-induced neuralgia. The clinical presentation of herpes zoster provides some context for considering what is possible. HSV-1 and HSV-2 tend to cause more localized symptoms at any one point in time, but patients’ symptoms may alternate between the genitalia, buttocks, thighs, and/or anus (areas innervated by the sacral ganglia). The review of Beauman, 2007 considers some “atypical” presentations of genital herpes. -6- Accurate Info for Patients Version 1.1 (Sept 2016) Patients who experience the most protracted primary HSV-1 or HSV-2 infections are at the greatest risk for having high-level complications associated with recurrent genital herpes, including (1) chronic neuropathic pain and/or (2) multiple sites of HSV recurrences that rotate from the left and right sides of the body. The latter symptoms indicate that latent HSV infections were established in multiple spinal ganglia. Many so-called “atypical” herpes symptoms make a great deal of sense if one understands the theoretical underpinnings of the biology of HSV infections. --------------------------------------------------------------------------------------------------------------------- 3. Strategies to Manage Genital Herpes: Present and Future The biology of latent HSV infections is presented above in terms of an equilibrium model, which effectively reduces to three points: 1. When viral activators accumulate in HSV-infected neurons, the virus overcomes interferon (host)-induced repression and active replication occurs. 2. When viral activators fail to accumulate, HSV replication in neurons is suppressed by the host immune response. 3. Most HSV reactivation events do not appear to kill their host neurons. Hence, the reservoir of latently infected neurons does not shrink over time, and most sufferers experience their outbreaks at the same site over and over again because the same neurons repeatedly support reactivation events. Below, the factors that influence recurrent genital herpes are described in the same terms. In essence, HSV reactivation is like an idling car that is temporarily stopped. There are two options to get it moving. You can (1) punch the gas to overpower the brakes (i.e., make more viral activators) or (2) release the brakes so the car starts rolling (i.e., compromise immune control of HSV). Triggers of HSV reactivation either i. increase production of viral activators; ii. interfere with host immune control of HSV; or iii. both. 3-A. Avoidance of HSV Triggers. Triggers include activities that increase levels of stress-related hormones, such as cortisol, or sunburn, local irritation of sites where herpes outbreaks occur, or damage to the HSV latently infected nerve fibers (e.g., a back injury). In animal models, such triggers tend to drive increased production of the viral IE activator protein ICP0, which promotes reactivation. Alternatively, triggers may dampen the host immune response that controls a latent HSV infection. Examples include alcohol consumption, anemia, systemic fever, or the progesterone spike that precedes menstruation. Additionally, many foods trigger herpes outbreaks in sufferers such as peanuts, chocolate, and coffee which have the potential to (1) drive expression of viral activators (particularly stimulants like coffee) and/or (2) trigger food allergies that would alter immune function. Knowing and avoiding activities that trigger herpes outbreaks is a simple strategy used by many herpes sufferers to reduce the frequency of their symptoms. 3-B. Pros and Cons of Acyclovir-Like Drugs. Acyclovir was developed in the 1970s, and functions as a chain terminator of viral DNA synthesis in HSV-infected cells. Although it is efficient at blocking HSV replication in a laboratory setting, acyclovir’s efficacy in patients is limited by its poor solubility, and oral acyclovir is additionally limited by poor absorption from the gut. Valacyclovir and famciclovir are related drugs that have the same mechanism of action, -7- Accurate Info for Patients Version 1.1 (Sept 2016) but which are slightly more soluble. In patients with recurrent genital herpes, acyclovir-like drugs may be taken episodically as needed to shorten the duration of herpes outbreaks. However, for this to be effective, the drugs must be taken at the earliest sign of the prodromal symptoms (nerve tingling or pain) that precedes an outbreak. Alternatively, some patients are placed on daily suppressive therapy to control their herpes outbreaks with acyclovir-related drugs. For some patients, daily antiviral drugs are effective, but for many this is not the case. In two studies in 1988, it was shown that patients who took daily acyclovir prophylactically exhibited a decrease in HSV-specific antibody levels. For others, acyclovir-related drugs may decrease the duration of skin symptoms, but are ineffectual in preventing the pain and tingling sensations (neuralgia) that accompany recurrent genital herpes. HSV-infected persons should absolutely consider acyclovirrelated drugs to manage their disease. However, patients should be realistic that acyclovir-related drugs are not effective for controlling 100% of herpes symptoms in 100% of patients. 3-C. Pritelivir: A Better Antiviral Drug? In 2016, the first new class of anti-herpesviral drugs appears to be close to reaching U.S. markets. This drug, pritelivir, functions as a helicase-primase inhibitor of HSV replication. The chemical structure and mechanism of action of pritelivir are completely unrelated to acyclovir-related drugs. Therefore, it is possible that combinations of pritelivir and acyclovir-related drugs may be more effective than either drug alone. Initial clinical trial results suggest pritelivir would be vastly superior to acyclovir-based antiviral drugs in terms of its capacity to reduce herpes symptoms and the frequency of shedding of infectious HSV-2 virions (Wald, et al, 2014). However, it remains unclear when pritelivir will be available to the public. Side-by-side comparative studies will be needed to determine if, in fact, pritelivir is more effective for managing genital herpes than acyclovir-based drugs. 3-D. Why Better Herpes Treatment Options Are Needed. The current strategies medical professionals rely upon to diagnose, manage, and prevent herpetic disease are in many ways outdated. Recent advances in the understanding of the in vivo biology of HSV infections may be exploited to yield better solutions, as opposed to relying upon acyclovir-based antiviral drugs. Antiviral drugs may be improved upon, but the past 20 years of experience with acyclovirrelated drugs suggest that antiviral drugs alone are insufficient to stop the epidemic spread of HSV infections from 4 billion carriers to >1 million uninfected persons every week. If antiviral drugs were effective at preventing the spread of HSV infections, this should have been obvious by 2005. However, to date, antiviral drugs have not curbed the rate of HSV-1 or HSV-2 transmission from HSV latently infected carriers to naïve individuals. At RVx, we believe better herpes solutions are possible today, and recommend the following changes, which might improve the management and prevention of genital herpes: 1. Accurate Diagnosis and Prophylactic Vaccines for Discordant Couples. The host immune response always serves as “the brakes” that restricts the spread of HSV. If genital herpes patients are accurately diagnosed with HSV-1 versus HSV-2 genital herpes, then patients with HSV-1 genital herpes may reduce the risk of sexual transmission by entering into a relationship with the >50% of the population who already carry HSV-1. Alternatively, an effective prophylactic HSV-1 or HSV-2 vaccine offered to a seronegative partner would greatly reduce the risk of transmission of herpetic disease. 2. Proper management of genital herpes. Many doctors have been misled to believe that management of genital herpes should focus exclusively on HSV (the virus). This approach does not adequately consider the in vivo biology of HSV infections, which indicates that latent HSV infections exist in an equilibrium that is controlled both by a gas pedal (the -8- Accurate Info for Patients Version 1.1 (Sept 2016) virus) and a braking system (the host immune response). If an antiviral drug is effective, this will interfere with the virus replication (amplification) required for a HSV reactivation event to progress to a recurrent herpes lesion. While this is sometimes helpful, ongoing, subclinical HSV reactivation events may be required to keep the adaptive immune system (antibodies and T-cells) adequately engaged in the active control of HSV replication. Hence, patients often observe that while antiviral drugs may initially help control their symptoms for 3 to 6 months, HSV-antibody levels (and likely HSV-specific T-cells) are not maintained when patients take antiviral drugs every day. If the host immune response becomes ineffective (no brakes), herpes sufferers note that the antiviral drugs “lose their potency” and their recurrent herpes symptoms return. Learn more about how daily antiviral drug suppression often erodes HSV antibody levels in patients. 3. Therapeutic HSV-2 vaccines: an underexplored treatment modality. The immune system explains why (1) 80% of HSV infections are asymptomatic; (2) HSV infections are devastating in newborns whose immune systems are under-developed; and why (3) HSV infections progress to fatal outcomes in interferon-deficient individuals. The possibility that the adaptive immune system may be “misfunctioning” (tolerized) in recurrent herpes sufferers has not been carefully investigated. Clonal exhaustion of T cells is known to occur when foreign antigens, like HSV proteins, are chronically present (Wherry and Kurachi, 2015). The underlying cause of recurrent genital herpes in many sufferers may reduce to “tolerization” of the adaptive immune system to HSV’s foreign proteins, which would severely compromise immune control of latent HSV infections. Therapeutic HSV-2 vaccines, such as the Agenus HerpV or Genocea GEN-003 vaccines, are being considered as a new treatment modality to break this potential stalemate of “tolerance to HSV-2 immunogens.” However, like many failed HSV-2 subunit vaccines, the GEN-003 and HerpV therapeutic HSV-2 vaccines only expose recipients to 2% of HSV-2’s potential immunogens. At RVx, we believe that the TheravaxHSV-2 vaccine is far more likely to yield an effective therapeutic HSV-2 vaccine because it encodes up to 99.3% of HSV-2’s potential antigens. Clinical trials to test this concept are imminent. 3-E. Why genital herpes is most likely a vaccine-preventable disease. In recent years, biomedical researchers have attempted to develop “subunit vaccines” to prevent genital herpes, AIDS, and other infectious diseases. Subunit vaccines typically contain less than 2% of HSV-2’s antigens, and are based on the premise that one small piece of HSV-2 may serve as an effective vaccine. To date, all HSV-2 subunit vaccines tested in clinical trials have failed to prevent genital herpes. RVx believes that our different approach, which uses rationally-engineered live vaccines that retain 99% of HSV’s potential antigens, will be sufficient to end the herpes epidemic. Live viral vaccines re-create every facet of a microbe’s life cycle, and fully prepare the human immune system to do battle with the natural pathogen. Live viral vaccines have been used to prevent the viral diseases of (1) smallpox, (2) yellow fever, (3) polio, (4) mumps, (5) measles, (6) rubella, and (7) chickenpox. Never once, in the history of medicine, has a live-and-appropriately-attenuated viral vaccine failed to stop the spread of its corresponding disease in the human population. RVx’s ProfavaxHSV vaccines offer a similar opportunity to eradicate all forms of herpetic disease. -9-